Diabetes Mellitus Pharmacology r Presented by Wanda Lovitz

Diabetes Mellitus Pharmacology r Presented by: Wanda Lovitz, APRN

Diabetes Pharmacology: Objectives l Discuss the nursing implications of oral anti-diabetes agents and injectable anti-diabetes agents including Byetta and insulins. l Describe teaching guidelines for clients receiving oral anti-diabetes agents, insulins, or glucose-elevating drugs. l Discuss the mechanisms of action, therapeutic uses, adverse effects, and interactions of the various type of agents for type 1 diabetes mellitus. l Discuss the mechanisms of action, therapeutic uses, adverse effects, and interactions of the various types of insulins.
…sulfonylurea glipizide (Glucotrol)…sulfonylurea metformin (Glucophage)… biguanide pioglitazone (Actos)… glitazone")
Drugs to Know l glyburide (Micronase)…sulfonylurea glipizide (Glucotrol)…sulfonylurea metformin (Glucophage)… biguanide pioglitazone (Actos)… glitazone (TZD) sitagliptin (Januvia)…incretin enhancer/DPP-4 l exanatide (Byetta)…incretin l l inhibitor mimetic/enhancer/GLP-1 agonist (INJECTABLE FOR TYPE II) Insulins: Novolog, Regular, NPH, Lantus & Levemir l Glucagon…glucose elevating drug used as tx for l HYPOGLYCEMIA

High blood sugar can cause many problems Type 2 Diabetes can lead to: Heart Disease Kidney Disease Eye Damage Foot Problems Nerve damage/neuropathy Depression Managing type 2 diabetes properly can help stop or slow down these problems

Agents used to treat Diabetes Oral Agents 1. 2. 3. 4. 5. Sulfonylureas Biguanides Thiazolidinediones (TZDs) DPP-4 inhibitors Combinations Insulins l l Novolog (rapid) Regular (short) NPH (intermediate) Lantus/Levemir (long) Injectable …but NOT insulin Incretin mimetic Agents to RAISE blood exenatide/Byetta 2. Dextrose 50% sugar 1. Glucagon

Normal blood sugar ranges
 Blood Sugar Goals (FOR THE DIABETIC): l 70 -130 mg/d.")
American Diabetes Association (ADA) Blood Sugar Goals (FOR THE DIABETIC): l 70 -130 mg/d. L before meals l Less than 180 mg/d. L two hours after starting a meal (2 H PP = 2 hours post prandial) l Less than 7% hemoglobin (A 1 C) level

What is a Hemoglobin A 1 C? l A serum blood test which measures the average glucose level over the preceding 2 -3 months l Is a better indicator of glycemic control over time than the FBS Note that a Hb. A 1 C of 6% corresponds to an AVERAGE blood sugar of 135

A better estimate of glycemic control over time: the Ha 1 C • Excess glucose attaches to RBC. • The life of a RBC is about 3 months

Target sites of the oral agents 1. 2. 3. 4. 5. 6. Pancreas Liver Intestine Adipose tissue Muscle Kidneys

Limitations of oral agents for TYPE II diabetics only! l Usually started after diet and exercise fail to adequately control blood sugars l Can typically reduce Hb. A 1 c by 0. 5 – 2. 0% l Mechanism of action addresses THE SYMPTOMS of diabetes rather than the underlying pathophysiology l Many UNDESIRABLE SIDE EFFECTS which often affects adherence (hypoglycemia, n/v, peripheral edema, weight gain) l BETA CELL FUNCTION TENDS TO WORSEN OVER TIME l Clinicians often fail to intensify therapy/start insulin to obtain good control

Wanda as a “Baby Nurse” Oral agents: nursing implications l Nursing implications – l monitoring of glucose levels and glycosylated hemoglobin (HA 1 C) l assessing for sulfa hypersensitivity (sulfonylureas) administering most agents with meals l understanding the onset of action, peak, and duration associated with oral agents l l assessing patient teaching needs l assessing for hypoglycemia

Patient Voices: Larry with Type II l http: //www. nytimes. com/interactive/2009/ 08/04/health/TE_DIABETES. html l Copy and paste the address above into your browser to hear several different patients talk about living with diabetes.

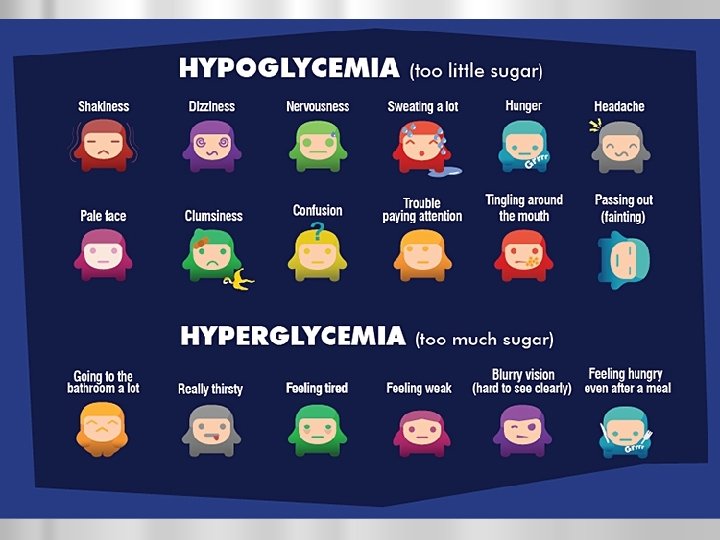
Hyperglycemia vs Hypoglycemia l Hyperglycemia High blood sugar l FBG levels of greater than 126 on 2 or more occasions=DM l l Insulin Resistance when FBG is greater than 100 but less than 126 l BG normally rises after food consumption l Should return to near normal in 2 H = 2 h. PP l Hypoglycemia Low blood sugar l Most people are symptomatic with when levels are below 60 l Diabetics may have ‘hypoglycemic’ reactions when BS drops after they receive anti-diabetic meds l Especially if oral intake is insufficient l
 act in pancreas to insulin production l l Think of")
SULFONYLUREAS l MOA: (1) act in pancreas to insulin production l l Think of sulfonylureas as “oral insulin” l l INSULIN SECRETOGOGUES Sulfonylureas increase insulin output from the pancreas Any agent that increases insulin output from the pancreas has the potential to cause hypoglycemia
, older, less potent drugs l Second-generation agents")
Sulfonylureas l First-generation agents – chlorpropamide (Diabinese), older, less potent drugs l Second-generation agents – (Micronase) l *glyburide l glipizide (Glucotrol) l glimepiride (Amaryl); newer, more potent drugs

SULFONYLUREAS l Adverse effects - nausea, vomiting, epigastric discomfort, heartburn, skin rash, HYPOGLYCEMIA, photosensitivity, hematologic problems (e. g. , hemolytic anemia), thrombocytopenia), WEIGHT GAIN l Contraindication: allergy to sulfa

Sulfonylurea: glyburide/Micronase l glyburide/Micronase is the most frequently prescribed 2 nd generation sulfonylurea l l Micronase has a slower onset and longer duration of action than another frequently rx sulfonylurea -*glipizide (Glucotrol) l These agents are beneficial in controlling glucose levels throughout the day and night glyburide/Micronase is sometimes used with glipizide/Glucotrol to better control glucose levels at meals = SYNERGISTIC EFFECT l Onset 1 – 1. 5 hours; peak 4 hours; duration 20 -24 hours

BIGUANIDE: metformin *THE most popular oral anti-diabetic agent in the U. S. l metformin (Glucophage) often used as monotherapy with type 2 diabetes l may also be used with a sulfonylurea l MOA: l (1) DECREASES HEPATIC GLUCOSE PRODUCTION and production of triglycerides and cholesterol from the liver l (2) enhances glucose transport into cells l l IMPROVES INSULIN SENSITIVITY by increasing peripheral glucose uptake and use (3) decreases glucose uptake in the intestine l SOME WEIGHT LOSS EXPECTED

MOA: metformin/Glucophage 1. intestinal absorption of glucose 2. hepatic glucose production 3. insulin sensitivity by glucose uptake in tissue Advantage over sulfonylureas: Since it has little to no effect on pancreatic output, NOT AS MUCH CONCERN WITH HYPOGLYCEMIA!
 peak 2 -4 weeks Adverse effects:")
BIGUANIDE: l Onset several DAYS l l (metformin/Glucophage) peak 2 -4 weeks Adverse effects: abdominal bloating l nausea, vomiting, DIARRHEA l l diarrhea can be uncontrollable; fecal incontinence issues for some l “Metformin moment” l risk for LACTIC ACIDOSIS in pts with creatinine l can be life threatening! l Nursing implications – recognize that it will not immediately lower BG l monitor serum glucose level l give 30 minutes before a meal l l Hold before any test which requires IV contrast dye d/t risk of lactic acidosis!!

THIAZOLIDINEDIONES /GLITAZONES or TZDS l MOA: 1. Decreases INSULIN RESISTANCE l does this by: 1. 2. increasing sensitivity of insulin receptors increaseing glucose uptake and use in skeletal muscle 2. Decreases fatty acid output in adipose tissue 3. Decreases glucose output in the liver

Insulin Resistance
 Adverse effects EDEMA")
TZD: pioglitazone/Actos l Available l l l agents pioglitzaone/Actos rosiglitazone (Avandia) Adverse effects EDEMA l weight gain l mild anemia l MAY CAUSE LIVER DAMAGE l l Onset unknown; peak unknown, duration 12 -24 hours

TZDs pioglitazone/Actos rosiglitazone/Avandia l ADVANTAGE of glitazones: l DOES NOT CAUSE HYPOGLYCEMIA since they do not have an affect on pancreatic production of insulin l PRESERVE SOME BETA CELL FUNCTION l May l MAY HAVE PROTECTIVE chlolesterol) VASCULAR effects (lowering DISADVANTAGE: may be toxic to the LIVER l Must have LFTs (ALT and AST) monitored
 l l Incretins are INTESTINAL HORMONES released")
Newest Class: Incretin MIMETICS: exenatide INJECTION (Byetta) l l Incretins are INTESTINAL HORMONES released in response to ingestion of food l Incretins increase the insulin response and depress the gluconeogenesis in the liver ↑insulin and ↓ glucose = lower BG l Incretins naturally decrease appetite NOTE: The incretin response is DIMINISHED in type II diabetics! l Incretin mimetics, mimic the response of endogenous incretin l So…. . Mimicking/enhancing the incretin response would result in lower glucose levels

exenatide/Byetta

exenatide/Byetta “Incretin Enhancer” l Given as a SQ INJECTION within 1 H of morning and evening meal (BID) l Major SE is NAUSEA AND HYPOGLYCEMIA Not a substitute for insulin!! l Serious SE: pancreatitis l l Should NOT be used in Type I DM!! l Is NOT to be used to treat DKA Average weight loss is 5 -10 pounds

DPP-4 INHIBITOR/incretin enhancer: sitagliptin/Januvia oral agent l A once a day l Is a DPP-4 inhibitor – Blocks DPP-4 l DPP-4 breaks down the hormone incretin l Low levels of incretin result in a DECREASE in the response from the pancreas and less insulin is secreted l Low levels of incretin also result in an increase in glucose output from the liver l Leading to. . . Hyperglycemia

MOA: sitagliptin/Junuvia l So…DPP-4 inhibitors slow the degradation of incretins thus prolonging the action of the incretins increasing/enhancing incretin levels l The result in an in output of insulin from the pancreas and a in glucose output from the liver l End result is lower glucose levels

DPP-4 inhibitors: MOA

Summary Slide: Effects of oral agents on diabetes
 l 1. 25/250; 2. 5/500; 5/500 l")
Combination Drugs: Many out there glyburide/metformin (Glucovance) l 1. 25/250; 2. 5/500; 5/500 l l rosiglitzone/metformin (Avandamet)

Summary Slide/ Side Effects of Antidiabetic Agents

Anti-diabetic Agents: the Insulins

INSULINS l Effects similar to the endogenous insulin produced from the pancreas l Primary treatment for type 1 diabetes l may also be used in the management of type 2 diabetes and gestational diabetes Various types of insulins: l l l rapid acting short acting intermediate acting long acting mixed l Pork, beef in the past l Now human source insulins l Human more effective, causes fewer SE and has a lower incidence of resistance

Which type of diabetic patients receive insulin? TYPE I DM and TYPE II DM

Insulin as the “key” • Insulin allows the glucose to get inside the cell • • Without insulin, the glucose stays in the bloodstream causing hyperglycemia
 l l")
RAPID ACTING INSULINS l Types of rapid acting insulins: l lispro (Humalog) l l aspart *(Novolog) Onset 0 -15 minutes!!! Peak 1 H l Duration 3 H l l Used with sliding scale regimens (SSC) “CORRECTION INSULIN” l “BOLUS INSULIN” l l Nursing implication risk for hypoglycemia by making sure that the meal is available before administering l Subcutaneous use: Humalog and Novolog l Intravenous use (Novolog only) l

SHORT ACTING INSULINS l Regular l Intravenous or subcutaneous use l Onset l 30 -60 minutes (sub-cu) Peak 2 -3 H l Duration l 4 -6 H Also used with SLIDING SCALE/CORRECTION REGIMENS
 forms Types include: l")
INTERMEDIATE ACTING INSULINS l l l Neutral Protamine Hagedorn (NPH) forms Types include: l *Humulin N and Novolin N Onset 1 -2. 5 hours l Peak 6 -14 hours Duration 18 -24 hours l CLOUDY insulin l NPH is given BID l NPH is normally given 30 min before 1 st meal of the day (2/3 dose) and (1/3 dose) before the evening meal or at bedtime. BID dosing

LONG ACTING “BASAL” INSULINS l l l Two types: l *glargine/Lantus l detemir/Levemir Onset 2 -4 hours; l Duration 24 hours l Closest insulin to the body’s own basal insulin Constant duration with NO DEFINED PEAKS l A basal or slow acting insulin Important note: Lantus and Levemir MUST NOT BE MIXED with any other insulin

MIXED/Combination Insulins l Developed to more closely stimulate varying levels of normal endogenous insulin production l Varying types – Humulin 70/30, 50/50, Novolin 70/30 l Contain varying amounts of intermediate and short acting insulin

INSULIN REGIMENS l BASAL/BOLUS INSULIN l Basal insulin: example: Lantus or Levemir provides “basal” coverage l usually once a day dose l l Bolus insulin: example: Regular or Novolog given before meals to “cover” elevated BS l FSBS or CHO count done to determine dose l l CORRECTION INSULIN/Sliding scale regimens (SSI/SSC)- regular insulin dosages are adjusted based on finger stick blood sugar(FSBS) l TYPICALLY AC AND HS l May or may not be used with a basal l

Comparison of action of NPH and Lantus Note that the Regular insulin peaks in about 3 H and is just about gone within 10 H. Note that the Lantus has no peaks and is present for about 24 H. Also, the action of Lantus most resembles the body’s own (endogenous) insulin.

The Ideal Insulin Regimen l Simulates the body’s own normal insulin output Combines “Basal” insulin with “mealtime” insulin l Is called a “basal-bolus” regimen l Bolus also known as “correction” insulin- it l corrects high BS before a meal- “sliding scale insulin” l Uses rapid- and short-acting (bolus) insulin before meals PLUS l l Uses a background insulin once a day Commonly prescribed as 4 injections a day: Lantus or Levemir at bedtime l Novolog or Regular before each meal l

Adverse Effects of Insulin l R/t hypoglycemia, hyperglycemia, or hyperinsulinemia l Localized allergic reactions at the injection site l Insulin Reaction l AKA: HYPOGLYCEMIA – occurs when there is more insulin in the blood than is needed for the amount of circulating glucose l Causes: Med error l Patient exercised and insulin peaked l Patient doesn’t eat after taking insulin l SX usually seen when BG 60 or less l l Generalized urticaria and swollen lymph glands

Insulin delivery methods Wireless pumps Insulin pens

GLUCOSE – ELEVATING DRUGS GLUCAGON & 50% DEXTROSE l MOA: STIMULATES hepatic production of glucose from glycogen stores. Used to treat hypoglycemia. l RAISES THE BLOOD SUGAR l Administered IM, IV, or SC l Indication: To treat hypoglycemic reactions l Adverse effects – nausea and vomiting, tachycardia, and anaphyaxis l **50% Dextrose (D 50 W) IVP is also given to raise low blood sugar for severe hypoglycemia**

Summary Slide: Hypoglycemia vs Hyperglycemia

TIME IS UP!
- Slides: 52