DIABETIC RETINOPATHY DIABETIC RETINOPATHY Definition Epidemiology Risk Factors

DIABETIC RETINOPATHY

DIABETIC RETINOPATHY • • • Definition. Epidemiology. Risk Factors. Pathogenesis. Signs & Symptoms. Classification. Investigations. Complications. Management.

Diabetic eye disease refers to a group of eye problems that people with diabetes may face as a complication of diabetes. All can cause severe vision loss or even blindness. Diabetic retinopathy - most common cause of blindness between ages 20 and 70 years.

Diabetes is associated with the following ocular events : • Corneal abnormalities. • Glaucoma ( rubeotic glaucoma ). • neovascularization. • Cataracts… snowflake retinopathy in younger pts and greater frequency and earlier onset of age related cataract. • Neuropathies. • Diabetic Retinopathy.

Diabetic retinopathy causes retinal vascular disease. Other causes of RVD : - Hypertensive retinopathy. - sickle cell retinopathy. - Retinopathy of prematurity. - central and branch retinal artery occlusion. - Central and branch retinal vein occlusion. - Abnormal retinal blood vessels.

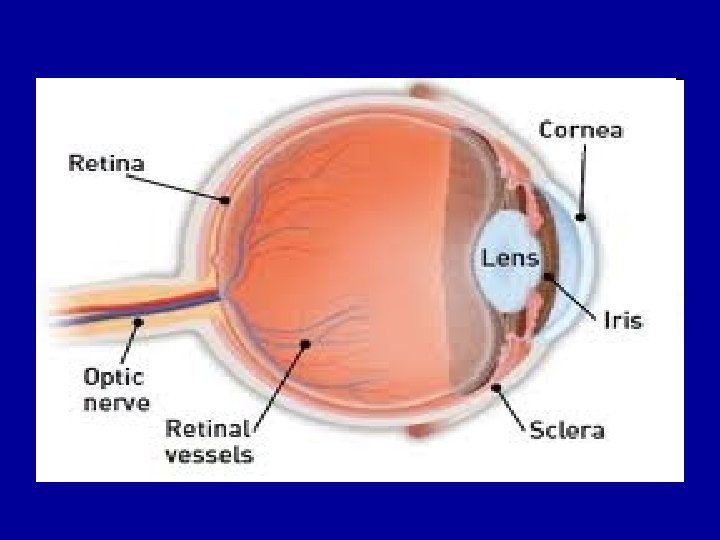
The Retina • What is Retina? Structure that lines the inside of the globe behind ora serrata. • 2 major layers: - Inner neurosensory retina (NSR): transparent, light sensitive membrane. - Outer retinal pigment epithelium (RPE). • Retinal blood supply: From central retinal artery and choroidal circulation.

Retinal Histology Sclera Outer Plexiform layer Choroid Bipolar cells RPE Photoreceptor outer segments Inner plexiform layer Ganglion cells Photoreceptor inner segment Nerve fiber layer

Retinal Anatomy
 loss of insulin secretion mostly in young people.")
• - DM 1 (IDDM) loss of insulin secretion mostly in young people. . Onset is relatively acute and retinopathy begins to appear about 5 years after onset. • - DM 2 (NIDDM) pt may retain some insulin secretion but develop resistance to its action. It occurs in older age group. • Bcoz DM 2 present several yrs prior to diagnosis, retinopathy may be found at predentation.

RISK FACTORS: 1. Duration of diabetes 2. Poor control of Diabetes 3. Hypertension 4. Nephropathy 6. Obesity and hyperlipidemia 7. Smoking 8. Pregnancy

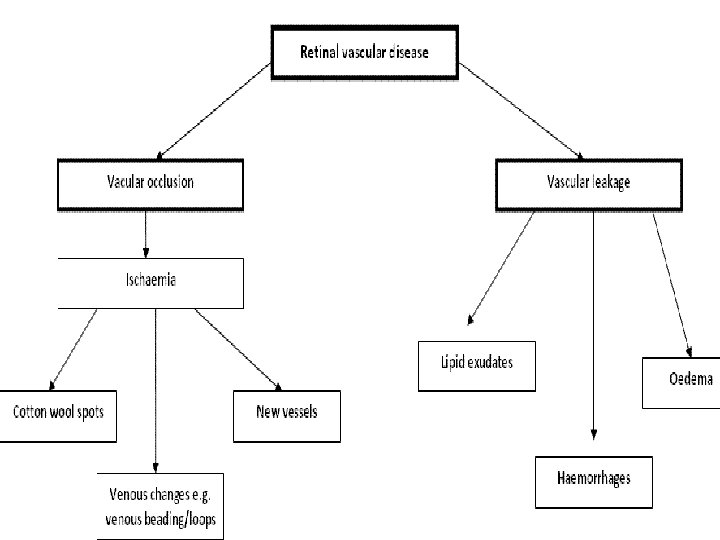
Pathogenesis ØMicroangiopathy which has features of both microvascular leakage and occlusion

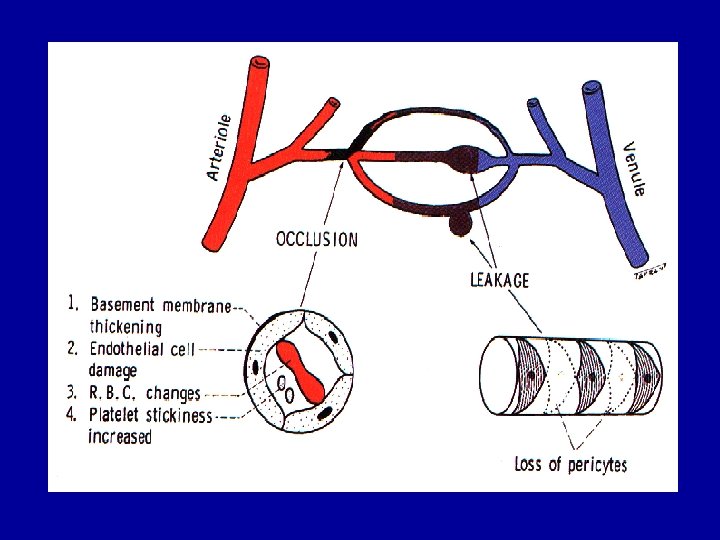
Microvascular leakage Ø Loss of pericytes results in distention of weak capillary wall producing microaneurysms which leak. Ø Blood-retinal barrier breaks down causing plasma constituents to leak into the retina – retinal oedema, hard exudates

Microvascular occlusion Ø Basement membrane thickening, endothelial cell damage, deformed RBCs, platelet stickiness and aggregation Ø Vascular Endothelial Growth Factor (VEGF) is produced by hypoxic retina Ø VEGF stimulates the growth of shunt and new vessels

Pathogenesis : Too much sugar in your blood can damage the tiny blood vessels (capillaries) that nourish the retina. This can result in diabetic retinopathy and vision loss. Elevated blood sugar levels can also affect the eyes' lenses. With high levels of sugar over long periods of time, the lenses can swell, providing another cause of blurred vision.

Response to Hypoxia: • More extensive retinal hypoxia triggers compensatory mechanisms within the eye to provide enough oxygen to tissues: • • Venous caliber abnormalities, such as • venous beading, loops, and dilation. • Intraretinal microvascular abnormalities (IRMA) represent either new vessel growth or remodeling of preexisting vessels through endothelial cell proliferation within the retinal tissues to act as shunts through areas of nonperfusion.

• Further increases in retinal ischemia trigger the production of vasoproliferative factors : – neovascularization at border of perfused and unperfused => fragile &highly permeable vessels. These delicate vessels are disrupted easily by vitreous traction, which leads to hemorrhage into the vitreous cavity or the preretinal space. – Fibrovascular changes & traction => retinal edema, retinal heterotropia and retinal detachments.

History – symptoms it's possible to have diabetic retinopathy and not know it. In fact, it's uncommon to have symptoms in the early stages of diabetic retinopathy. As the condition progresses, diabetic retinopathy symptoms may include: • Spots or dark strings floating in your vision (floaters) • Blurred vision • Fluctuating vision • Dark or empty areas in your vision • Poor night vision • Impaired color vision • Vision loss • Diabetic retinopathy usually affects both eyes.

Simulation of defective vision as experienced by a Diabetic whose vision has been affected by Diabetic retinopathy Normal Defective
. – Earliest clinical")
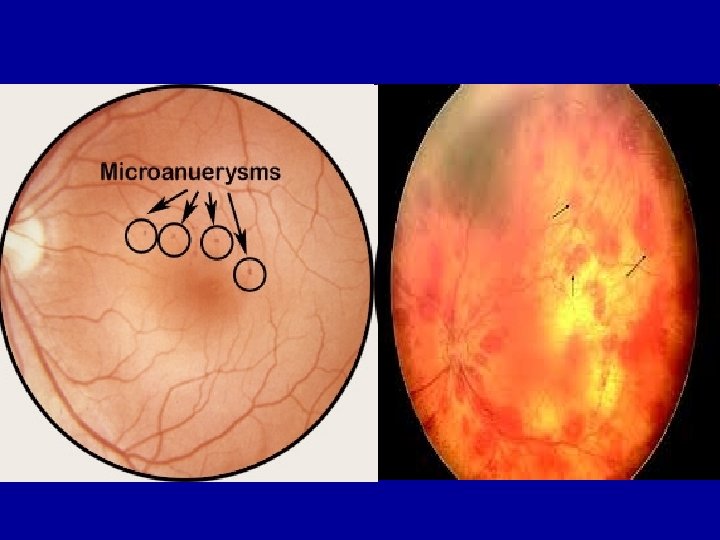
Signs on Examination: • Microaneurysms (Earliest , red or yellowish dots). – Earliest clinical sign of diabetic retinopathy – Secondary to capillary wall outpouching due to pericyte loss – Appear as small red dots in the superficial retinal layers – Fibrin and RBC accumulation in the microaneurysm lumen – Rupture produces blot/flame hemorrhages – May appear yellowish in time as endothelial cells proliferate and produce basement membrane

• Dot and blot hemorrhages • Occur as microaneurysms rupture in the deeper layers of the retina • (similar to microaneuryms if they are small, distinguish by fluorescein angio). • Flame-shaped hemorrhages - Splinter hemorrhages, superficial.

• Retinal edema and hard exudates. Caused by the breakdown of the blood-retina barrier, allowing leakage of serum proteins, lipids, and protein from the vessels. • Cotton-wool spots. . Nerve fiber layer infarction from occlusion of precapillary arterioles. Fluorescein angiography - No capillary perfusion • Intraretinal microvascular abnormalities – Remodeled capillary beds without proliferative

Cotton-wool spots hard exudate

Flame-shape hemorrhage

Classification of DR International Clinical DR Disease Severity Scale q q No apperant retinopathy. non-proliferative DR (NPDR) Mild Moderate Severe q q Proliferative DR (PDR) significant macular oedema - May exist by itself or along with NPDR and PDR
")
Mild NPDR • Microaneurisms only • (earliest clinically detectable lesion)

Moderate NPDR • Microaneurysms and/or dot and blot hemorrhages in at least 1 quadrant • Soft exudates (Cotton wool spots) • Venous beading or IRMA (intraretinal microvascular abnormalities) IRMA

Mild and Moderate Non- proliferative DR was previously known as Background DR

Severe NPDR Any one of the following 3 features is present • Microaneurysms and intraretinal hemorrhages in all 4 quadrants • Venous beading in 2 or more quadrants • Moderate IRMA in at least 1 quadrant Known as the 4 -2 -1 rule
 Characterized by Proliferation of new vessels from retinal veins • New")
Proliferative DR (PDR) Characterized by Proliferation of new vessels from retinal veins • New vessels on the optic disc • New vessels elsewhere on the retina

Proliferative DR NVD
 Disease Severity Scale: • DME absent: No")
2. International Clinical Diabetic Macular Edema (DME) Disease Severity Scale: • DME absent: No retinal thickening or hard exudates (HE)present in the posterior pole. • DME present: Some retinal thickening or hard exudates (HE) present in the posterior pole.

• If DME present, it can be categorized as follows: - Mild DME: Some retinal thickening or HE present in the posterior pole but distant from the center of macula. - Moderate DME: Retinal thickening or HE approaching the center of the macula but not involving its center. - Severe DME: Retinal thickening or HE involving the center of the macula.

Diabetic Macular Edema

COMPLICATIONS OF DIABETIC RETINOPATHY • Vitreous hemorrhage • Tractional retinal detachment • Rubeosis Iridis • Glaucoma • Blindness

Vitreous Hemorrhage SUBHYALOID HEMORRHAGE

Tractional retinal detachment

Rubeosis Iridis

Neovascular Glaucoma • Complication of rubeosis iridis • New vessels cause angle closure • Mechanical obstruction to aqueous outflow • Intra ocular pressure rises • Pupil gets distorted as iris gets pulled • Eye becomes painful and red • Loss of vision

Blindness • Non-clearing vitreous hemorrhage • Neovascular glaucoma • Tractional retinal detachment • Macular ischemia

PREVENTION OF COMPLICATIONS • By early institution of appropriate treatment • This requires early detection of DR in its asymptomatic treatable condition • By routine fundus examination of all Diabetics (cost effective screening) • And appropriate referral to ophthalmologist

Screening Type 1 diabetics: First screen 5 years after onset, then annually. Type 2 diabetics: First screen upon diagnosis and then annually.

ØMild and Moderate NPDR - No specific treatment for retinopathy - Good metabolic control to delay progression - Control of associated Hypertension, Anemia and Renal failure ØSevere and very severe NPDR – Close follow up by Ophthalmologist

ØClinically significant macular oedema - Laser photocoagulation to minimise risk of visual loss ØProliferative DR Retinal laser photocoagulation as per the judgment of ophthalmologist (in high risk eyes) ─ ─ It converts hypoxic retina (which produces ANGIOGENIC factors) into anoxic retina (which can’t)

Referral to Ophthalmologist • Visual Symptoms – Diminished visual acuity – Seeing floaters – Painful eye • Fundus findings - Macular oedema/hard exudates close to fovea - Proliferative DR - Vitreous hemorrhage - Moderate to severe and very severe NPDR - Retinal detachment - Cataract obscuring fundus view

Referral to Ophthalmologist • Presence of Risk Factors - Pregnancy - Nephropathy

DIRECT OPHTHALMOSCOPY • Examination of the fundus of the eye • To screen for Diabetic Retinopathy • After dilatation of both eyes with 0. 5% tropicamide

View of the retina through an ophthalmoscope

Normal fundus views of Right and left eye

Mild NPDR – Microaneurysms, Dot and Blot hemorrhages

Moderate NPDR

Moderate NPDR with CSME

Circinate retinopathy – Hard exudates in a ring around leaking aneurysms

Age related Macular degeneration: Note the drusen. Not to be confused with Hard exudates. There are no microaneurysms or dot/blot hemorrhages. DRUSEN

Severe NPDR • Cotton wool patches • Hemorrhages - 4 quadrants With CSME

Very severe NPDR -Venous beading Cotton-wool patches, venous segmentation - scars of laser spots - Absorbing hemorrhages

CSME – in Different Stages of NPDR

Proliferative DR – New vessels elsewhere on the retina along the supero-temporal vessels

PDR – New vessels on disc

PDR – New vessels on disc and new vessels elsewhere on retina

PDR – with vitreous hemorrhage Vitreous bleed

Vitreous Hemorrhage

Tractional retinal detachment Fibro-vascular proliferation

Thank you!
- Slides: 67