DIABETIC MANAGEMENT UPDATE Focus on Diabetic Foot Prevention

DIABETIC MANAGEMENT UPDATE : Focus on Diabetic Foot Prevention Supriyanto Kartodarsono Endocrinology Sub Divisionon Internal Medicine Department Faculty of Medicine UNS/ Moewardi General Hospital Surakarta

Epidemiology q 40% - 60% of all non traumatic lower limb amputation q 85% of diabetic related foot amputation are preceded by foot ulcer q 4 out of 5 ulcer in diabetics are precipitated by trauma q 4% -10% is the prevalence of foot ulcer in diabetics

Social & Economic Factors q. Diabetic foot complications are expensive : (cost of healing 7000 -10000 USD) (healing with amp. 43000 -63000 USD) (4 weeks dressing cost 110000 SD) q. Intervention of foot care is cost effective in most societies q. Scarce information regarding long term prognosis
 • Hiperosmolar hiperglikemia • Hipoglikemia •")
Komplikasi • Akut : • Ketoasidosis diabetik (KAD) • Hiperosmolar hiperglikemia • Hipoglikemia • Kronis : • Komplikasi makrovaskular (penyakit jantung koroner, stroke, penyakit vaskuler perifer) Eyes (retinopathy) Cerebrovascular disease Coronary heart disease Kidney (nephropathy) • Komplikasi mikrovaskular (retinopati, nefropati, neuropati) Peripheral nervous system (neuropathy) Peripheral Vascular disease Diabetic foot Konsensus pengelolaan dan pencegahan DM tipe 2 di Indonesia, PERKENI, 2011

Diab. Care Indonesia 2008 Diabetes Complications Soewondo, P, et al. The Diab. Care Asia 2008 Study – Outcomes on control and complications of type 2 Diabetets patients in Indonesia. Med J Indones 2010; 19: 235 -44)

UKPDS: Better glucose control means fewer complications EVERY 1% reduction RISK* A 1 C Myocardial infarctions – 14% Deaths from diabetes – 21% Microvascular complications – 37% Peripheral vascular disorders *P < 0. 0001. Adapted from Stratton IM et al. UKPDS 35. BMJ 2000; 321: 405 -12. – 43%

• Hb. A 1 c > 9. 0% or mean plasma glucose 212 mg/d. L (170 -249)* • Symptom (+) PERKENI recommended to use Insulin * Correlation between A 1 c levels and mean glucose levels, based on ADA Standards of Medical Care in Diabetes - 2017
 q. Neuro -ischemic")
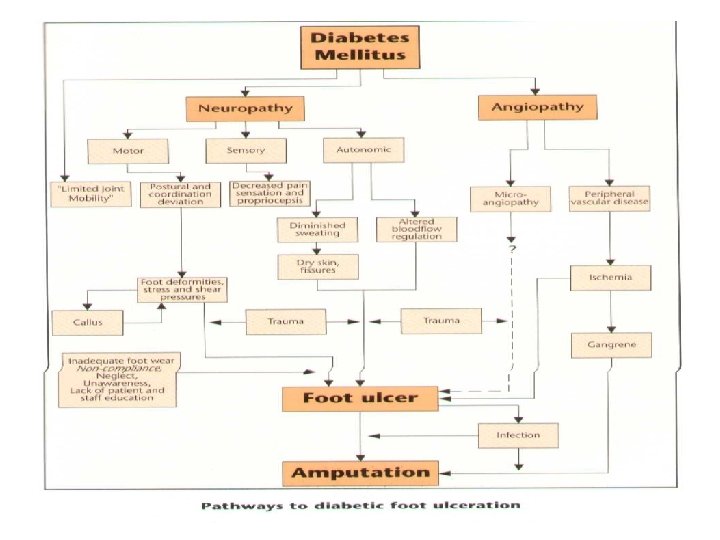
Pathophsiology of Foot Ulceration q Neuropathic q. Ischemic (vasculopathy) q. Neuro -ischemic

Chronic complications of Diabetes Macro Vascular Coronary Heart Dis. Micro and Macro Micro Vascular Diabetic Foot Neuropathy Stroke Retinopathy Peripheral Arterial Dis. Nephropathy

Macro vascular Complications
 In People with")
People with diabetes developing complications within 9 years of diagnosis (%) In People with Diabetes Macrovascular Complications Are Two Times Greater than Microvascular Complications Macrovascular complications Microvascular complications Adapted from Turner R et al Ann Intern Med 1996; 124: 136 -145.

2/3 of People with Diabetes Die of Macrovascular Diseases 67% Adapted from Alexander CM, Antonello S Pract Diabet 2002; 21: 21 -28.

Macro vascular complications • PAD • CHD • Stroke

Macro vascular complications • PAD • CHD • Stroke

Does PAD differ in diabetic from nondiabetic Subjects ? • PAD is more common in Diabetes: 30% of diabetic subjects older than 50 yrs have PAD. • Occurs at a younger age • Loss of female protection: A roughly equal male-to-female ratio

Different anatomical distribution: Predilection for the tibial and peroneal arteries between the knee and the foot.

• Diminished ability to establish collateral circulation, especially around the knee. from • Increased risk of progression intermittent claudication to critical limb ischemia and gangrene.
 frequently involves")
Medial calcinosis • Calcification involving the intimal plaque and media (medial calcinosis) frequently involves diabetic arteries at all levels.
 frequently involves")
Medial calcinosis • Calcification involving the intimal plaque and media (medial calcinosis) frequently involves diabetic arteries at all levels.

Presentation of PAD • One-half are asymptomatic or have atypical symptoms, • One-third have claudication, • The remainder have more severe of the forms disease

Intermittent Claudication • Intermittent claudication, defined as pain, cramping, or aching in the calves, thighs, or buttocks that appears reproducibly with walking exercise and is relieved by rest. • The history of PAD is characteristic and consistently reproducible, and may alone be diagnostic for many individuals.

Signs of PAD Unlike other forms of atherosclerotic disease, PAD is easily diagnosed in the outpatient clinic noninvasively.


• The dorsalis pedis pulse is reported to be absent in 8. 1% of healthy individuals, and the posterior tibial pulse is absent in 2. 0%. • Nevertheless, the absence of both pedal pulses, when assessed by a person experienced in this technique, strongly suggests the presence of vascular disease

• Temperature differences can be reliably assessed only when limbs have been exposed to a constant room temperature for 10 -20 minutes.


• Absence of hair growth, thin and shiny skin, dystrophic toenails, and cool, dry, fissured skin are signs of vascular insufficiency and should be noted.

Chronic complications of Diabetes Macro Vascular Coronary Heart Dis. Micro and Macro Micro Vascular Diabetic Foot Neuropathy Stroke Retinopathy Peripheral Arterial Dis. Nephropathy

Micro Vascular complications

Micro vascular complications • Neuropathy • Retinopathy • Nephropathy

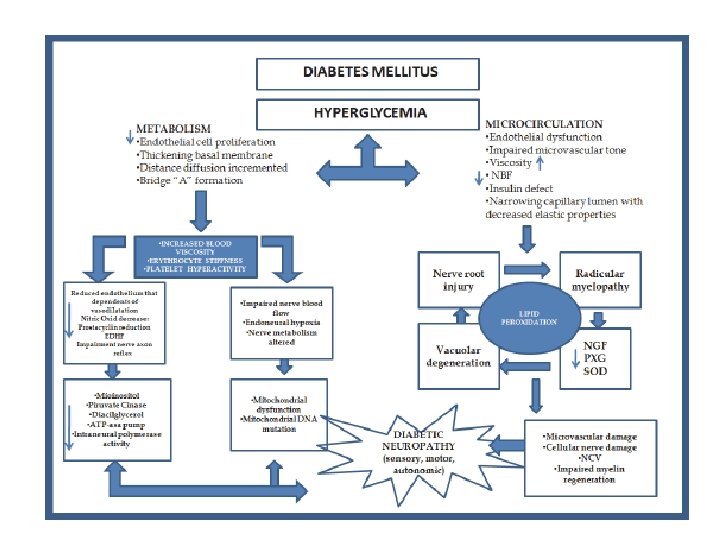
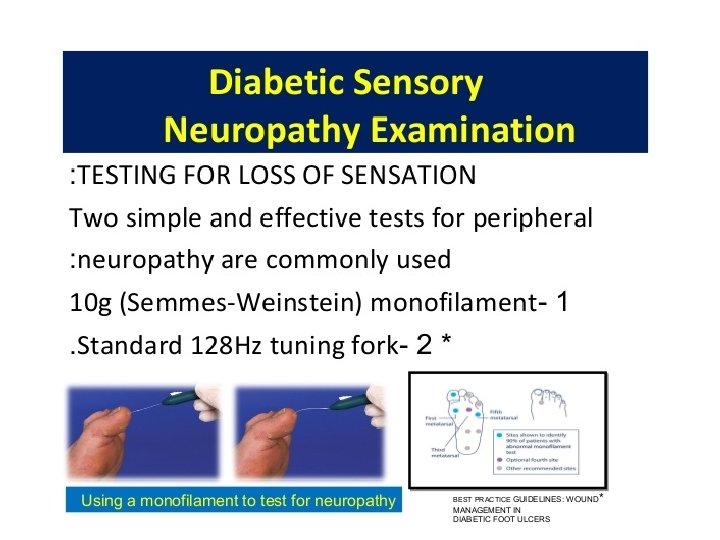
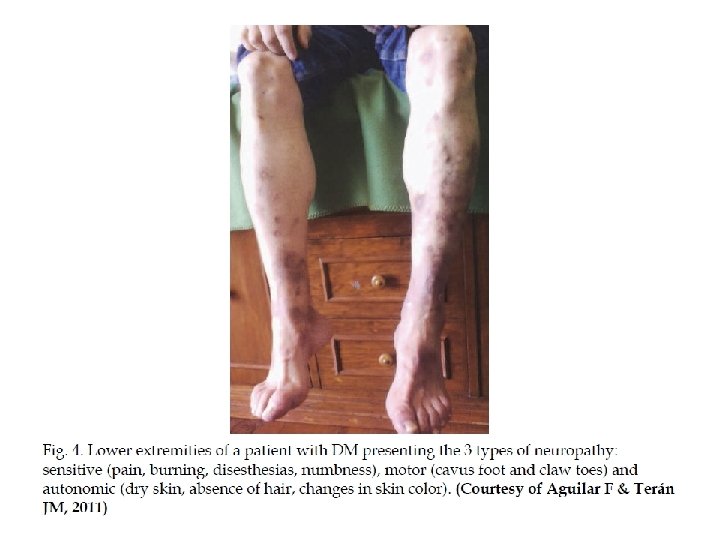
Diabetic Neuropathy q. Sensorimotor & peripheral sympathatic neuropathy are major risk factors for ulcer q. History & careful foot examination are mandatory to diagnose neuropathy q. Up to 50%of type 2 diabetic patient have significant neuropathy & at risk of foot ulcer

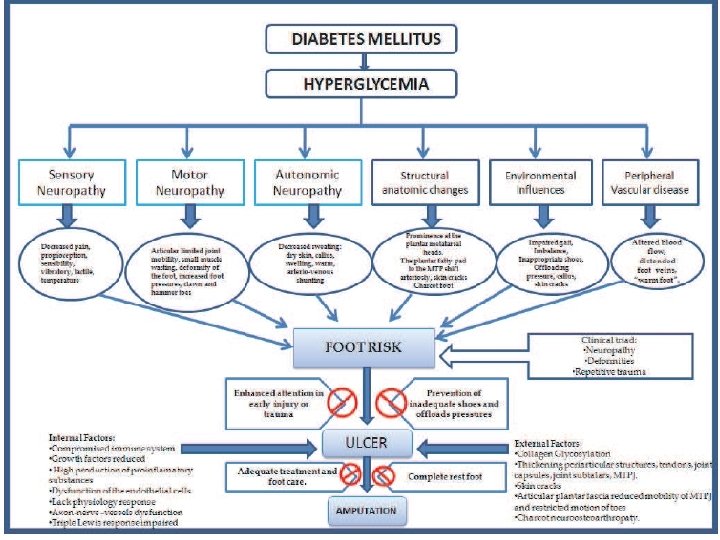
Pathophysiology of foot ulcers from diabetic neuropathy Sensory dysfunction Decreased Sensory Perception of : • Pain • Vibration • Temperature • Touch Injury : • Mechanical • Thermal • Chemical Motor dysfunction Small Muscle atrophy Imbalance of flexor And extensor muscles Clawed toes Prominent metatarsal heads Altered gait Callus Foot Ulcer Autonomic dysfunction Decreased sweating Arterio-venous shunt Dry, scaly skin Decreased capilary pressure Fissures Edema Infection Poor wound healing

Neuro-osteoarthropathy q. Non- infective pathology q. Should be suspected in any swollen hot erythematous foot q. Differentiation from infection is important to prevent misdiagnosis & possible amputation q. Treatment should aim at preventing severe deformity

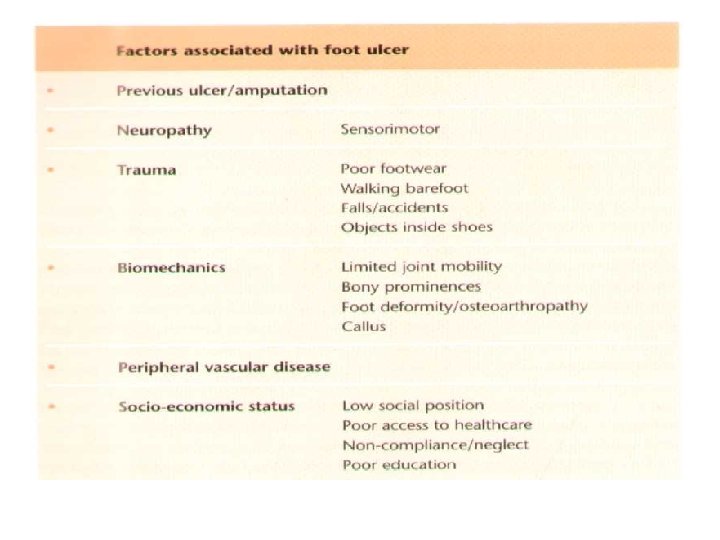
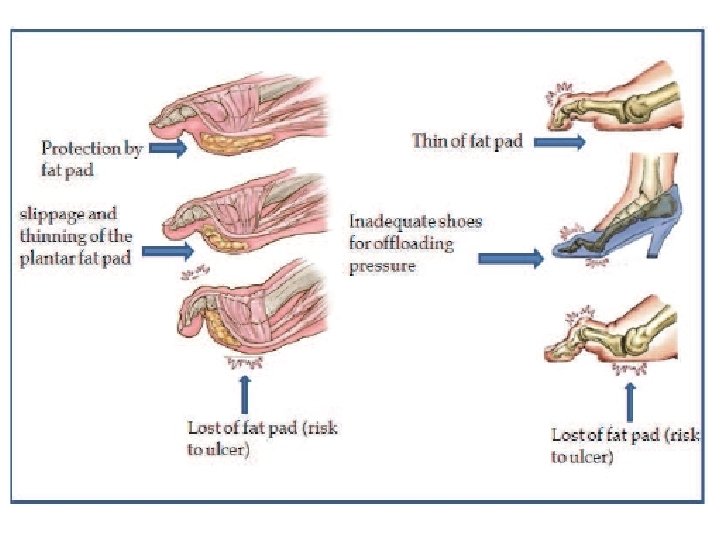
Biomechanics of foot wear q Biomechanical abnormalities are consequence of neuropathy, they lead to abnormal foot pressure q Foot deformity & neuropathy increase the risk of ulcer q Pressure relief is essential for ulcer healing and/or prevention q Frequent inspection of shoes & insoles is mandatory q Appropriate foot wear significantly reduce ulcer recurrence

Diabetic Foot Infection q Infection in diabetic foot is limb threatening q Signs of infection may be absent in diabetic pt. with foot ulcer q Superficial infection is usually caused by gram +ve cocci, deep infection is poly microbial q Surgical debridment is essential in acute deep infection q Osteomylitis( diagnoses & treatment)

Diabetic Foot Ulcer Treatment q. Multidisciplenary approach q. Staging dictate the treatment option q. Continuity of care & life long observation

Amputation in Diabetic Patient q. Increased minormajor amputation increased the no. of deformed feet q. Minor amputation is needed : *Gangrene *As part of debriment *for correction of foot deformities q. Minor amputation doesn’t significantly compromise walking ability

Major Amputation q Risk of loss walking ability q Mortality q Risk of contra-lateral amputation q Strict indication q Careful choice of the level

How To Prevent Foot Problems 5 corner stones q. Regular inspection & examination of foot & foot wear q. Identification of high risk patient q. Education of patient, family & health care providers q. Appropriate foot wear q. Treatment of non ulcerative pathology

q. Thight glucose control is the most important

CARE • Control: control blood glucose levels • Annual: attend your annual foot screening examination. • Report: report any changes in your feet to your immediately healthcare professional. • Engage: engage in a simple daily foot care routine by washing and drying between your toes, moisturizing and checking for abnormalities.

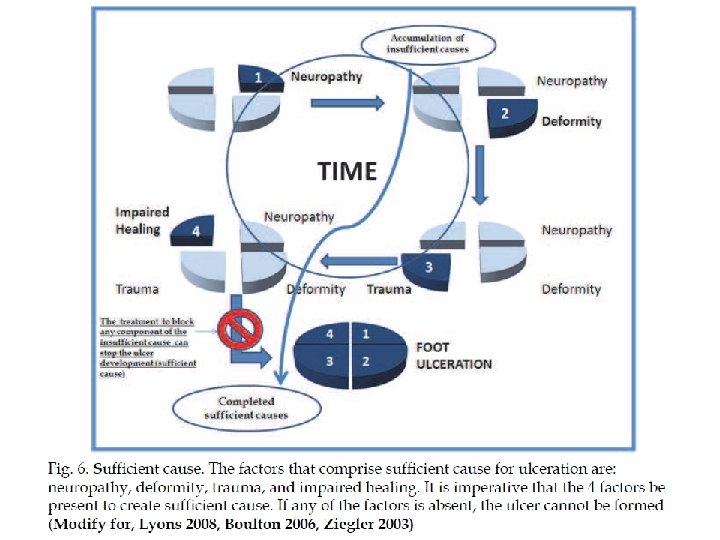
• In order to prevent amputation, we should diagnose and treat any mild foot pathology before its progression into advanced foot pathology.

Low Risk Foot High Risk Foot Advanced Foot Pathology Gangrene

What can be done to prevent the development of advanced foot pathology? • Regular inspection and examination of the foot. • Identification of the foot at risk. • Education of patient, family and healthcare providers. • Appropriate footwear. • Treatment of non ulcerative pathology Tight glucose control is the most important
- Slides: 56