Diabetes Mellitus In Pregnancy Diabetes Mellitus In Pregnancy

Diabetes Mellitus In Pregnancy ������� �������

Diabetes Mellitus In Pregnancy Definition Epidemiology Pathogenesis Classification Screening Diagnosis Complications Treatment
 - type 1 insulin dependent - type 2")
Diabetes Mellitus ����������� ��� (glucose intolerance) - type 1 insulin dependent - type 2 noninsulin dependent The most common medical complication of pregnancy Gestational diabetes (GDM) : diagnosed during pregnancy Pregestational diabetes (Overt DM) : before pregnancy

Epidemiology ������ 2 -3 ����������� 90 ���� GDM Usually occur in 2 nd trimester

Classification Cla ss Onset Fasting Plasma Glucose 2 -hr Postpandrial Glucose The rapy A 1 Gestation <105 mg/dl And <120 mg/dl Diet A 2 Gestation >105 mg/dl And/or ≥ 120 mg/dl Insulin Class Age of Onset Duration (yr) Vascular Disease Therapy B > 20 < 10 None Insulin C 10 – 19 None Insulin D < 10 20 Benign Retinopathy Insulin F Any Nephropathy Insulin R Any PDR Insulin H Any Heart Insulin

Diabetes Mellitus In Pregnancy Overt : Random plasma glucose > 200 mg/dl ������� classical signs & symptoms (polydipsia, polyuria & unexplained wt. loss) Fasting glucose ≥ 126 mg/dl

Diagnostic test One-step approach : 100 g OGTT Two-step approach - 50 g GCT : ≥ 140 mg/dl (80%), : ≥ 130 mg/dl (90%) - 100 g OGTT Selective screening : ������� high risk ���� Universal screening : �����������

Risk Assessment for Detecting GDM Low Risk : blood glucose testing not routinely required Age < 25 yr Member of an ethnic group with a low prevalence of GDM No known diabetes in first-degree relatives Weight normal before pregnancy No history of abnormal glucose tolerance No history of poor obstetric outcome

Risk Assessment for Detecting GDM High Risk : ������������ �������� GA 24 -28 wks. ���������� GDM Age > 30 yr Marked obesity (20% more than ideal weight) First-degree relative with DM Previous GDM Previous large baby wt. > 4, 000 g Previous still birth, or a child with a birth defect, PIH Glucosuria Polyhydramnios

Risk Assessment for Detecting GDM Average Risk : ������� GA 24 -28 wks. Not in High risk and Low risk categories

Diagnostic criteria

�������� ������������ RDS Neonatal ������� hypoglycemia Neonatal ���������� hypocalcemia ����� Hyperbilirubinemia ������� Cardiomyopathy ��������� Polycythemia � hydramnios ����� (macrosomia)

Congenital anomaly in overt DM Anomaly Percent Caudal regression 252 Situs inversus 84 Spina bifida, hydrocephaly, or other CNS defect 2 Anencephaly 3 Heart anomalies 4 Anal/rectal atresia 3 Renal anomalies -Agenesis -Cystic kidney -Duplex ureter 5 4 4 23

�������� ����� Abortion Hypoglycemia Hyperglycemia Infection PIH Hydramnios ������������ PPH death

MANAGEMENT

�������� DIET EXERCISE INSULIN ORAL HYPOGLYCEMIC AGENT

DIET Goals : provide necessary nutrients for mother and fetus control glucose level prevent starvation ketosis
 Average = 1800 -2000 Kcal/d")
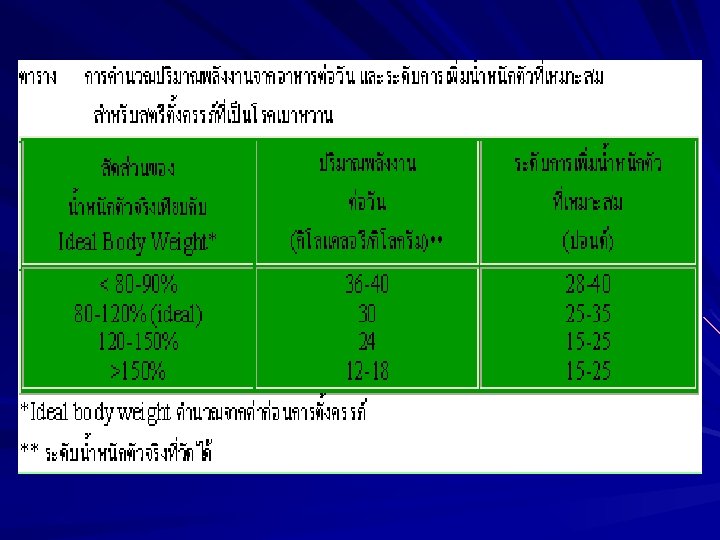
Diet control ������ Ideal body weight (30 -35 kcal/kg) Average = 1800 -2000 Kcal/d CHO : Protein : Lipid = 55 : 20 : 25 ���� 4 ���� /������� ����� 25/30/30/15 ��������� /������������ �� Cardiovascular – conditioning ���� aerobic exercise ���������������

Insulin ������������������� , ���� hypoglycemia ������ Used when FBS > 105 mg/dl persist despite diet control ���� Dx overt DM ������ admit ������� insulin ������������ Overt DM ��� intermediate + short-acting insulin – ������ mix-split dose ��� NPH + RI ���� /������� fluctuation ���� NPH: RI = 2: 1 (2/3 ��� total dose) ���� NPH: RI = 1: 1 (1/3 ��� total dose)

Goal ������ blood sugar Goal ���� BS mg/dl FBS 60 -90 Before lunch/dinner/snack After meal 1 hr 60 -105 ≤ 140 After meal 2 hr ≤ 120 From 2 -6 a. m. 60 -90

Diabetic ketoacidosis BS 200 -250 mg/dl ������� ��� Na Treatment – IV 2 lines ������ 1 ���� /��. �� 2 ��. ��� BS < 250 mg/kg/hr ������ 5% D/W – Insulin IV bolus RI 10 -20 U ������� Insulin drop 5 -10 U/hr – Potassium Within 2 -4 hr : ��������� Not to drop > 30 -40 m. Eq/hr – Bicarbonate Only in severe acidosis ( p. H<7. 0) Stop when p. H ≥ 7. 2

�������� GA 30 -32 wk Fetal movement count GDM : ���� NST 1 ����� /wk Overt DM : ���� NST 2 ����� /wk ����� nonreactive test ������� BPP ������� doppler ultrasound ����������� vasculopathy

����������� GA 38 wks. ������ GA ������������� DM �� lung maturity �������� L/S ratio (Lecithin/sphingomyelin) : >2 Foam stability test or Shake test PG level (phosphatidylglycerol level) : >3%

������� Labor induction is attempted when fetus is not excessively large, and the cervix is considered favorable C/S is common to avoid traumatic delivery of a large infant in class B or C and more advanced DM esp. with vascular disease (���� macrosomia, ������ > 4500 g)
mg/dl( 100 > 140 -")
LOW-DOSE INSULIN INFUSION FOR THE INTRAPARTUM PERIOD Blood glucose )mg/dl( 100 > 140 - 100 180 - 141 220 - 181 220 < Insulin Dosage )U/hr( Fluids (125 ml/hr) 0 1. 5 2. 0 2. 5 D 5 lactated Ringer Normal saline From ACOG (1994(

Table : postpartum evaluation 2 -hour, 75 -g oral glucose tolerance test plasma glucose(mg/d. L) Impaired Time tested No diabetes glucose tolerance Fasting < 115 < 140 Diabetes ≤ 140 ½, 1, 1½ hr All < 200 1 value ≤ 200 2 hr 140 -199 < 140 ≤ 200

- Slides: 45