DIABETIC CONSIDERATIONS IN PROSTHODONTICS UNNI PYMPALLIL II nd

DIABETIC CONSIDERATIONS IN PROSTHODONTICS UNNI PYMPALLIL II nd MDS DEPT. OF PROSTHODONTICS

CONTENTS: ØINTRODUCTION Ø TYPES ØETIOLOGY ØHOW INSULIN DECREASE PLASMA GLUCOSE LEVEL ØPATHOGENESIS ØMECHANISM OF HYPERGLYCEMIA IN DIABETES ØRISK FACTORS ØCLINICAL MANIFESTATION ØCOMPLICATIONS OF DIABETES MELLITUS

ØLABORATORY TESTS ØORAL ANTI DIABETIC DRUGS ØINSULIN PREPARATION ØORAL MANIFESTATION ØPROSTHODONTIC CONSIDERATION DIABETES ØSALIVA ØCANDIDIASIS ØDENTURE STOMATITIS ØANGULAR CHELITIS ØDENTAL CARIES ØPREPROSTHETIC SURGEY AND IMPLANT ØRESIDUAL RIDGE RESORPTION ØANTIBIOTIC CONSIDERATION ØANAESTHETIC CONSIDERATION

ØPROSTHODONTIC MANAGEMENT OF DIABETIC DENTAL PATIENT ØEMERGENCY MANAGEMENT ØCONCLUSION ØREFERENCES

INTRODUCTION

TYPE 1 IDDM • Beta cell destruction, usually leading to absolute insulin deficiency • Immune-mediated: presence of islet cell or insulin antibodies that identify the autoimmune process, leading to beta cell destruction • Insulin resistance with relative insulin TYPE 2 NIDDM deficiency/ insulin secretory defect with insulin resistance • Circulating endogenous insulin blood levels are adequate to prevent ketoacidosis in the resting state, but inadequate to meet increased needs caused by insensitivity of the tissues. • High incidence of obesity. Joslin’s diabetes melliyus thirteenth edition, page 193 -199

TYPE III OTHER TYPES • diseases of exocrine pancreas, drug or chemical-induced diabetes, infections, uncommon forms of immune-mediated diabetes Data from American Diabetes Association: Standards of Care— 2011, Diabetes Care 34(Suppl 1): S 11 -S 61, 2011.

Etiology 1. Etiology of Type 1 Diabetes 8 Joslin’s diabetes melliyus thirteenth edition, page 193 -199

2. Etiology of Type 2 Diabetes 9 Joslin’s diabetes melliyus thirteenth edition, page 193 -199

How Insuline Decrease Plasma Glucose Level? 10 Joslin’s diabetes melliyus thirteenth edition, page 193 -199

PATHOGENESIS: Reduced insulin secretion Decreased glucose use by the body Increased glucose production Joslin’s diabetes mellitus thirteenth edition, page 216 -240

12 Joslin’s diabetes melliyus thirteenth edition, page 216 -240

13 Joslin’s diabetes melliyus thirteenth edition, page 216 -240

14 Joslin’s diabetes melliyus thirteenth edition, page 193 -199

Risk Factors �Type 1 DM Genetic predisposition � �In an individual with a genetic predisposition, an event such as virus or toxin triggers autoimmune destruction of b-cells probably over a period of several years. Joslin’s diabetes melliyus thirteenth edition, page 282 --300 15

�Type 2 DM � Family History � Obesity � Habitual physical inactivity � Hypertension � Hyperlipidemia 16 Joslin’s diabetes melliyus thirteenth edition, page 300 -372

Clinical Manifestations of Diabetes Polydypsia Polyuria Polyphagia with weight loss Loss of strength Nocturnal anueresis Blurred vision TYPE 1 TYPE 2 ++ ++ ++ ++ Joslin’s diabetes melliyus thirteenth edition, page 300 -372

OTHER SYMPTOMS: TYPE 1 TYPE 2 v Decreased vision v Repeated skin v Paresthesias, infections v Loss of sensation v. Headache v Impotence v Drowsiness v Postural hypotension Joslin’s diabetes melliyus thirteenth edition, page 300 -372
 : ACUTE hypoglycemia diabetic ketoacidosis Joslin’s diabetes melliyus thirteenth")
Complications of Diabetes Mellitus (DM) : ACUTE hypoglycemia diabetic ketoacidosis Joslin’s diabetes melliyus thirteenth edition, page 605 -670 hyperosmolar nonketotic coma
 : CHRONIC Vascular system: atherosclerosis (coronary heart disease), microangiopathy.")
Complications of Diabetes Mellitus (DM) : CHRONIC Vascular system: atherosclerosis (coronary heart disease), microangiopathy. 2/3 rd have high BP ; risk for stroke and heart disease death is 2 to 4 times higher among people with DM Eyes: retinopathy, cataracts; DM is leading cause of new cases of blindness among adults Kidney: diabetic nephropathy; DM is leading cause of renal failure Joslin’s diabetes melliyus thirteenth edition, page 605 -670

Laboratory Tests 1. Glucosuria o o o Normally glucose does not appear in urine until the plasma glucose rises above 160 -180 mg/dl. In certain individuals due to low renal threshold glucose may be present despite normal blood glucose levels. Conversely renal threshold increases with age so many diabetics may not have Glycosuria despite high blood sugar levels. 2. Ketonuria – To detect keton bodies in urine by a paper strip 21

3. Fasting blood glucose is measured after an overnight fast of 10 hrs. Fasting blood glucose estimation is better than random blood glucose. Fb. G < 100 mg/d. L is considered normal; Fb. G = 100– 125 mg/d. L is defined as Intermediate Fb. G > 126 mg/d. L warrants the diagnosis of DM. 22

4. Random Blood glucose – RBG measurement is required only during emergency. o. The current criteria for the diagnosis of DM emphasize that the FPG is the most reliable and convenient test for identifying DM in asymptomatic individuals. o A random plasma glucose concentration 200 mg/d. L accompanied by classic symptoms of DM (polyuria, polydipsia, weight loss) is sufficient for the diagnosis of DM. 23

5. Glucose tolerance test � 75 gm of glucose are given to the patient with 300 ml of water after an overnight fast �Blood samples are drawn 1, 2, and 3 hours after taking the glucose �This is a more accurate test for glucose utilization if the fasting glucose is borderline 24
 �Hb. A 1 C is formed by")
6. Glycosylated hemoglobin (Hb. A 1 C) �Hb. A 1 C is formed by condensation of glucose with free amino groups of the globin component of hemoglobin �Normally it comprises 4 -6% of the total hemoglobin. �Increase in the glucose blood concentration increases the glycated hemoglobin fraction. �Hb. A 1 C reflects the glycemic state during the preceding 8 -12 weeks. 25
 �Since serum albumin")
7. Serum Fructosamine �Formed by glycosylation of serum protein (mainly albumin) �Since serum albumin has shorter half life than hemoglobin, serum fructosamine reflects the glycemic state in the preceding 2 weeks �Normal is 1. 5 - 2. 4 mmole/L when serum albumin is 5 gm/d. L. 26

Lipid profile : o Serum Total cholesterol is elevated o Serum triglycerides are high o Serum HDLc is low

Self Monitoring Test �Self-monitoring of blood glucose �Extremely useful for outpatient monitoring specially for patients who need tight control for their glycemic state. �A portable battery operated device that measures the color intensity produced from adding a drop of blood to a glucose oxidase paper strip. �e. g. One Touch, Accu-Chek 28

29
 1. 2. First generation")
Oral anti-diabetic drugs 1. Sulphonylureas (Daonil 5 mg once daily) 1. 2. First generation – tolbutamide , chlorpropamide Second generation – glibenclemide , glipicide , gliclazide , glimipride Biguanides (Glucophage XR 500 mg b. i. d) – Metformin, fenformin 3. Meglitinide analogue – Repaglinide 4. D-phenyalanine derivative – nateglinide 5. Thiazolidinediones (Avandia 4 mg once daily)- Rosiglitazone, pioglitazone 6. Alpha-glucosidase inhibitors - acarbose
")
Insulin preparations: CLASSIFI GENERIC ONSET CATION NAME PEAK DURATIO EFFECT(i N (in n hours) Rapid acting <15 mins 1 -2 3 -4 Short acting Humulin R Novalin R Reli. On 0. 5 -1 hr 2 -3 3 -6 Intermediat NPH e acting 2 -4 hrs 4 -10 10 -16 Long acting Insulin Glargine 2 -4 hrs Peakless 20 -24 Lispro Aspart

Methods of insulin administration SITE OF ADMINISTRATION 1. Abdomen, buttock, anterior thigh and dorsal arm- subcutaneously

Inhaled Insulin-The FDA approved the first inhaled version of insulin called Exubera from Pfizer Inc.

Drug Interactions �B adrenergic blockers mask tachycardia, the important warning symptom of hypoglycemia. They also prolong hypoglycemia by inhibiting compensatory mechanisms acting through B 2 receptors. �Salicylates precipitate hypoglycemia by enhancing insulin secretion and B cell sensitivity to glucose.

�Current insulin administration requires subcutaneous injection or infusion �Constant monitoring and multiple daily doses of insulin are required to maintain a healthy blood glucose level �Oral delivery would be easier and could provide an extended pharmacological effect for basal insulin levels
 Ø Salivary dysfunction")
Oral Manifestations of Diabetes Mellitus Ø Periodontal diseases (periodontitis and gingivitis) Ø Salivary dysfunction - reduction in salivary flow and changes in saliva composition, and taste dysfunction. Ø Oral fungal and bacterial infections. Ø There also reports of oral mucosa lesions in the form of stomatitis and angular chelitis. Ø In addition, delayed mucosal wound healing, dental caries and tooth loss. Ø Xerostomia, periapical abscesses, burning mouth are also manifested. Oral Manifestations and Complications of Diabetes Mellitus : A review Awatif Y. Al-Maskari, 1 Masoud Y. Al-Maskari, 2, * and Salem Al-Sudairy 1

PROSTHETIC CONSIDERATIONS ON DIABETES SALIVA CANDIDAL INFECTIONS DENTURE STOMATITIS ANGULAR CHELITIS ALTERED TASTE SENSATION BURNING MOUTH SYNDROME DENTAL CARIES PRE PROSTHETIC SURGERY AND IMPLANT PLACEMENT 9. RESIDUAL RIDGE RESORPTION 10. ANTIBIOTIC CONSIDERATION 11. ANAESTHETIC CONSIDERATION 1. 2. 3. 4. 5. 6. 7. 8.
 Major groups of")
SALIVA There are Major and Minor groups of Salivary Glands: a) Major groups of salivary glands which are consists three major glands, the parotid, submandular and sublingual glands. The parotid produces mucous secretions. The parotid and sub-mandular glands each drain into the mouth in a single long duct. Where as the sublingual glands drain via many small ducts. TEXTBOOK OF HUMAN HISTOLOGY INDERBIR SINGH, FIFTH EDITION, PAGE 54
 Minor groups of salivary glands may be found in the lips, cheeks,")
b) Minor groups of salivary glands may be found in the lips, cheeks, tongue, floor of the mouth, palate, larynx, trachea and tonsils and lacrymal gland. And all are liable to undergo the same pathological change as the major groups. The total salivary secretion is between 1, 000 ml – 1, 500 ml daily and is almost all the result of stimulation. TEXTBOOK OF HUMAN HISTOLOGY INDERBIR SINGH, FIFTH EDITION, PAGE 54

A. SALIVA Lysozyme Amylases, Cystatins, Histatins, Mucins, Peroxidases Cystatins, Mucins Anti. Bacterial Carbonic anhydrases, Histatins Buffering Anti. Viral Digestion Salivary Functions Anti. Fungal Mineralization Histatins Tissue Coating Amylases, Cystatins, Mucins, Proline-rich proteins, Statherins Lubrication &Viscoelasticity Amylases, Mucins, Lipase Cystatins, Histatins, Prolinerich proteins, Statherins Mucins, Statherins

Salivary Gland Changes : Ø Sialoadenosis or Ø Noninflammatory, non-neoplastic enlargement of the parotid salivary glands, Ø decreased salivary flow rates, Ø Changes in salivary composition The enlargements are caused by gradual accumulation of fat in the glands, hypertrophy of the acini or secreting units, and, eventually, impaired glandular secretion. These structural changes may be the result of alteration in autonomic neuroregulation of the glands and atrophy of the myoepithelial cells that facilitate salivary secretion. Non-Periodontal Oral Manifestations of Diabetes: A Framework for Medical Care Providers Beatrice K. Gandara, DDS, MSD and Thomas H. Morton Jr. , DDS, MSD

Xerostomia : The sensation of dry mouth, is reported to occur in 40– 80% of diabetic patients and is related to decreased salivary flow rates. The mechanism by which salivary flow is affected in diabetic patients is thought to be the result of autonomic nerve dysfunction or microvascular changes that diminish the ability of the salivary glands to respond to neural or hormonal stimulation. Other causes may include dehydration or side effects of concomitant drug therapy commonly used in diabetic patients. Newrick PG, Bowman C, Green D, O'Brien IA, Porter SR, Scully C, Corrall R: Parotid salivary secretion in diabetic autonomic neuropathy. J Diabetes Complications 5: 35– 37, 1991

PROSTHETIC CONSIDERATIONS ON XEROSTOMIA �Difficult to wear denture, may cause constant irritation in the mucosa �Patient should be allowed to wet his mouth constantly during appointment �Salivary substitutes can be given if condition is severe

Type 1 diabetes mellitus, xerostomia, and salivary flow rates Paul A. Moore, DMD, Ph. D, MPH, a James Guggenheimer, DDS, b Kenneth R. Etzel, Ph. D, c Robert J. Weyant, DMD, Dr. PH, �study of 406 subjects with type 1 diabetes and 268 control subjects without diabetes that assessed the associations between oral health and diabetes. This report describes the prevalence of dry-mouth symptoms (xerostomia), the prevalence of hyposalivation

�Conclusion: Subjects with type 1 diabetes who had developed neuropathy more often reported symptoms of dry mouth as well as symptoms of decreased salivary flow rates. Because of the importance of saliva in the maintenance and the preservation of oral health, management of oral diseases in diabetic patients should include a comprehensive evaluation of salivary function

Effects of glycemic control on saliva flow rates and protein composition in non-insulin-dependent diabetes mellitus Michael W. J. Dodds, BDS, Ph. D, a and Anne P. Dodds, BDS, MPH, b San Antonio, Texas �Objective. The objective of this study was to determine whether improvements in the level of diabetic control in a group of subjects with poorly controlled noninsulin-dependent diabetes mellitus influence salivary output and composition �Conclusions. Poorly controlled non-insulin-dependent diabetes mellitus has no influence on saliva output, although amylase activity may be elevated, and there may be taste alterations.

Angular Cheilitis �Cracks, fissures, crusts, pain in commissure area �Loss of vertical dimension �Deep folds of skin at angles of mouth �Continual wetting by saliva �Nutritional deficiencies 3 rd edition Oral and maaxillofacial pathology, Neville page: 422 -436

Commissural Cheilitis. - Refers to inflammation of the angles of the mouth. - Attributed to excessive interocclusal distance. - Usually develops when occlusal plane of the lower teeth is too high. This prevents the regular action of the cheek from eliminating the saliva from the lower buccal vestibule, so saliva will exit through the corners of the mouth causing spread of infection to the angles of the mouth. - To treat the problem, it is advisable to construct new dentures. 3 rd edition Oral and maaxillofacial pathology, Neville page: 422 -436
")
Fungal Infections Candida albicans �Mainly on the tongue �Candidal counts overlap between patients (infection) and carriers 3 rd edition Oral and maaxillofacial pathology, Neville page: 422 -436

RESIDUAL RIDGE RESORPTION �Residual ridge : “the portion of the residual bone and its soft tissue covering that remains after the removal of teeth ” �Residual ridge resorption : “a term used for the diminishing quantity and quality of the residual ridge after teeth are removed ” ( GPT 8 ) Atwood DA: Postextraction changes in the adult mandible as illustrated by microradiographs of midsadittal section and serial cephalometric roentgenograms. JPD; 1963; 13; 810

Anatomic consequences of edentulism � Bone needs stimulation to maintain its form and density. � When a tooth is lost, the lack of stimulation to the residual bone causes a decrease in trabeculae and bone density in the area, with loss in external width, then height of the bone volume. Atwood DA: Postextraction changes in the adult mandible as illustrated by microradiographs of midsadittal section and serial cephalometric roentgenograms. JPD; 1963; 13; 810

Anatomic consequences of edentulism � There is a 25 % decrease in width of bone during the first year after tooth loss and an overall 4 mm decrease in height during this first year following extractions for an immediate denture. � A tooth is necessary to the development of the alveolar bone, and stimulation of this bone is required to maintain its density and volume.

Anatomic consequences of edentulism � The bone loss often accelerates when the patient wears a poorly fitting soft tissue borne prosthesis. � Yet the patients do not understand that bone is being lost over time, and at a greater rate under poorly fitting dentures. ( moreover, no regular visits ) � Hence the traditional method of tooth replacement often affects bone loss in a manner not sufficiently considered by the dentist and the patient. Atwood DA: Postextraction changes in the adult mandible as illustrated by microradiographs of midsadittal section and serial cephalometric roentgenograms. JPD; 1963; 13; 810

Anatomic consequences of edentulism � The loss of teeth causes remodeling and resorption of the surrounding alveolar bone and eventually leads to atrophic edentulous ridges. � The rate and amount of bone loss may be influenced by such things as sex, hormones, metabolism, parafunction, and ill fitting dentures. Atwood DA: Postextraction changes in the adult mandible as illustrated by microradiographs of midsadittal section and serial cephalometric roentgenograms. JPD; 1963; 13; 810

Anatomic consequences of edentulism � The loss of bone first causes decreased bone width. � The remaining narrow residual ridge often causes discomfort when the thin overlying tissues are loaded under a soft tissue borne removable prosthesis. � Loss of bone in the maxilla or mandible is not limited to alveolar bone ; portions of the basal bone may be resorbed also, especially in the posterior aspect of the mandible where severe resorption may result in more than 65 % bone loss. Atwood DA: Postextraction changes in the adult mandible as illustrated by microradiographs of midsadittal section and serial cephalometric roentgenograms. JPD; 1963; 13; 810

Anatomic consequences of edentulism � The load from mastication is transferred to the bone surface only and not to the whole bone. � Masticatory forces generated by short facial types can be 3 or 4 times that of long facial types. � The short facial types patients are at increased risk to develop severe atrophy. Atwood DA: Postextraction changes in the adult mandible as illustrated by microradiographs of midsadittal section and serial cephalometric roentgenograms. JPD; 1963; 13; 810

Anatomic consequences of edentulism � Many of these similar conditions exist in the partially edentulous patient wearing a removable soft tissue borne prosthesis. � In addition, the natural abutment teeth, on which direct retainers are designed, must submit to additional lateral forces. � Because these teeth are often compromised by deficient periodontal support, many partial dentures are designed to minimize the forces applied to them. Atwood DA: Postextraction changes in the adult mandible as illustrated by microradiographs of midsadittal section and serial cephalometric roentgenograms. JPD; 1963; 13; 810

Anatomic consequences of edentulism � The net result is an increase in mobility of the removable prosthesis and greater soft tissue support. � These conditions protect the remaining teeth, but accelerate the bone loss in the edentulous regions. Atwood DA: Postextraction changes in the adult mandible as illustrated by microradiographs of midsadittal section and serial cephalometric roentgenograms. JPD; 1963; 13; 810

Alveolar Bone Loss Progression in Diabetes: � It suggested that poorer glycemic control leads to both an increased risk for alveolar bone loss and more severe progression over those without type 2 DM. � 1. Polymorphonuclear Leukocyte Function. � 2. Collagen Metabolism and Advanced Glycation End products. Joslin’s diabetes melliyus thirteenth edition, page 912 -920

Association of type 2 diabetes mellitus with the reduction of mandibular residual ridge among edentulous patients using panoramic radiographs Osama Al-Jabrah, Open Journal of Stomatology, 2011, 1, 61 -68 Objective: To evaluate the association between type 2 diabetes mellitus and the reduction of mandibular residual ridge in completely edentulous patients wearing complete dentures and to investigate the effect of gender, age and years of edentulousness/ den-ture wearing on ridge resorption on both groups. �

� Conclusion: Completely edentulous, den-ture- wearing diabetics, women in particular, are at more risk to have ridge resorption than “nondiabetic” subjects. Reduced mandibular height is di-rectly related to years of edentulousness and den-ture wearing with greater amount of resorption among diabetics.

TREATMENT Non surgical � Mechanical stimulation • Stimulation is to be administered with an automatic tooth brush applied to the gingiva and the edentulous area with the bristle head of the toothbrush. • The stimulation should be administered for 15 seconds in each section. Stimulation is to be administered daily except Sundays, for a period of 4 weeks. • The power device oscillates the brush at an average of 2000 strokes per minute. Nylon bristles with thickness ranging from 0. 007 to 0. 012 inch in diameter comprise the brushes.

TREATMENT Nutrient Effect on metabolism Calcium Increases peak bone mass, decreases rate of bone loss in post menopausal women Vitamin D Increases intestinal absorption of calcium, decreases bone resorption. Phosphorus High intake may increase calcium urinary loss Sodium High intake increases urinary calcium losses if the calcium intake is low Fluoride Stimulate osteoblasts, increases trabecular bone mass, new bone may be poorly mineralized. Caffeine High intake increases calcium urinary losses Alcohol High intake accelerates menopause toxic effects on osteoblasts, increased calcium urinary losses

Surgical treatment � Preprosthetic surgery includes the following: � Ridge preservation procedure as a preventive measure � Corrective or recontouring procedures of the defects and abnormalities � Ridge extension procedures �Relative methods e. g. , sulcus extension (vestibuloplasty) �Absolute methods e. g. , ridge augmentation method

Dietary guidelines for patients at risk of losing bone � Maintain a high daily calcium intake �Obtain four servings of low fat dairy foods or obtain equivalent amounts of calcium from green, canned fish or tofu daily �Take calcium supplements if dietary intake is low �Choose calcium citrate maleate if patient has achlorhydria �If lactose intolerant, treat milk with lactase tablets or drops

Dietary guidelines for patients at risk of losing bone � Prevent negative calcium balance �Limit daily alcohol and caffeine intake �Consume about 6 ounces of protein from meat, poultry and fish �Use small amounts of processed foods high in sodium

Dietary guidelines for patients at risk of losing bone � Obtain 4000 I. U of Vitamin D daily �Spend 15 minutes in the sun 3 times a week �Choose a multivitamin or calcium supplement that contains 4000 I. U of Vitamin D. � Discuss calcium or drug interactions that interface with calcium bioavailability with the physician

BACTERIAL AND FUNGAL INFECTIONS : Lack of adequate saliva leads to : - risk of oral yeast infections + caries rate - difficulty with maintaining oral hygiene, - in quality of life because of discomfort from eating, swallowing, and talking. The combination of a low flow rate and immune dysfunction greatly increases the risk of oral candidiasis. This may also be the result of increased salivary glucose levels, which promote over-growth of Candida as well as decreased antifungal immunoglobulins in saliva caused by diabetes Sashikumar R, Kannan R: Salivary glucose levels and oral candidal carriage in type II diabetics. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 109: 706– 711, 2010

PROSTHETIC MANAGEMENT OF RESIDUAL RIDGE RESORBED CASES

-While fabricating the removable dentures the main area of focus should be on reduction of the forces on residual ridge. -Mucostatic or open mouth impression techniques, selective pressure impression technique, should be employed to reduce mechanical forces while impression making. -Semi anatomic or non anatomic teeth with narrow buccolingual width should be selected. Osteoporosis: its prosthodontic considerations –a review, JCDR, 2015

�While fabricating the removable dentures the main area of focus should be on reduction of the forces on residual ridge. � -Mucostatic or open mouth impression techniques, selective pressure impression technique, should be employed to reduce mechanical forces while impression making.

A Technique for Impressing the Severely Resorbed Mandibular Edentulous Ridge Nair K. Chandrasekharan, MDS, Ashish T. Kunnekel, MDS, Mahesh Verma, BDS, MBA & Rajiv K. Gupta, MDS Journal of Prosthodontics 21 (2012) 215– 218 �The mandibular primary impression is made with irreversible hydrocolloid in a stock tray modified with putty-consistency elastomeric impression � The primary cast is poured in Type III dental stone and a tray devoid of spacer or relief wax is fabricated over the primary cast using autopolymerizing resin

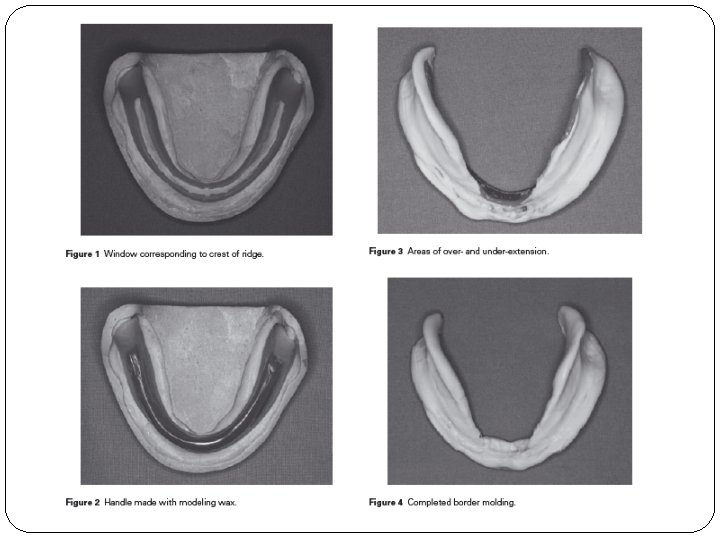
�After evaluation in the mouth, the custom tray is adjusted to be 2 mm short of the functional depth of the labial and lingual sulci. � The crest of the ridge is marked using an indelible pencil and is transferred to the tray via placement of the tray on the ridge. � A window is cut in the tray using a straight bur outlining the marked area, corresponding to the crest of the ridge Journal of Prosthodontics 21 (2012) 215– 218

�The tray is then seated onto the cast, and softened modeling wax is placed into the window, thereby replacing the eliminated acrylic resin, and shaped to form a handle � Putty consistency elastomer (Affinis) and tray adhesive and intaglio surface of the custom tray are placed on the tray. The tray is seated onto the ridge, and the labial and lingual borders are molded �Areas of overextension indicated by exposure of the tray borders are corrected by removing the putty in the corresponding area and trimming the tray Journal of Prosthodontics 21 (2012) 215– 218

�A second application of putty is made over the first, and the borders are molded again � The borders of the impression are carefully re-examined for any over- or under-extensions and are corrected accordingly. �The borders of the impression are trimmed by 0. 5 mm using a sintered diamond bur mounted in a micromotor handpiece. � The wax handle is removed and the putty material over the window is cut out using a sharp Bard-Parker knife. � Light-body elastomeric impression material (Affinis) is loaded into the tray, which is then seated on the ridge. Additional light-body material is then expressed into the window. Lingual and facial borders are molded, ensuring the tray remains steady until the impression material sets Journal of Prosthodontics 21 (2012) 215– 218

Modified fluid wax impression for a severely resorbed edentulous mandibular ridge Kian M. Tan, Michael T. Singer, Radi Masri, Carl F. Driscoll, J Prosthet Dent 2009; 101: 279 -282 �According to Applegate, the use of fluid wax in impression making was described previously by Everett. It has the following advantages: (1) it can be easily controlled to gain maximum coverage; (2) it can be corrected readily; (3) it can be used to accurately determine the extent of the muccobuccal reflections; and (4) it can be used to direct pressure to the loadbearing areas, specifically, the buccal shelves and the slopes of residual ridges in the mandible.

J Prosthet Dent 2009; 101: 279 -282

J Prosthet Dent 2009; 101: 279 -282

J Prosthet Dent 2009; 101: 279 -282

Impression Techniques for Resorbed Ridges � The different techniques available are: 1. The Functional Impression Technique 2. The Neutral Zone Technique Jain M. Impression techniques for the resorbed mandibular arch: A guide to increased stability. J Sci Soc 2015; 42: 88 -91.

Functional Impression Technique � Functional impression can be used very effectively to create stability in cases exhibiting extreme resorption � Though retention is usually poor in such cases yet the clinician can set out to achieve stability in these patients � The prosthesis should remain stable within the oral cavity and not move at the slightest movement of the tongue Jain M. Impression techniques for the resorbed mandibular arch: A guide to increased stability. J Sci Soc 2015; 42: 88 -91.

� A functional impression can be made after doing the border moulding using a stable custom tray � Temporary soft liners and tissue conditioners can be used as functional impression materials as they exhibit the property of delayed setting and a continuous over a longer period of time thereby recording all possible movements of the mandibular musculature. Jain M. Impression techniques for the resorbed mandibular arch: A guide to increased stability. J Sci Soc 2015; 42: 88 -91.

� The extensions of the custom tray should be verified accurately and border moulding done � After completion of the procedure, instead of using the regular impression material for making definitive impressions, a functional impression material can be used � The material is mixed and placed on the impression surface of the custom tray Jain M. Impression techniques for the resorbed mandibular arch: A guide to increased stability. J Sci Soc 2015; 42: 88 -91.

� The material is initially moulded using the regular movements technique of secondary impression making � Once the material attains an initial set, the patient is instructed to read a news paper aloud, drink water 34 times and swallow saliva at regular intervals and other daily chores � The functional impression material stays within the oral cavity for a period of 45 -60 min. All oral activities of the patient are encouraged Jain M. Impression techniques for the resorbed mandibular arch: A guide to increased stability. J Sci

� Once the material has achieved a final set, the tray is removed and the impression is poured � The cast obtained is used as a master cast for fabrication of prosthesis Jain M. Impression techniques for the resorbed mandibular arch: A guide to increased stability. J Sci Soc 2015; 42: 88 -91.

Neutral Zone Impression Technique � Though all of us realize the importance of neutral zone yet no one tries to use it for increasing the stability in complete denture prosthesis � If done correctly, the neutral zone can increase the stability and retention to a great extent � Recording the neutral zone is itself quite simple Jain M. Impression techniques for the resorbed mandibular arch: A guide to increased stability. J Sci Soc 2015; 42: 88 -91.

� After taking jaw relations, the maxillary and mandibular cast is mounted using a face bow transfer � Thereafter, the mandibular wax rim is cut off and wire loops in the shape of letter “v” are made on the lower record base up to the height of the mandibular wax rim � Now the maxillary record base is placed in the oral cavity Jain M. Impression techniques for the resorbed mandibular arch: A guide to increased stability. J Sci Soc 2015; 42: 88 -91.
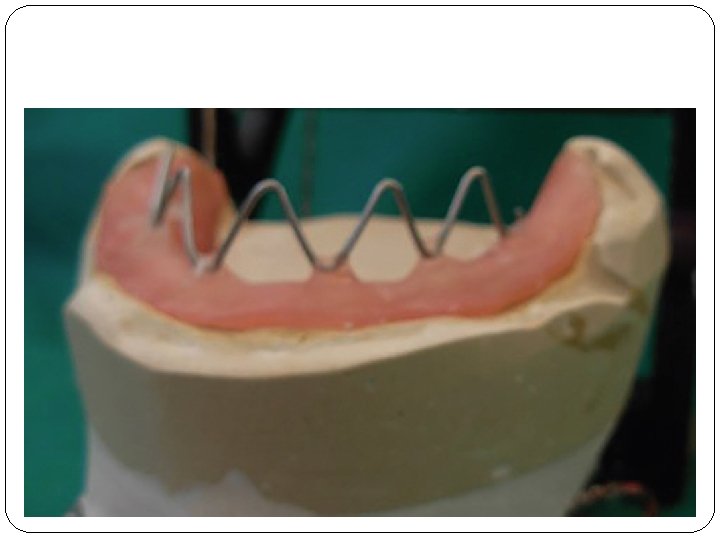

� Functional impression material is placed within these loops on the lower record base and it is placed within the oral cavity � The patient is instructed to say words like “ooo”, “aaa”, and “eee”. Pronouncing these words leads to recording of neutral zone existing in the mouth � Functional impression is added incrementally at regular intervals in these loops till the time the record base shows adequate retention within the mouth Jain M. Impression techniques for the resorbed mandibular arch: A guide to increased stability. J Sci Soc 2015; 42: 88 -91.

Jain M. Impression techniques for the resorbed mandibular arch: A guide to increased stability. J Sci Soc 2015; 42: 88 -91.

� Plaster indices are poured around the recorded neutral zones and thereafter, the loops are dismantled from the record base � After placing these indices, a new occlusal rim is made within the area of plaster indices, which serves as a guide for future teeth arrangement Jain M. Impression techniques for the resorbed mandibular arch: A guide to increased stability. J Sci Soc 2015; 42: 88 -91.

Jain M. Impression techniques for the resorbed mandibular arch: A guide to increased stability. J Sci Soc 2015; 42: 88 -91.

Classification of Oral Candidosis �Classifications: acute or chronic, oral or extraoral �Acute: �Psuedomembranous �Erythematous (atrophic) �Chronic �Psuedomembranous �Erythematous (atrophic) �Hyperplastic (candidal leukoplakia) 3 rd edition Oral and maaxillofacial pathology, Neville page: 414 -418

Candida-associated denture stomatitis in type 2 diabetes mellitus Barbara Dorocka-Bobkowska a, *, Dorota Zozulinska-Ziolkiewicz b, Bogna Wierusz-Wysocka b, Wieslaw Hedzelek a, Anna Szumala-Kakol c, Ejvind Budtz-Jo¨rgensen d i a b e t e s r e s e a r ch and c l i n i c a l p r a c t i c e 9 0 ( 2 0 1 0 ) 8 1– 8 6 �Objective: To describe the clinical appearance of Candida-associated denture stomatitis (DS) in subjects with type 2 diabetes (T 2 DM). The relationships between the types of DS, oral complaints and associated conditions were assessed in terms of glycemic control as determined by glycated hemoglobin (Hb. A 1 c) measurements.

�Conclusions: Diffuse type of inflammation was associated with T 2 DM. BS and DOM were the most common oral complaints. Inadequately controlled diabetes with Candida-associated DS was linked to a high incidence of an extensive type of inflammation, oral complaints and associated conditions.

TREATMENT �Topical and systemic administration of nystat is done in conventional cases �In immunosuppressed patients systemic administration of amphotericin-B and fluconazole necessary �Removal of primary etiological factor and improved oral hygiene is essential Text book of Oral pathology, Purkit page 246 -256

Dental Caries � DEFINITION Dental caries is a microbial disease of the calcified tissues of the teeth, characterized by demineralization of the inorganic portion and destruction of the organic substances of the tooth. -SHAFER Essentials of Preventive and Community Dentistry. Soben Peter.

MODIFIED KEY’S DIAGRAM HOST MICRO FLORA SUB STRATE TIME

SALIVA Lysozyme Amylases, Cystatins, Histatins, Mucins, Peroxidases Cystatins, Mucins Anti. Bacterial Carbonic anhydrases, Histatins Buffering Anti. Viral Digestion Salivary Functions Anti. Fungal Mineralization Histatins Tissue Coating Amylases, Cystatins, Mucins, Proline-rich proteins, Statherins Lubrication &Viscoelasticity Amylases, Mucins, Lipase Cystatins, Histatins, Prolinerich proteins, Statherins Mucins, Statherins

Key salivary Factors in dental caries Factors associated with low caries Factors associated with high caries High flow rate Low flow rate Proper salivation Xerostomia Normal Viscosity Too High or too low viscosity Buffering capacity Lack of salivary action Salovary enzymes Salivary glycoprotiens may contribute plaque accumulation Salivary Immunoglobulins Sucrose in saliva may be used up by the plaque bacteria to produce caies Remineralization Direct antibacterial action

MICROBIOLOGY OF DENTAL CARIES �Three carieogenic Bacteria �Actinomyces �Lactobacilli � L. Acidophilus, L. Casei �Mutans Streptococci �S. mutans, S. Sobrinus, S. Sanguinus, S. Salivarius, S. Milleri Essentials of Preventive and Community Dentistry. Soben Peter.

Prosthodontic consideration �Dental caries may increase due to xerostomia thus if possible full coverage crowns should be given �Choosing of abutment teeth Vernillo AT. Dental considerations for the treatment of patients with diabetes mellitus. J Am Dent Assoc 2003; 134: 24 -33.

Mucosal Disorders: Ø Disorders of the oral mucosa commonly occurring in diabetic patients include atrophy of the mucosa, candidiasis (thrush), and lichen planus or lichenoid mucositis. Ø These disorders are related to chronic salivary hypofunction and to the generalized immune dysfunction seen in diabetic patients. Guggenheimer J et al. : Insulin-dependent diabetes mellitus and oral soft tissue pathologies: II. Prevalence and characteristics of Candida and Candidal lesions. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 89: 570– 576, 2000

Oral Lichen Planus and Lichenoid Drug Reactions: Ø Although its exact etiology is not known, the presence of OLP has been frequently associated with diabetes Ø Mucosal changes called lichenoid drug reactions occur as an adverse side effect to medications that diabetic patients are commonly prescribed. These include antihyperglycemic and antihypertensive medications. Romero MA, Seoane J, Varela-Centelles P, Diz-Dios P, Garcia-Pola MJ : Prevalence of diabetes mellitus amongst oral lichen planus patients: clinical and pathological characteristics. Med Oral 7: 121– 129, 2002

Poor Oral Wound Healing : Ø Poor soft tissue regeneration and delayed osseous healing in patients with diabetes are known complications in DM pts. Ø It is reported that delayed vascularisation, reduced blood flow, a decline in innate immunity, decreased growth factor production, and psychological stress may be involved in the protracted wound healing of the oral cavity mucosa in patients with diabetes The mechanism of protracted wound healing on oral mucosa in diabetes. Review. Abiko Y, Selimovic D Bosn J Basic Med Sci. 2010 Aug; 10(3): 186 -91.

THE MECHANISM OF PROTRACTED WOUND HEALING ON ORAL MUCOSA IN DIABETES. REVIEW Yoshihiro Abiko 1* and Denis Selimovi, BOSNIAN JOURNAL OF BASIC MEDICAL SCIENCES 2010; 10 (3): 186 -191 � This review article summarizes reports on the wound healing in diabetes and discusses the mechanism of the protracted wound healing of the oral mucosa in diabetes �What they concluded was decreases in growth factor production, and psychological stresses may be involved in the Delayed vascularization, reduction in blood flow, decline in innate immunity, protracted wound healing of the oral mucosa in diabetics.

PROSTHETIC CONSIDERATION FOR ORAL ULCER �In case of oral ulcerations remove dentures during the active phase. Topical anaesthetic rinses, medications are prescribed �If the ulcerations caused by denture it has to noticed

DIABETES IN IMPLANT FAILURE �Significance �Liability of infection due to fragility of vessels so as to alter blood supply �Impaired wound healing

�Surgical stress can release endogenous norepinephrine which can cause significant increase in plasma glucose level

� Prevention �Screen patients for diabetes �If patient is diabetic get medical consultation �If uncontrolled, treatment postponed till condition is under control �Preoperative antibiotic prophylaxis, aseptic technique, atraumatic tissue handling and frequent and close follow up

Micha Peled et al , Implant Dent 2003; 12: 116 – 122 �Systemic factors, such as diabetes mellitus, can influence the success rate of dental implants. �The authors describe their experience using the MIS implant system (Medical Implant System, Shlomi, Israel) for retention of overdentures in patients with type 2 diabetes mellitus and provide data regarding the level of satisfaction of the patients, the improvement of function, mucosal and periimplant health, and bone level around implants in this group.

�The clinical outcome of dental implants in a selected group of patients with well-controlled type 2 diabetes mellitus is satisfying and encouraging.

Influence of diabetes on implants: A retrospective study PSG PRAKASH, DHAYANAND J VICTOR �Aim: The aim of the study reports on the influence on surgically placed implats �Conclusion: The result of this retrospective study indicate that a high success rate is achievable when dental implats are placed in diabetic patients whose diseases are in control

Implant Survival in Patients With Type 2 Diabetes: Placement to 36 Months Harold F. Morris, *†‡ Shigeru Ochi, *‡ and Sheldon Winkler Ann Periodontol 2000; 5: 157 -165. � This study attempted to determine if Type 2 diabetes represents a significant risk factor to the long-term clinical performance of dental implants. � Conclusion: Type 2 diabetic patients tend to have more failures than non-diabetic patients; however, the influence was marginally significant. These findings need to be confirmed by other scientific clinical studies with a larger Type 2 diabetic sample size.

PROSTHETIC CONSIDERATION � Implant dentistry is not contraindicated in most diabetics � Diabetics patients with blood glucose levels of around 100 Mg/dl � Sedative procedures and antibiotics. � Need for a stress reduction protocol, diet evaluation before after surgery � Corticosteroids, often used to decrease edema, swelling and pain may not be used in the diabetic’s patient. � Detrimental effects of diabetes on osseointegration can be modified using amino guanidine systemically Prosthodontic Management Of Patients With Diabetes Mellitus Gagandeep Kansal, Deepal Goyal J Adv Med Dent Scie Res 2013; 1(1): 3844.

Denture Stomatitis • Denture stomtatis is a generalized inflammation of the area underneath your denture, usually the palate. It is sometimes also called, 'denture sore mouth' even though it very rarely causes soreness. • It is a common problem found in 30 -60% of full denture wearers. Denture stomatitis affects women four times more than men and is much more likely to be found under the top denture than the bottom. It can be found under both partial and complete dentures. Mandana Khatibi 1, Zohre Amirzadeh 2, Majid Sadegh Pour Shahab 3, Iraj Heidary 4, Azad Estifaee 5, J. Appl. Environ. Biol. Sci. , 5(12)284 -287, 2015

What Causes Denture Stomatitis Night time denture wear. If you wear your dentures all day and all night, your gums rarely get a chance to breathe giving the perfect environment for the canidida to grow undisturbed. High sugar diet. This provides food for the candida, allowing them to grow and multiply. Mandana Khatibi 1, Zohre Amirzadeh 2, Majid Sadegh Pour Shahab 3, Iraj Heidary 4, Azad Estifaee 5, J. Appl. Environ. Biol. Sci. , 5(12)284 -287, 2015
. Your saliva provides natural protection against infection and lubricates your mouth")
Dry mouth (Xerostomia). Your saliva provides natural protection against infection and lubricates your mouth to stop dentures from traumatizing your gums. Without it you are more prone to getting problems. There are various things you can do to help improve the situation, though it will depend on the cause of the problem. Systemic problems. Diabetes, Medication- broad spectrum antibiotics, Steroids, Cytotoxic drugs (cancer drugs), Nutritional deficiences- iron, vitamin b 12, folic acid Mandana Khatibi 1, Zohre Amirzadeh 2, Majid Sadegh Pour Shahab 3, Iraj Heidary 4, Azad Estifaee 5, J. Appl. Environ. Biol. Sci. , 5(12)284 -287, 2015

What is the Treatment for Denture Stomatitis? • Pop your denture in a mild hypochlorite solution for up to twenty minutes. This solution is most effective at killing plaque and cleaning your denture • Leave dentures out at night • Try to watch the sugar in diet and eat a little less. Mandana Khatibi 1, Zohre Amirzadeh 2, Majid Sadegh Pour Shahab 3, Iraj Heidary 4, Azad Estifaee 5, J. Appl. Environ. Biol. Sci. , 5(12)284 -287, 2015

• If trauma from an ill fitting denture is a problem, • An antifungal, such as amphotercin B, nystatin or miconazole can be useful, but it is important that the underlying causes are treated, or when the drug therapy is stopped, the denture stomatitis will re-occur. • If it is suspected that you have systemic factors contributing to the problem, then you may need to see your medical doctor to get these investigated. Mandana Khatibi 1, Zohre Amirzadeh 2, Majid Sadegh Pour Shahab 3, Iraj Heidary 4, Azad Estifaee 5, J. Appl. Environ. Biol. Sci. , 5(12)284 -287, 2015

Examining the relationship between type II diabetes with denture stomatitis Mandana Khatibi 1, Zohre Amirzadeh 2, Majid Sadegh Pour Shahab 3, Iraj Heidary 4, Azad Estifaee 5, J. Appl. Environ. Biol. Sci. , 5(12)284 -287, 2015 This study aimed to determine the relationship between suffering from type II diabetes and then development of denture stomatitis on clients who came to the Iran University of Medical Sciences Endocrine Center, and was designed and implemented in a certain timeframe.

CONCLUSION Finding a significant relationship between type II diabetes and the prevalence of denture stomatitis can attract dentists to their role in detecting diabetes among the denture stomatitis patients. Moreover, The collaboration between physicians and dentists in taking care of patients with uncontrolled type II diabetes who are likely at risk of denture stomatitis, can reduce these patients problems.

ANTIBIOTIC CONSIDERATION Ø It is strictly recommeneded as prophylactic coverage for diabetic patients Ø Defective leucocytic function Ø Decreased Chemotaxis and phagoctosis Ø Decreased Bactericidal activity Ø Higher infection Rates
 then 500 mg QID, 4 days • Erythromycin-")
Regime • Pencillin V-1000 mg (stat) then 500 mg QID, 4 days • Erythromycin- Pencillin sensitivity • Avoid Glucocorticoids • For Type I Diabetic patients who are on hypoglycemic drugs on sulphonylurea drugs, salicylates should be avoied for preventing drug interactions

ANAESTHETIC CONSIDERATIONS • Excessive quantities of epinephrine should be avoided • It can accomplished by using 1: 100, 000 concentration of epinephrine • Choice of anaesthtics ØShort duration- Lidocaine &mepivacaine, ØLong duration- combination of ØMepivacaine& Levonordefrin ØRavocaine, Norepinephrine bitartrate
 Medical history : · Take history and")
PROSTHODONTIC MANAGEMENT OF DIABETIC DENTAL PATIENT 1) Medical history : · Take history and assess glycemic control at initial appt. · Glucose levels · Frequency of hypoglycemic episodes · Medication, dosage and times. 2) Establishing the levels of glycemic control early in the treatment process: · Patients recent glycated Hb values Prosthodontic Management Of Patients With Diabetes Mellitus Gagandeep Kansal, Deepal Goyal, J Adv Med Dent Scie Res 2013; 1(1): 38 -44.
 Stress Reduction : · Endogenous production of epinephrine and cortisol increase during stressful")
3) Stress Reduction : · Endogenous production of epinephrine and cortisol increase during stressful situations. · Profound anesthesia reduces pain and minimizes endogenous epinephrine release. · Conscious sedation should be considered for extremely anxious patient. 4) Oral hygiene instructions, frequent prophylaxis & monitoring of periodontal health, as there is increased risk of periodontal disease. 5) Treatment: The use of antibiotics in case of infection and Diet Modification. Prosthodontic Management Of Patients With Diabetes Mellitus Gagandeep Kansal, Deepal Goyal, J Adv Med Dent Scie Res 2013; 1(1): 38 -44.

Appointment Timings · Diabetic patients can receive dental treatment in the morning. · But, it is generally best to plan dental treatment to occur either before or after periods of peak insulin activity. a. 30 -90 min after injecting Lispro Insulin. b. 2 – 3 Hours after injecting regular insulin c. 4 -10 hours after injecting Lente Insulin Prosthodontic Management Of Patients With Diabetes Mellitus Gagandeep Kansal, Deepal Goyal, J Adv Med Dent Scie Res 2013; 1(1): 38 -44.

EMERGENCY MANAGEMENT FOR HYPOGLYCEMIC SHOCK I. Administer oral carbohydrates orange juice, soft drinks, candy II. If no recovery is apparent within 2 -5 min I. Administer 50 ml 5% dextrose intavenously II. Administer 1 mg glucagon i. m followed by 0. 5 mg epinephrine (1: 1000 considerations) Stanley Malamed – Medical emergencies in the dental office. Page 178 -164

EMERGENCY MANAGEMENT FOR HYPERGLYCEMIC SHOCK I. Basic life support Procedures I. Maintain open airway II. Administer 100% O 2 if necessary III. Administer i. v fluids to prevent vascular collapse II. Activate Medical alert & Transport to hospital III. Administer insulin under controlled conditions Stanley Malamed – Medical emergencies in the dental office. Page 178164

Dental management of diabetes For NIDDM � All procedures can be performed if blood glucose levels are under control �No Special precautions needed unless complications of diabetes present Stanley Malamed – Medical emergencies in the dental office. Page 178 -164
 Morning appointment preferred. Also short appointments and mid appointments food break")
For IDDM a) Morning appointment preferred. Also short appointments and mid appointments food break are preferred b) Advise the patient to take insulin dosage and normal meals on day of aental appointment c) Advise patient to inform operator if symptoms of insulin reaction occur d) Have source of glucose available e) Premedication of Diazepam preferred f) Tissue Mainpulation should be minimized Stanley Malamed – Medical emergencies in the dental office. Page 178 -164

SUMMARY

CONCLUSION �Management of diabetic dental patient should focus on periodontal health & the delivery of comprehensive dental care with minimal disruption of metabolic homeostasis & recognition of diabetic co morbidities.

REFERENCES : v. TEXT BOOK ORAL MEDICINE- BURKETT v. TEXT BOOK OF ORAL MEDICINE – GHOMS v. JOSLIN’S DIABETES MELLITUS, THIRTEENTH EDITION v Stanley Malamed – Medical emergencies in the dental office. v Little and Falaces – Dental Management of the medically compromised patient v Sonis Fazio and Fang – Principles and practice of oral medicine v Harsh Mohan – Pathology v. BONE HEALING AT A FAILED IMPLANT SITE IN A TYPE II DIABETIC PATIENT: CLINICAL AND HISTOLOGIC EVALUATIONS: A CASE REPORT Jun-Beom Park, Journal of Oral Implantology, Vol. XXXIII /No. One/2007 v. Molecular aspects of wound healing in diabetes Mc. Lennan S • Yue DK • Twigg SM

� Molecular aspects of wound healing in diabetes Mc. Lennan S • Yue DK • Twigg SM � Implant Survival in Patients With Type 2 Diabetes: Placement to 36 Months Harold F. Morris, *†‡ Shigeru Ochi, *‡ and Sheldon Winkler � The impact of diabetes on the success of dental implants and periodontal healing, Wings T. Y. Loo 1, L. J. Jin 1, Mary N. B. Cheung 1 and Min Wang 2* � RESIDUAL RIDGE RESORPTION : A REVIEW Dr. AJAY GUPTA , Dr. BHAWANA TIWARI, Professor, Dr. HEMANT GOEL HIMANSHU SHEKHAWAT � Association of type 2 diabetes mellitus with the reduction of mandibular residual ridge among edentulous patients using panoramic radiographs Osama Al-Jabrah

�Candida-associated denture stomatitis in type 2 diabetes Mellitus Barbara Dorocka-Bobkowska a, *, Dorota Zozulinska-Ziolkiewicz b, Bogna Wierusz. Wysocka b, Wieslaw Hedzelek a, Anna Szumala. Kakol c, Ejvind Budtz-Jo¨rgensen �Dental considerations for the patient with diabetes �Silvia Martí Álamo 1, Yolanda Jiménez Soriano 2, Mª Gracia Sarrión Pérez 3 �Dental implants and diabetes mellitus—a systematic review, Hendrik Naujokat*, Burkhard Kunzendorf and Jörg Wiltfang �Dental Implants in the Diabetic Patient: A Retrospective Study, Thomas J. Balshi, Glenn J. Wolfinger

�Diabetes Mellitus: A concern for Prosthodontic care Talib Amin Naqash, International Journal of Clinical Cases and Investigations 2013. Volume 5 (Issue 3), 30: 33, 1 st October 2013 � Effects of diabetes on the osseointegration of dental implants Ana Mellado Valero , Juan Carlos Ferrer García , Agustín Herrera Ballester, Carlos Labaig Rueda, Med Oral Patol Oral Cir Bucal 2007; 12: E 3843. �Effects of glycemic control on saliva flow rates and protein composition in non-insulin-dependent diabetes mellitus, Michael W. J. Dodds, Anne P. Dodds, (Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1997; 83: 465 -70)
- Slides: 139