Diabetes The Everchanging Scene Brian R Tulloch MD

Diabetes The Everchanging Scene Brian R Tulloch. MD Diagnostic Clinic Past President, American Diabetes Assoc’n Texas

This is a CME Program The opinions are those of the speaker -Received research grants from Sanofi, Abvie, Novo, BMS, Pfizer and others -Consulted for BMS, Pfizer, Squibb-Novo Sanofi -Lecture panel for Upjohn, Pharmacia, Lilly, BMS, Pfizer, Abvie, Novo-Nordisk, etc. -Fields of diabetes, hypertension, impotence, hyperlidipemia, platelet function, fertility control, thyroid, pituitary and adrenal function

Diabetes-The Everchanging Scene 1 -What is diabetes? 2 -Some useful statistics DM in the US, in minorities The challenges of DM -Prevention -Treatment 1 & 2 -Type 2 & Cardio-Vascular Disease -Future trends-& new ideas

What is Diabetes? 2 nd Century AD “Diabetes is a wonderful affliction among men…. being a melting down of flesh and limbs into urine…. . Life is short, disgusting and painful, thirst unquenchable, death inevitable…” Araeteus the Cappadocian, 2 nd Century AD

Definition of Diabetes 21 st. C Rule of two’s -Casual glucose >200 + Symptoms(polyuria, P-dipsia + unexplained wt loss) -Fasting glucose >126 mg/dl. -2 -hr glucose >200 on Oral glucose test -Elevated Hb. A 1 c > 6. 5% <5. 7%=N

Diabetes prevalence rates-USA 2017 -30. 3 million Pre-diabetes 2017 -84 million Increased in Native Americans. Pima 50% by aet 50 Higher in Hispanics, Blacks, Asians


Mortality in People With Diabetes: Causes of Death

Mortality Attributable to Diabetes

Normal Regulation of Blood Glucose

ADA-Types of Diabetes, Type 1: Auto-immune rejection of the pancreatic beta cells Onset in youth, can occur at any age, HLA markers Progressive damage to insulin supply -Sudden onset, + ketosis/coma. Rare in each family, But other auto-immune diseases. Thyroid, Adrenal, RA, Celiac disease, PAnemia etc Only treatment is insulin replacement. By injection/ ? inhalation. Immune suppression so far ineffective

Discovery of Insulin 1921 Banting, Best and Marjorie l
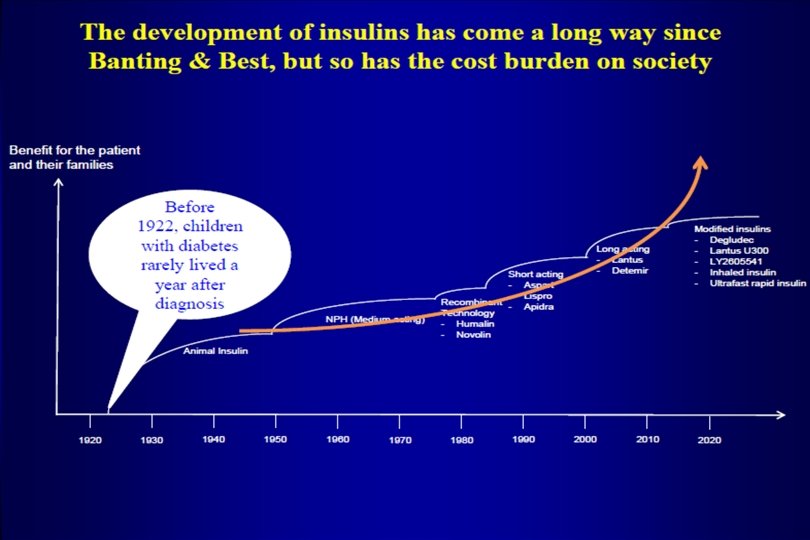

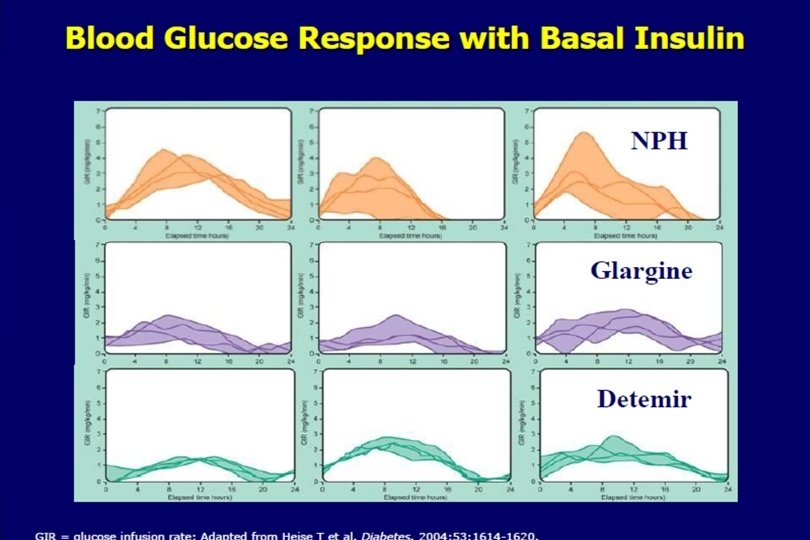
Treating Type 1 • Insulins-use the best • 1 - Long-acting- Tresiba/Levemir-(soluble, very stable effect day to day, less hypo’s) • >Tujeo, Lantus, Basalglar (ph 4) • (these ppt SQ, with variable tissue - absorption rates & more hypo’s) • But all are $$$, + need a scrip Cheapest- NPH-action very variable ($25), no scrip needed
 Onset = 2 -4 hours, ~25 -hour half-life Duration of action")
Insulin Degludec (Tresiba) Onset = 2 -4 hours, ~25 -hour half-life Duration of action at least 42 hours Steady state in ~3 -4 days O N 6 HN Degree of variability in glucose lowering over 24 hours is one fourth that of Glargine U 100 (20% vs 84%) so less hypo’s Garber AJ. Diabetes Obesity Metab; [Epub ahead of print; published online 31 Oct 2013]. Owens DR, et al. Diabetes Metab Res Rev. 2014; 30: 104 -119. Heise et al. Diabetes Obes Metab. 2012; 14: 859 -864 HO 2 C CO 2 HH O
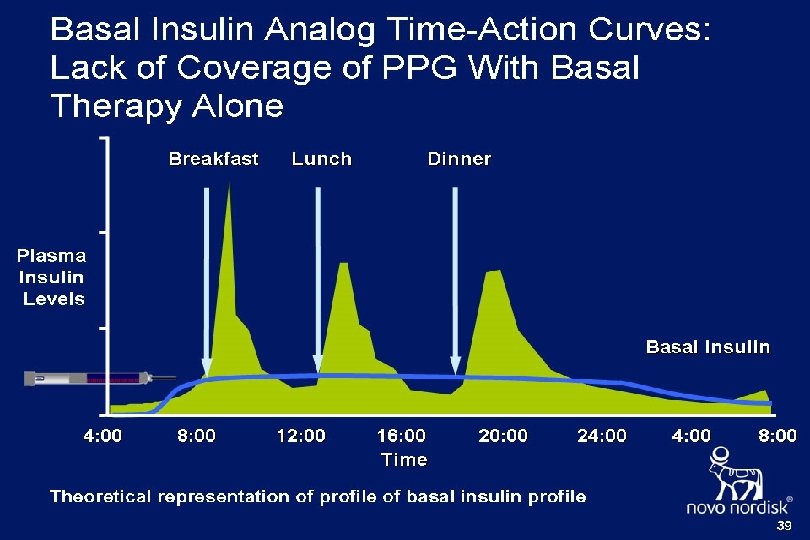

Treating Type 1 • Meal Time Insulins • Best-Novolog-, Humulog, Apidra • can be taken with meals, use in proportion to BS & mealtime carbs. • But-are $$$, + need a scrip. • Also R—Regular • Cheap-$25, no scrip • But-has to be taken 1/2 hr before meal

Treating Type 1 Ideal set-up • Long-acting Insulin Titrate Tresiba to wake-up glucose of 80 -120 Start with 10 U expect (15 - 2, 500 U/day) • Short-acting Insulins Add a dose of analog proportional to prevailing BS & mealtime carbseg- 1 Unit/12 -20 gms carbs • Check sugar before next meal.

Fine tuning Type 1 -tools • 1 -Home glucose monitor- reads in 5 secs • How many sticks? Know the levels 24 hrs Some Insurance will cover 5 -6/day • Continuous glucose monitor (SMBG)- eg Dexcom- stable reading monitoring for 7 -14 days. - (Insurance will now cover SMBG)
 • Avoid Low sugars • Pocket glucose, Granola")
Fine tuning Type 1 Issues (1) • Avoid Low sugars • Pocket glucose, Granola bar • Glutose tube-rapid absorption • Family member-Glucagon shot • Risky times for low sugars • Unaccustomed exercise, missed meal • Pure alcohol (switches off liver production of glucose)
 • Avoid High sugars • 1 -Xs food,")
Fine tuning Type 1 Issues (2) • Avoid High sugars • 1 -Xs food, esp carbs • 2 -Emotional Stress • 3 -Infection, fever • 4 -Hormonal cycle • Also when Pt Sick, no food/vomiting -if sugars high, may need 2 -3 X more insulin q-4 hrs to avoid ketoacidosis
 • Insulin Pumps ? ? ? Provide continuous")
Fine tuning type 1 Issues (3) • Insulin Pumps ? ? ? Provide continuous infusion under skin Basal-1 Unit/hr, less at night<dawn Bolus- 1 Unit/15 Gms carbs • But $$$ ($5 -6 K to buy, $1800/yr to run) if disconnected rapid rise in BS Comparison-Pumps are rarely better than the best combo of basal/Bolus- (so only use if requested!)
 -No FDA clearance yet) Addition of a")
Fine tuning type 1 New Issues (4) -No FDA clearance yet) Addition of a GLP-1 (eg Victoza-14 pts) 1 -drop in Insulin dose (30%) 2 -Less hypoglycemia and glucose variability 3 -Wt loss of 10 lbs 4 -better glucose control (Hb. A 1 c 6. 5 -6. 1%) Addidtion of a SGLT 1 +2 (Sotaglifoxin- 1400 pts, 24 wks) 1 -Lower Hb. A 1 c (down -0. 43%) 2 -Weight loss of 6. 4 lbs 3 -No change in hypoglycemia BUT 1 -More perineal yeast (6. 4% vs 2. 1%), gut gas ++ 2 -More Dehydration (1. 9% vs 0. 3%) & Ketoacidosis (3. 4% vs 0. 7%)

 Lifetime")
Type 2 Diabetes 95% of our cases Onset in Adults (or obese youth) Lifetime of insulin resistance Minorities-MA’s, Asians-I+V, No HLA Slow onset--”a touch of sugar” slow progression, no ketosis-CVD & limb loss Traditional Treatment: Diet, exercise-/+ pills-1, 2 or 3 Insulin when pills fail.

Natural history of DM 2 • Progressive condition: • Insulin Resistance, Beta cell exhaustion, slowly progressive rise in sugars • Also -High Blood Pressure • -Hyperlipidemia- High T/G’s, Low HDL • -Central Obesity, (Apple vs Pear)

Type 2 --Common in families- cousins, G-parents - Especially seen with obesity & hypokinesis, - No HLA markers -Can be delayed by diet & exercise - Now +/- 17 medications for treatment -Can be “reversed” by wt loss Newer approach-? use GLP-1 shots earlier

Type 2 How should we treat now? • It is a Strongly Familial disease- So • Early detection of young relatives • ? screen for pre-DM in high schools • -Follow up Gestational mothers • -Check obese subjects, • PCOS-Hirsutism, acne, truncal obesity, irregular cycles, Infertility. • Acanthosis Nigracans-

Natural History of Type 2 Diabetes Thiazolidinediones, AGIs, Metformin Insulin SFU, Meglitinides Lifestyle Glucose Adapted from D Kendall, R Bergenstal. © International Diabetes Center. Post Meal Glucose 300 Fasting Glucose 200 100 50 Relative Function 300 Insulin Resistance 200 100 0 At risk for Diabetes -10 -5 Beta cell failure 0 5 10 15 20 Years of Diabetes Insulin Level 25 30

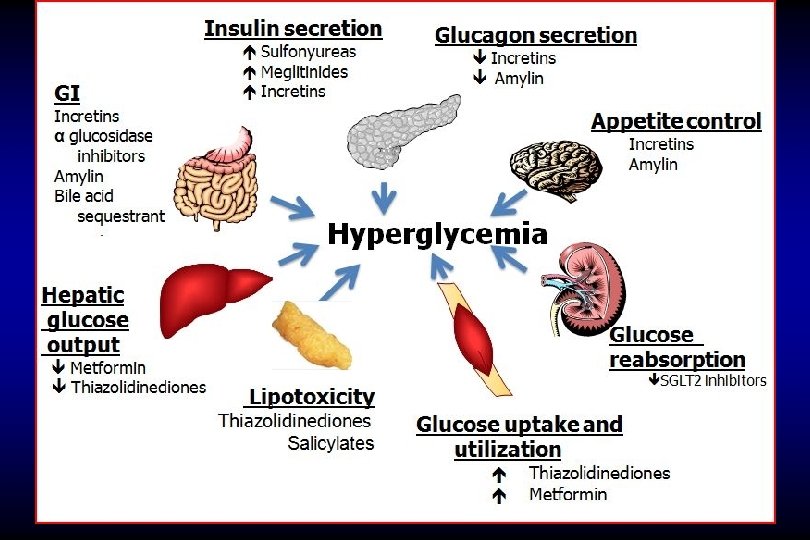
The Ominous Octet 8 Abnormailties in DM 2! Decreased incretin effect Increased lipolysis Decreased INS secretion HYPERGLYCEMIA Increased glucose reabsorption Increased glucagon secretion Increased HGP, hepatic glucose production. De. Fronzo RA. Diabetes. 2009; 58: 773 -795. Neurotransmitter dysfunction Decreased glucose uptake

Treatment of DM 2 New ideas • Start with the grand-kids! • Exercise-PT in schools • Diet-Fiber, Protein & Greens • Prevention-Pre-diabetes cases • DPP-Study Placebo, Rezulin, Metformin(33%), • Personal trainer (55%) • PCOS-Metformin < androgen, hair, >fertility.
 • 1*-Metformin-Use XR form (Less diarrhea)")
Drug options for DM 2 (*-have a future) • 1*-Metformin-Use XR form (Less diarrhea) • < CVD by 35% < Dementia, • < Cancer by 35%. • 2 -Sulfonyl. Ureas-Glipizide, etc • Early drop in sugar • Later burn-out of beta cells • 3*-Actos/Pioglitazone-(goodbye Avandia) • Slower drop in sugars • later preservation of insulin secretion •

Drugs for DM • 4 -? *SGLT 2 -Blockers of Kidney sugar re- absorption-lose 100 gms of sugar/day, Wt loss, drops Systolic BP & CCF but$$, 17% females, 7% males yeast. examples-Invokana, Jardiance, Farxiga, • 5 -DPP-4 inhibitors- Raise secretin, but not enough to affect satiety & no effect on CVD $$, only modestly effective Examples-Januvia, Tradjenta, Onglyza

Drugs for DM 6*-SGLT 1 -Oral blockers of gut glucose absorpt’n. Help with weight loss, cheap, effective, popular in Europe, but gas++ Examples-Miglitol, Acarbose, Sotaglifoxin(1&2) 7*-Oral blockers of Cholesterol absorption eg Welchol -drop chol + sugar 8*-Oral stimulators of brain dopamineeg Cycloset

Drugs for DM 2 • 9 -***GLP-1 s-V Potent, increase Insulin, decrease XS glucagon, correct 6/8 of DM 2 Induce satiety, effect is glucose dependent, so safe for long distant truck driversexamples Bydureon (Gila monster spit), Victoza, Ozempic (Human GLP-1) - some weekly, one oral (pending). Some reduce CVD • A Victoza analogue* is cleared for weight loss (Saxenda) • 10 -*Insulin- 50% loss of Insulin reserve at diagnosis so Basal insulin needed by 5 -15 yrs

Drugs for DM 2 • 11 -Weight Loss Surgery. Can produce 70 -80% “cure” of DM, so surgeons are claiming cost effectiveness for saving cost of DM, BP and Lipid meds within 3 -5 yrs! But no demonstrated CV reduction so far
 -greater reduction")
Type 2 therapy • 12*-Combinations- eg-a-Basal Insulin + GLP-1 Degludec +Liraglutide (Xultophy) -greater reduction in BS to <7 than Lantus +pc short-acting -at 1/2 total insulin dose -with 7 lbs wt loss b-SGLT 2+Metformin<BS + SBP control & others

T 2 DM subjects die of CVD!! Rawshani A, et al. N Engl J Med. 2017; 376: 1407 -1418.
 Improves CV Outcomes Marso SP, et al. N Engl J")
SUSTAIN 6 (GLP-1 Ozempic/Semaglutide) Improves CV Outcomes Marso SP, et al. N Engl J Med. 2016; 375: 1834 -1844.
 CV Death, MI and Stroke Patients With Event/Analysed Empagliflozin")
SGLT 2 EMPA-REG Trial: (Jardiance) CV Death, MI and Stroke Patients With Event/Analysed Empagliflozin Placebo HR (95% CI) P-value 3 -point MACE 490/4687 282/2333 0. 86 (0. 74, 0. 99)* 0. 0382 CV death 172/4687 137/2333 0. 62 (0. 49, 0. 77) <0. 0001 Non-fatal MI 213/4687 121/2333 0. 87 (0. 70, 1. 09) 0. 2189 Non-fatal stroke 150/4687 60/2333 1. 24 (0. 92, 1. 67) 0. 1638 Favors empagliflozin Cox regression analysis. MACE, Major Adverse Cardiovascular Event; HR, hazard ratio; CV, cardiovascular; MI, myocardial infarction. *95. 02% CI. Favors placebo
 1 -Metformin")
New Med Sequences for DM-2 (DM 2 s die of cardiovascular Disease) 1 -Metformin reduced CVD & Cancer by 35% (UKPDS), <Dementia 2 -GLP-1’s that reduce CVD-Victoza and Ozempic (Semaglutide) -don’t-Bydureon, all DPP 4’s 3 -SGLT-2’s that reduce CCF and CV death -Jardiance & Invokana 4 -A new SGLT 2 (Sotaglifoxin) also has SGLT 1 action (like Jardiance combined with Miglitol)
 • Appropriate")
Tight Control-in a perfect world • Access to regular medical care (FP’s>85%) • Appropriate medications, also to <CVD • Monitoring system- fingerstick sugar • 3 -4 monthly followup-goals are Hb. A 1 c<7%(6. 5), LDL<78, BP<130/80. • Preventive measures • Lipids- statins, PSK 9 • Blood pressure- ACE, ARB • Eye, foot : exam annually • Kidney: Micro-albumin annually.

Long-term issues with DM 2 The Ever-changing scene • Diabesity is now a major Public Health issue • Community Action is now advisable (like smoking) • Exercise should come back to our schools • USA restaurant sugar drink & food helping sizes should be matched to Europe • At-risk DM 2 subjects should now get early treatment • -Metformin for pre-diabetes • -GLP-1’s that reduce CVD should be added early with long-acting basal insulin for DM 2’s

Summary – The changing scene-1 DM 1 Watch families for auto-immune: RA, thyroid, adrenal, pernicious anemia, & HLA siblings • Foster good control using best insulins and close glucose measurement. Best- Tresiba and analogue short actings • Encourage insurance to cover CGM eg Dexcom • Artificial Pancreas just cleared by FDA ? Cost ? ? efficacy

Summary The Changing scene 2 DM 2 - A Familial Condition, No HLA • Prevention-early- diet, exercise for all. • Pre-diabetics(BS 99 -125)-Metformin ? +Pioglitazone +CVD sparing GLP-1 • Later- Basal Insulin+CVD sparing GLP-1 (Victoza/Ozempic &Tresiba-Xultophy. ) • Glucose absorption blockers-SGLT 1(gut-eg Miglitol) &2(kidney eg Jardiance) Both 1&2 Sotaglifoxin--Basal+SGLT 2 mixes (<CVD) • Goal-Hb. A 1 c <7%, & BP, TG, Chol controlled

If Clients ask whom to support in their wills • Remember the Diabetes Charities • American Diabetes Association-covers day-to-day support gps for DM patients. Govt issues (insurance coverage, etc). • Juvenile Diabetes Foundation-Raises funds for Diabetes Research, especially islet transplants, “Walk for the Cure”.

Thank You !!! B R Tulloch

Diabetes When things go wrong-1 • No insulin at all-FFA & Glucose both up -Ketosis • Glucose >1000 -dehydration • High FFA’s • Ketones –acetone++, breathlessness • Impaired consciousness • Treatment: Insulin, fluids, • look for ppt cause

Gone Wrong-2 • A Little insulin-FFA OK, Hyperosmolar Coma • High sugar >2000 • ? High triglycerides • Loss of consciousness, 30% stroke. • Treatment: Fluid++, Insulin, heparin, fix the ppt problem. Older adults-slow onset. Progressive dehydration

Gone wrong 3 Poor control- Few/no symptoms: Sugars 250 -300 for months/years Sugar sticks to body structures -Hb. A 1 c >9 -10%(N 4 -6%): -Eye- bloodvessels leak -Kidney- filtration system leaks -Peripheral nerves-legs lose feeling, arteries block up (esp smokers) -LDL-increased atheroma-CVD++
- Slides: 56