Diadetic foot M Pourafkari Shahid Beheshti University of


Diadetic foot M. Pourafkari Shahid Beheshti University of medical science Taleghani Hospital Radiology Department marina@ams. ac. ir

Diabetic foot infections are associated with significant morbidity, account for the largest number of diabetes-related hospital bed days and contribute to 50% of all lower extremity amputations in the United States.




Plain Radiography Initial procedure for imaging suspected osteomyelitis in the diabetic patient. Characteristic signs of osteomyelitis on plain radiograph include focal loss of trabecular pattern, periosteal reaction and frank bone destruction. Plain radiographs can also reveal presence of foreign bodies, gas in soft tissues, fractures or bony abnormalities. Poor sensitivity (22 -75%) as osteomyelytic changes are delayed for 10 -21 days following infection. 30 -50% loss of bone density is required before a radiograph will demonstrate osteomyelitis. False positive results may be found in patients with neuroarthropathy (Charcots arthropathy).



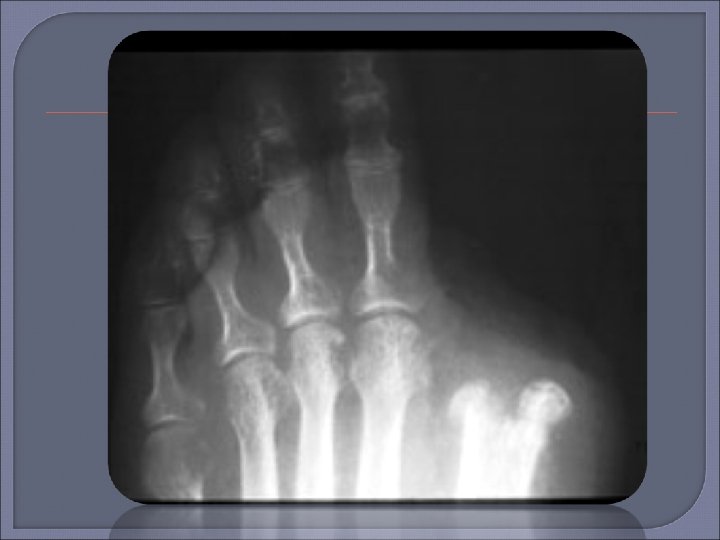
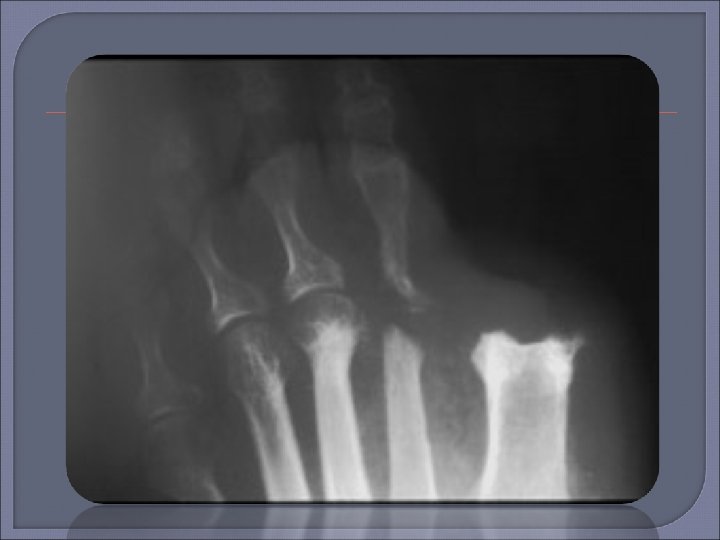



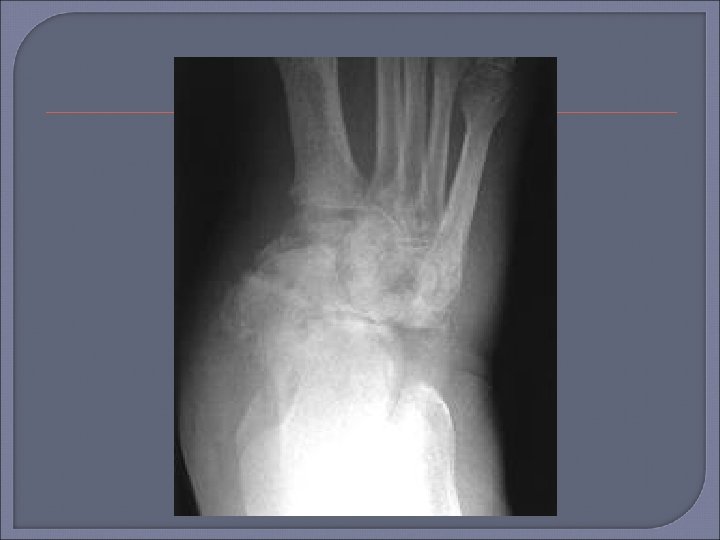

Plain film x-ray should be the first imaging examination for suspected osteomyelitis in the diabetic foot. If the initial x-ray is negative, the absence of osteomyelitis can be confirmed by repeat examination 2 -4 weeks later. MRI can be useful if x-ray images are equivocal or if there is concern for soft tissue infection.





After initial radiography, MR imaging is the modality of choice for the evaluation of pedal osteomyelitis and soft-tissue infection, with sensitivity of 90% and specificity of 83%. Magnetic resonance (MR) imaging allows preoperative mapping of the extent of infection and thus may help minimize the area of resection.

T 1 -weighted imaging has the highest specificity for the detection of osteomyelitis. In addition, T 2 -weighted fat-suppressed imaging is recommended to detect changes in bone marrow and adjacent soft tissue.

The simplest method to determine whether osteomyelitis is present is to track the ulcer or sinus tract down to bone at MR imaging and evaluate the signal intensity of marrow: Noticeably low signal intensity on T 1 -weighted images is a primary sign of osteomyelitis.
, T 2 -weighted (b), and gadolinium-enhanced T 1 -weighted")
Sagittal T 1 -weighted (a), T 2 -weighted (b), and gadolinium-enhanced T 1 -weighted fatsuppressed (c) MR images show that the marrow in the tip of the great toe (arrowhead) has low signal intensity on the T 1 -weighted image; has high signal intensity on the T 2 -w. . . Donovan A , Schweitzer M E Radiographics 2010; 30: 723736 © 2010 by Radiological Society of North America
, T 2 -weighted (b), and gadolinium-enhanced T 1 -weighted")
Sagittal T 1 -weighted (a), T 2 -weighted (b), and gadolinium-enhanced T 1 -weighted fatsuppressed (c) MR images show that the marrow in the tip of the great toe (arrowhead) has low signal intensity on the T 1 -weighted image; has high signal intensity on the T 2 -w. . . Donovan A , Schweitzer M E Radiographics 2010; 30: 723736 © 2010 by Radiological Society of North America
, T 2 -weighted (b), and gadolinium-enhanced T 1 -weighted")
Sagittal T 1 -weighted (a), T 2 -weighted (b), and gadolinium-enhanced T 1 -weighted fatsuppressed (c) MR images show that the marrow in the tip of the great toe (arrowhead) has low signal intensity on the T 1 -weighted image; has high signal intensity on the T 2 -w. . . Donovan A , Schweitzer M E Radiographics 2010; 30: 723736 © 2010 by Radiological Society of North America

In cases in which the bone marrow is hyperintense on T 2 -weighted images but is not hypointense on corresponding T 1 weighted images, osteitis is more likely than osteomyelitis, even when bone marrow enhancement is present.

Osteitis in a patient who underwent transmetatarsal amputation. Donovan A , Schweitzer M E Radiographics 2010; 30: 723736 © 2010 by Radiological Society of North America

Osteitis in a patient who underwent transmetatarsal amputation. Donovan A , Schweitzer M E Radiographics 2010; 30: 723736 © 2010 by Radiological Society of North America

The criteria for diagnosing osteomyelitis at the site of amputation are the same as those for patients who have not undergone amputation. However, in patients who undergo débridement instead of amputation, associated postoperative edema may occur at the surgical site and should not be mistaken for osteomyelitis. Surprisingly, most patients who undergo amputation have little postoperative bone marrow edema.

Osteomyelitis in a patient who underwent a partial calcaneal resection. Donovan A , Schweitzer M E Radiographics 2010; 30: 723736 © 2010 by Radiological Society of North America

At MR imaging, a skin callus appears as a focal infiltration or mass within subcutaneous fat, with low signal intensity on T 1 -weighted images and low to intermediate signal intensity on T 2 -weighted images. After the administration of contrast material, callus enhancement may be mistaken for a softtissue infection; a typical location and lack of adjacent soft-tissue change should help distinguish callus formation from infection.

Skin callus. Donovan A , Schweitzer M E Radiographics 2010; 30: 723736 © 2010 by Radiological Society of North America

Skin ulcer associated with osteomyelitis. Donovan A , Schweitzer M E Radiographics 2010; 30: 723736 © 2010 by Radiological Society of North America

Skin ulcer associated with osteomyelitis. Donovan A , Schweitzer M E Radiographics 2010; 30: 723736 © 2010 by Radiological Society of North America

Calcaneal ulcers and sinus tract associated with osteomyelitis. Donovan A , Schweitzer M E Radiographics 2010; 30: 723736 © 2010 by Radiological Society of North America

Abscess in a patient who underwent transmetatarsal amputation. Donovan A , Schweitzer M E Radiographics 2010; 30: 723736 © 2010 by Radiological Society of North America

Abscess in a patient who underwent transmetatarsal amputation. Donovan A , Schweitzer M E Radiographics 2010; 30: 723736 © 2010 by Radiological Society of North America

Abscess in a patient who underwent transmetatarsal amputation. Donovan A , Schweitzer M E Radiographics 2010; 30: 723736 © 2010 by Radiological Society of North America

Neuroarthropathy with superimposed osteomyelitis. Donovan A , Schweitzer M E Radiographics 2010; 30: 723736 © 2010 by Radiological Society of North America

— 67 -year-old diabetic man with nonhealing ulceration of left calf. Lapeyre M et al. AJR 2005; 185: 1641 -1650 © 2005 by American Roentgen Ray Society

— 48 -year-old man with nonhealing ulceration of left calf. Lapeyre M et al. AJR 2005; 185: 1641 -1650 © 2005 by American Roentgen Ray Society

- Slides: 54