Diabetes mellitus Diabetes is not one disease but

Diabetes mellitus

• Diabetes is not one disease, but rather is a group of syndromes characterized by an elevation of fasting blood glucose caused by a deficiency in insulin. • Diabetes mellitus is the leading cause of adult blindness amputation major cause of renal failure heart attacks strokes.
 Type 2 (noninsulin-dependent")
• Divided into 2 types Type 1 (insulin-dependent diabetes mellitus) Type 2 (noninsulin-dependent diabetes mellitus).
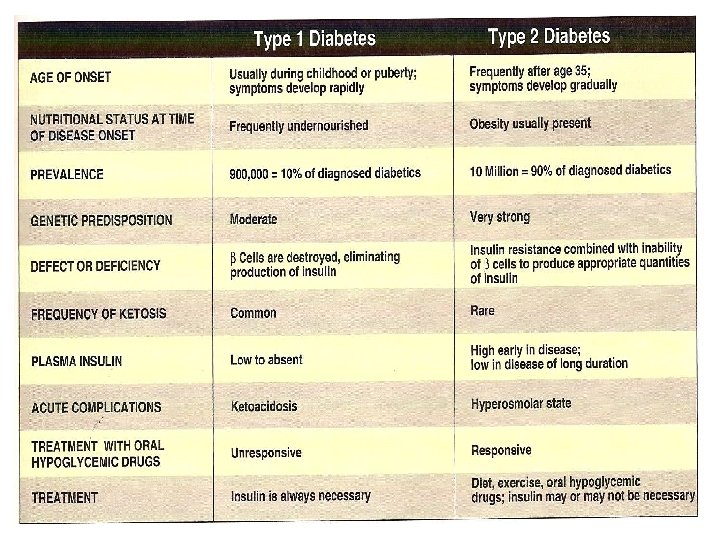

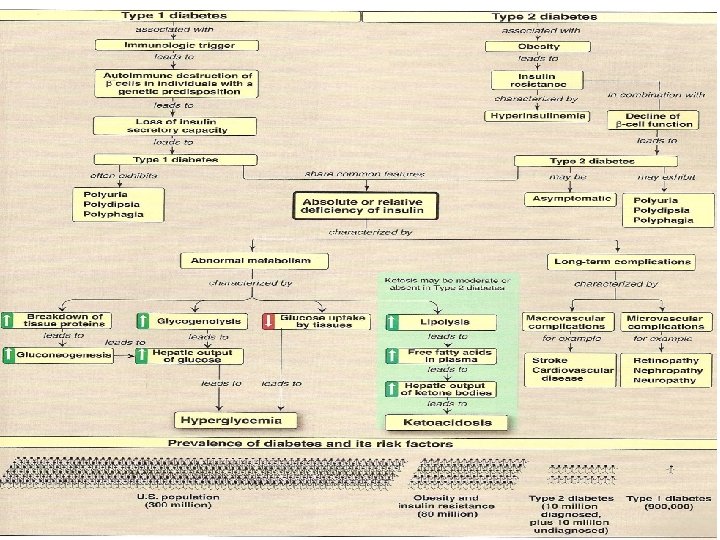
Type 1 Diabetes • Persons with Type 1 diabetes constitute ~10% of the ten million known diabetics in the US. • an absolute deficiency of insulin caused by an autoimmune attack on the β cells of the pancreas.

A porcine islet of Langerhans. The left image is a brightfield image created using hematoxylin stain; nuclei are dark circles and the acinar pancreatic tissue is darker than the islet tissue. The right image is the same section stained by immunofluorescence against insulin, indicating beta cells.

insulin resistance, your muscle, fat, and liver cells do not use insulin properly. The pancreas tries to keep up with the demand for insulin by producing more. Eventually, the pancreas cannot keep up with the body's need for insulin, and excess glucose builds up in the bloodstream. Many people with insulin resistance have high levels of blood glucose and high levels of insulin circulating in their blood at the same time.

• Over a years, the autoimmune attack on the βcells leads to gradual depletion of the β-cell population • symptoms appear unexpectedly when 80— 90% of the β cells destroyed. • At this point, the pancreas fails to respond adequately to ingestion of glucose • insulin therapy is needed to restore metabolic control and prevent life-threatening ketoacidosis.

• β-Cell destruction requires both: Øa stimulus from the environment (such as a viral infection) Øa genetic

Among identical twins, if one sibling develops Type 1 diabetes mellitus, the other twin has only a 30 — 50% chance of developing the disease. • In Type 2 disease the genetic influence is stronger, and in virtually all monozygotic twinships, the disease develops in both individuals.

A. Diagnosis of Type 1 diabetes • The onset of Type 1 diabetes is typically during childhood or puberty, and symptoms develop rapidly. • Patients with Type 1 diabetes can usually be recognized by the sudden appearance of polyuria polydipsia (excessive thirst) polyphagia (excessive hunger) fatigue weight loss weakness
 greater than or")
• diagnosis is confirmed by a fasting blood glucose (FBG) greater than or equal to 126 mg/dl, • accompanied by ketoacidosis. • Fasting is defined as no caloric intake for at least 8 hours. • If diagnosis of Type 1 diabetes is uncertain by clinical presentation, testing for circulating islet-cell antibodies is recommended. • Oral glucose tolerance test as a diagnostic tool for diabetes has fallen into disfavour because it is timeconsuming and the results are highly variable.

B. Metabolic changes in Type 1 diabetes • The metabolic abnormalities of diabetes mellitus result from a deficiency of insulin which deeply affects metabolism in three tissues: liver, muscle, and adipose tissue 1. Hyperglycemia and ketoacidosis: • Elevated levels of blood glucose and ketones are the feature of untreated Type 1 diabetes mellitus. • Hyperglycemia is caused by ↑hepatic production of glucose + diminished peripheral utilization.

Ketosis results from increased mobilization of fatty acids from adipose tissue, combined with accelerated hepatic fatty acid β-oxidation and synthesis of 3 -hydroxybutyrate and acetoacetate. Diabetic ketoacidosis (DKA, a type of metabolic acidosis) occurs in 25— 40% of those newly diagnosed with Type 1 diabetes, and may recur if the patient becomes ill (most commonly with an infection) or does not comply with therapy. DKA is treated by replacing fluid and electrolytes, followed by administration of low-dose insulin to gradually correct hyperglycemia without sudden hypoglycaemia.



Ketone bodies • are 3 water-soluble compounds that are produced as byproducts when FA are broken down for energy. • They are used as a source of energy in the heart and brain. In the brain, they are a vital source in fasting. • The 3 ketone bodies are acetoacetate, betahydroxybutyrate and acetone, although betahydroxybutyrate is not technically a ketone but a carboxylic acid.

• Ketocidosis means dangerously high levels of ketones. Ketones are acids that build up in the blood. They appear in the urine when your body doesn't have enough insulin. Ketones can poison the body. They are a warning sign that your diabetes is out of control or that you are getting sick.

Ketoacidosis • is a metabolic acidosis is caused by high concentrations of ketone bodies, formed by the deamination of amino acids, and the breakdown of fatty acids. • when the liver breaks down fat and proteins in response to need for respiratory substrate. • It can also occur with people undergoing hunger strikes, fasting over 3 days, or people starving to death as the body is forced to break down fat for sustenance due to their lack of outside nutrition.

• Ketoacidosis can be smelled on a person's breath. It is often described as smelling like fruit or paint thinner. • should not be confused with ketosis, which is one of the body's normal processes for the metabolism of body fat. • In ketoacidosis, the accumulation of keto acids is so severe that the p. H of the blood is substantially decreased.

C. Treatment of Type I diabetes • Type 1 diabetics must rely on exogenous insulin injected subcutaneously to control the hyperglycemia and ketoacidosis. • Two therapeutic regimens are currently in use— standard and intensive insulin treatment.

1. Standard treatment versus intensive treatment: Standard treatment : typically consists of one or two daily injections of insulin. • Mean blood glucose levels obtained are typically in the 225— 275 mg/dl range, with a hemoglobin A 1 c(Hb. A 1 c) level of 8— 9% of the total hemoglobin

• In the normal 120 -day life span of the red blood cell, glucose molecules join hemoglobin, forming glycated hemoglobin. • In individuals with poorly controlled diabetes, increases in the quantities of these glycated hemoglobin are noted. • Once a hemoglobin molecule is glycated, it remains that way.

• A build up of glycated hemoglobin within the red cell reflects the average level of glucose to which the cell has been exposed during its life cycle. • Measuring glycated hemoglobin assesses the effectiveness of therapy by monitoring long-term serum glucose regulation. • The Hb. A 1 c level is proportional to average blood glucose concentration over the previous 4 weeks to 3 months.

• Thus, Hb. A 1 c provides a measure of how well treatment has normalized blood glucose in the diabetic over that time. intensive treatment: seeks to more closely normalize blood glucose through more frequent monitoring, and subsequent injections of insulin— 3 or more times a day. • Mean blood glucose levels of 150 mg/dl can be achieved, with Hb. A 1 capproximately 7% of the total hemoglobin

• Normal mean blood glucose is approximately 110 mg/dl and Hb. A 1 c is 6% or less • Thus, normalization of glucose values (euglycemia) is not achieved even in intensively treated patients. • patients on intensive therapy showed a 60% reduction in the long-term microvascular complications of diabetes— retinopathy, nephropathy, and neuropathy—compared with patients receiving standard care. • This confirms that the complications of diabetes are related to an elevation of plasma glucose.

2. Hypoglycemia in Type 1 diabetes: • therapeutic goals is to ↓ blood glucose levels in an effort to minimize the development of long-term complications of the disease • appropriate dosage is difficult to achieve.

• Hypoglycemia caused by excess insulin is the most common complication of insulin therapy, occurring in more 90% of patients. • The frequency of hypoglycemic episodes, coma, and seizures is particularly high with intensive treatment regimens designed to achieve tight control of blood glucose

• in normal individuals hypoglycemia triggers a compensatory secretion of counter-regulatory hormones, glucagon and epinephrine, which promote hepatic production of glucose. • patients with Type 1 diabetes also develop a deficiency of glucagon secretion. • This defect occurs early in the disease and is present four years after diagnosis. • These patients thus rely on epinephrine secretion to prevent severe hypoglycemia.

• As disease progresses, Type 1 diabetes patients show diabetic autonomic neuropathy and impaired ability to secrete epinephrine in response to hypoglycemia. • The combined deficiency of glucagon and epinephrine secretion creates a condition sometimes called “hypoglycemia unawareness? ’ Thus, patients with longstanding diabetes are particularly vulnerable to hypoglycemia.

• Exercise promotes glucose uptake into muscle and decreases the need for exogenous insulin. • Patients should check blood glucose levels before or after exercise

3 - Contraindications for tight control: • Children are not put on a program of tight control of blood glucose because of the risk that episodes of hypoglycemia may adversely affect brain development. • Elderly people typically do not go on tight control. • Hypoglycemia can cause strokes and heart attacks in older people. Also, the major goal of tight control is to prevent complications many years later.

TYPE 2 DIABETES • Type 2 diabetes is the most common form of the disease, afflicting approximately 90% of the diabetic population in the US • Type 2 diabetes develops gradually without obvious symptoms. • The disease is often detected by routine screening tests.

• many individuals with Type 2 diabetes have symptoms of polyuria and polydipsia of several weeks duration. • Polyphagia may be present, but is less common. • Patients with Type 2 diabetes have a combination of insulin resistance and dysfunctional cells • but do not require insulin to sustain life, although insulin may be required to control hyperglycemia in some patients.

• The metabolic alterations observed in Type 2 are milder than those for Type 1, because insulin secretion in Type 2 diabetes—although not adequate—does contain ketogenesis and blunts the development of DKA. • Diagnosis is based most commonly on the presence of hyperglycemia—that is, a blood glucose concentration of equal to or greater than 126 mg/dl. • Pathogenesis does not involve viruses or autoimmune antibodies.

A. Insulin resistance • Insulin resistance is the decreased ability of target tissues, such as liver, adipose, and muscle, to respond properly to normal circulating concentrations of insulin. • For example, insulin resistance is characterized by uncontrolled hepatic glucose production, and decreased glucose uptake by muscle and adipose tissue.

D. Treatment of Type 2 diabetes • The goal in treating Type 2 diabetes is to maintain blood glucose concentrations within normal limits, and to prevent the development of long-term complications. • Weight reduction • Exercise • dietary modifications often correct the hyperglycemia of Type 2 diabetes Hypoglycemic agents’ or insulin therapy may be required to achieve satisfactory plasma glucose levels.
- Slides: 38