Diabetic Retinopathy Screening in Scotland Roderick Harvey DRS

Diabetic Retinopathy Screening in Scotland Roderick Harvey DRS Lead Clinician

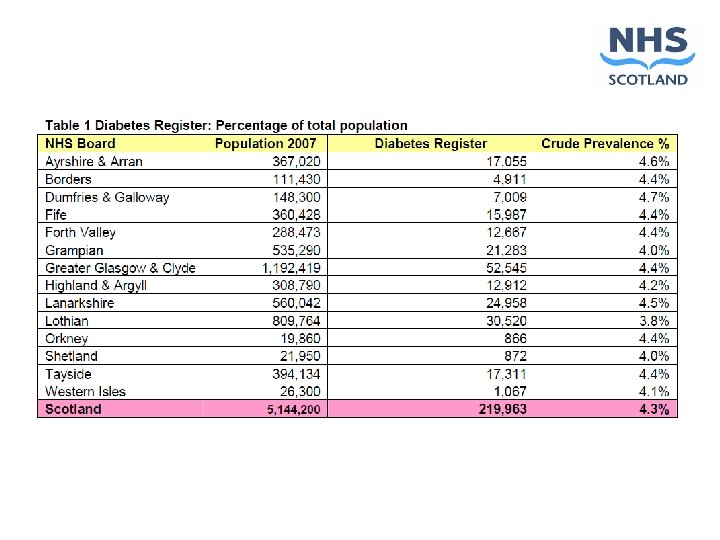
Population 5, 144, 200

The national programme l White paper 2000 l Commitment to develop a Scottish Diabetes Framework l “The framework will include plans to establish a national screening strategy for diabetic retinopathy”

HTBS Report 2002 l Aim – detection of sight threatening diabetic retinopathy l Screening modalities w Primary - digital retinal photography w Secondary - slit lamp biomicroscopy

Benefits of photographic screening l High sensitivity and specificity for sight threatening disease l Ease of image acquisition, storage and transmission l The opportunity for quality assurance through double reading l Cost effectiveness

Publications

NHS QIS DRS Standards l Screening delivered to a defined specification l 80% of eligible people screened per year l 100% of eligible people invited per year l Call & recall in place using national software l Arrangements for hard to reach groups l Staff trained and qualified (or under supervision) l Quality assurance is in place

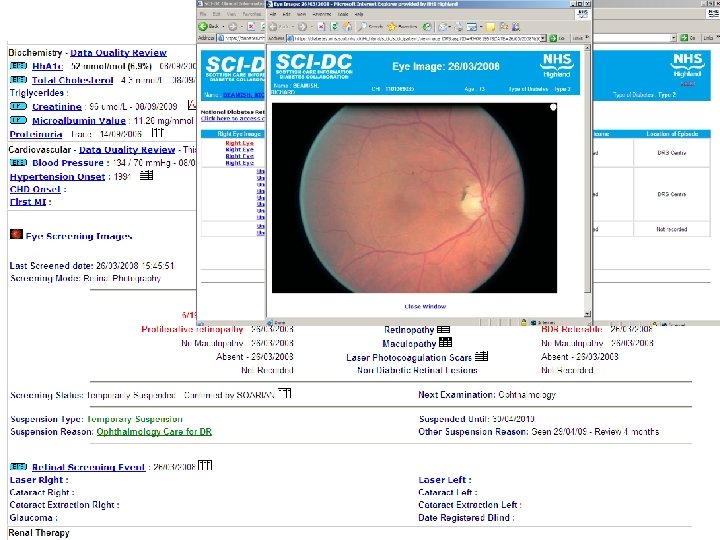
Special features l Single field macular centred image l Mydriasis only if initial image of inadequate quality

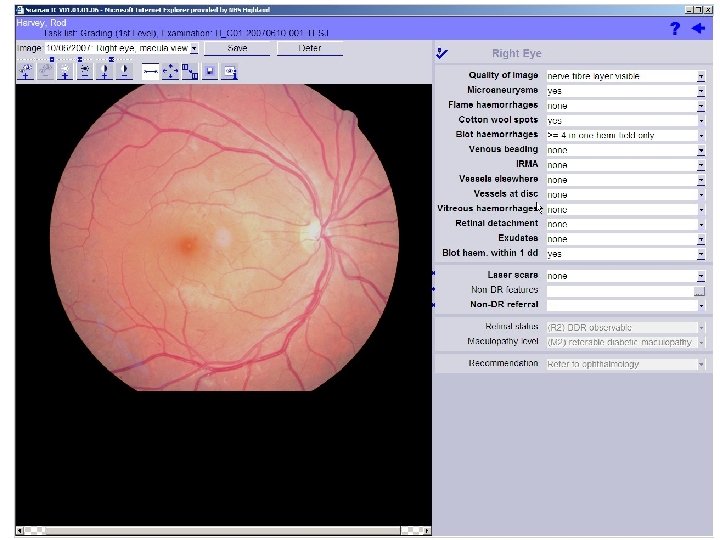
Grading l Feature based l Software calculates final grade according to grading algorithm l Outcome determined automatically l All graders perform full grading w Level 1 final grade normals only w Level 2 final grade non referrable w Level 3 final grade all referrable
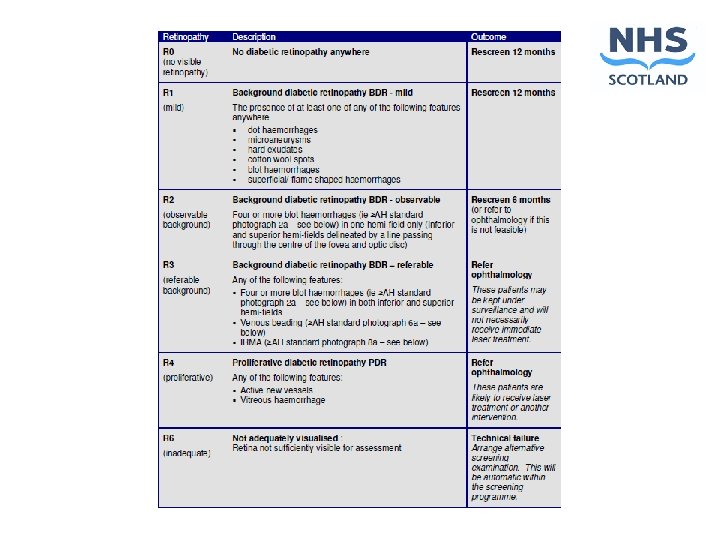
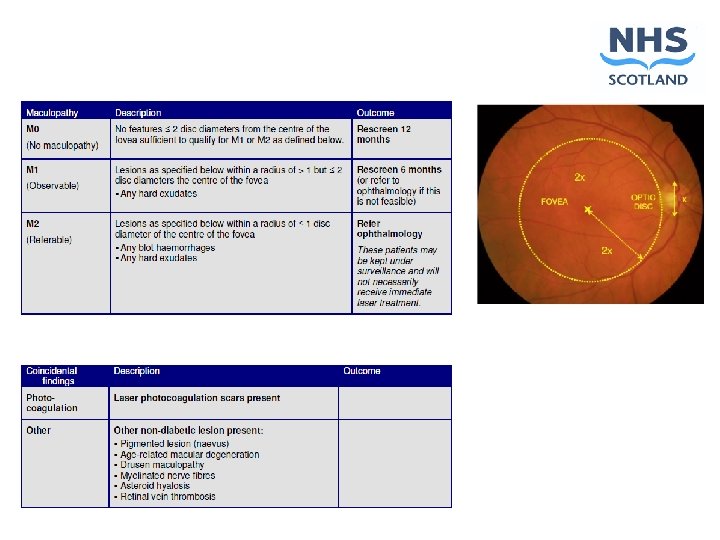

Outcomes Re screen 12 months R 0 or R 1 M 0 Re screen 6 months R 2 or M 1 Refer ophthalmology R 3 or above, or M 2 Non diabetic lesions Technical failure R 6 – inadequate image

Quality assurance l All L 1 & L 2 graders have 500 image pairs per year regraded randomly by L 3 grader l External QA of images under development w 1 st round of pilot completed 2008 l External QA of programmes w Standardised annual report template w National Key Performance Indicators

Training & Accreditation l City & guilds Level 3 Certificate in Diabetic Retinopathy Screening l 140 people in Scotland registered l 110 modules passed l Slit lamp examiner standards and accreditation process defined

The Scottish National DRS Programme l Responsibility for screening lies with the fourteen individual Health Boards l Within each Board the programme is delivered to common standards defined by w NHS QIS standards on DRS w Policies developed by the DRS Collaborative w Constraints embedded in the national DRS software l National software for photography, administration and grading

The Board Programmes are all members of a formal DRS Collaborative SGHD SDG NSD IT Board NSD PFIG DRS IT Board SCI-DC Executive Group Board Co-ordinators Clinical Group Short-life groups As required Service Management IT Users Group

Implications of franchise model l Adherence to national standards l Sharing of a national database of eligible patients l Ability to tailor the details of the delivery of the screening programme to suit local needs w Fixed site photography w Mobile units w Image capture through optometrists

Eligible population l All people resident in Scotland with confirmed diabetes l Aged 12 years or older l Not under the care of an ophthalmologist for treatment of diabetic retinopathy l Not suspended for a valid clinical or organisational reason (excludes temporarily unavailable)

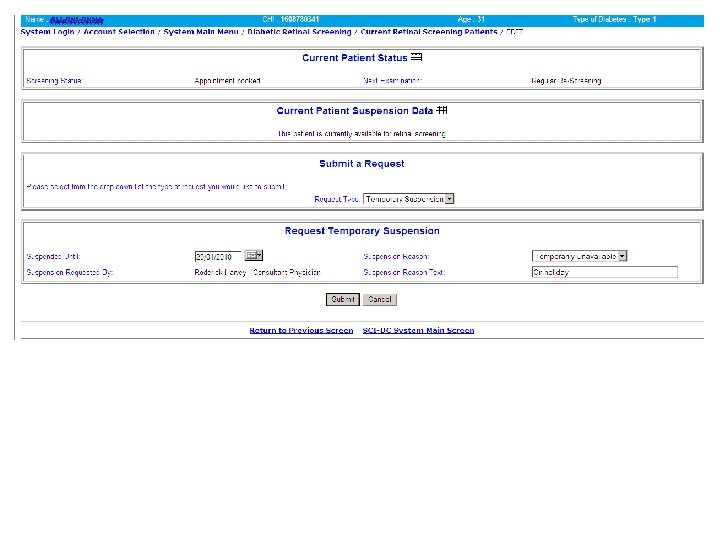
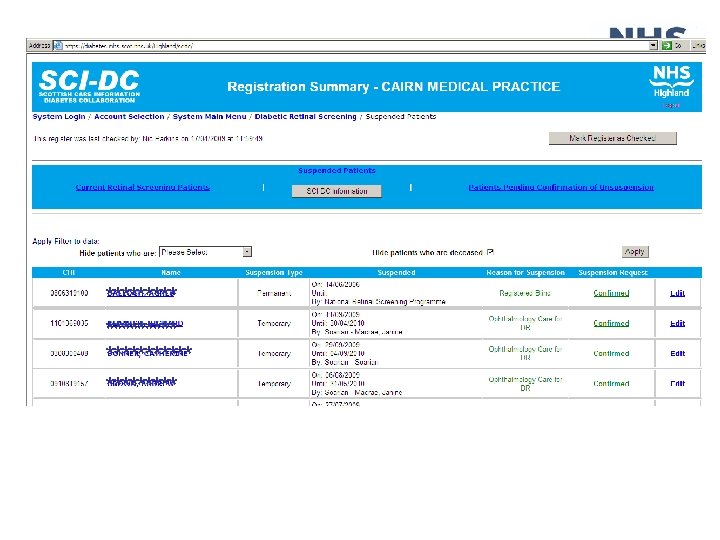
Suspensions Suspension Reason Suspension Type Who suspends and can unsuspend Informed choice to opt out Temporary GP Under Age Temporary System Total Loss of Vision Permanent GP as advised by Ophthalmologist Terminal Illness Temporary GP Disabilities: Learning, Mental or Physical Temporary or Permanent GP Under the care of an Ophthalmologist Temporary Retinal Screening Administrator as advised by Ophthalmologist Temporarily Unavailable Temporary GP or Retinal Screening Administrator Deceased Temporary Permanent GP System Not Diabetic Permanent GP or other HCP Not Permanently Resident in Scotland Permanent System

How is it all put together

Maintenace of the eligible population l Recording of diabetes in a primary care system automatically registers the patient for DRS l Dynamic link with SCI-DC and the CHI ensures that the population is accurately maintained l Registration can also be done directly through SCI-DC or Soarian l Suspensions are managed through SCI-DC and Soarian

SCI-DC Consortia server CHI Staging Server Soarian EMIS XML Messages Vision GPASS SCI-DC Mobile Admin Fixed

How are we doing

Total living diabetic population 239, 495 Eligible population 204, 817

Invitation rate 93. 2% Attendance rate 77. 0% Successful screening rate 73. 7%

Overall Referable 3. 5% Observable 1. 9% Tech failure 7. 6%

Challenges

Slit lamp examination l About 8% of patients require slit lamp examination l Training & accreditation requirements defined l Difficulty for small and dispersed boards in meeting the requirements

Optometry l Most optometrists now have digital retinal cameras l Photography is part of GOS contract for over 60 s l Opportunities for synergy and image capture by optometrists l Challenges of integration with board wide screening programmes without compromise of quality standards on grading l Framework for optometry image capture is being piloted in two health board regions

Ophthalmlogy l Closing the loop l Capturing outcome of ophthalmology consultations l Ensuring appropriate suspension of patients under the care of ophthalmology l Failsafe to track ophthalmology referrals l Capacity

Quality assurance l Need for more robust analysis of internal QA performance across all health boards l Need to establish regular external QA image sets and define reporting formats

Future Automated Grading

Start Yes Image of adequate quality? No Refer to Level 2 Manual Grader Yes Microaneurysms present? No Final Grade R 0 M 0

Automated Grading l 6732 patients using gold standard grading for actionable retinopathy w Automated grading 97. 9% w Routine manual 99. 1% l 33, 535 patients from the Scottish DRS service the performance of automated grading for actionable retinopathy was w Sensitivity 99. 1% w Specificity 59%

Automated grading l DRS Collaborative commissioned an independent review of the performance of automated lesion detection software l Four patients from 33535 (0. 012%) may have missed clinically relevant maculopathy l Cost to detect these patients in Scotland £ 275, 000 pa l Conclusion that it should be used for DRS programme in Scotland

Thank you for you attention
- Slides: 45