DIABETES MELLITUS AND NONALCOHOLIC FATTY LIVER DISEASE DR

DIABETES MELLITUS AND NON-ALCOHOLIC FATTY LIVER DISEASE DR. GHOSON KANAYA

NONALCOHOLIC STEATOHEPATITIS


EPIDEMIOLOGY In the US, the prevalence of NAFLD has been increasing over time. This increase was demonstrated in a comparison of 3 cycles of the National Health and Nutrition Examination Survey(NHANES).

PREVALENCE NHANES DATA Time Period: Prevalence of NAFLD: 1988 -1994 5. 5% 1999 -2004 9. 8% 2005 -2008 11. 0% Accounting for 47, 63 and 75% of chronic liver disease during those time periods, respectively. However, it should be noted that the definition of NAFLD used in the study (elevated serum aminotransferase levels in the absence of an alternative explanation) could lead to misclassification and likely underestimated the true prevalence of NAFLD, since patients with NAFLD may have normal serum aminotransferases

PREVALENCE Over the same three time periods, the study also noted increases in the rates of other components of the metabolic syndrome, including obesity, Type 2 DM and systemic hypertension. Obesity DM 2 Systemic HTN 1988 -1994 22 6 23 1999 -2004 30 8 33 2005 -2008 33 9 34

TYPES OF NAFLD Secondary Primary 1 -Insulin resistance Obesity Diabetes Hypertriglyceridemia Hypertension 1 - sever weight loss jejunoileal bypass gastric bypass sever starvation 2 - total parenteral nutrition 3 - Iatrogenic Amiodarone Diltiazem tamoxifen Steroids 3 - Refeeding syndrome 4 - Toxic exposure Hydrocarbon , yellow 5 - Disorders of lipid metabolism A beta lipoproteinemia
 often have one")
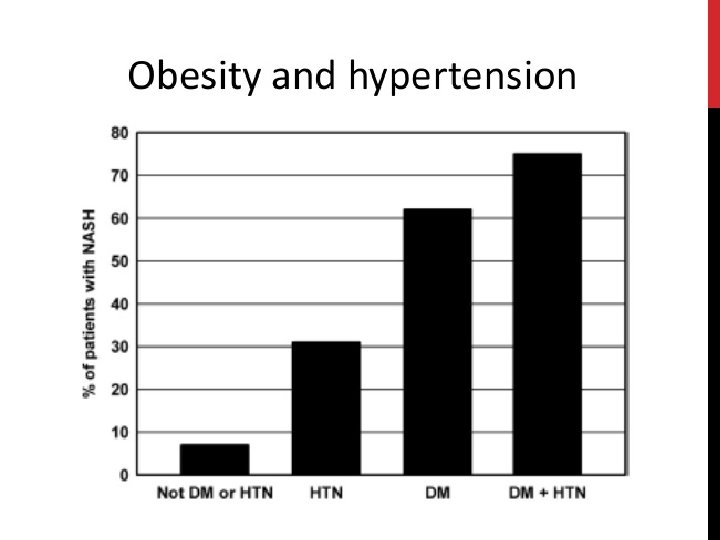
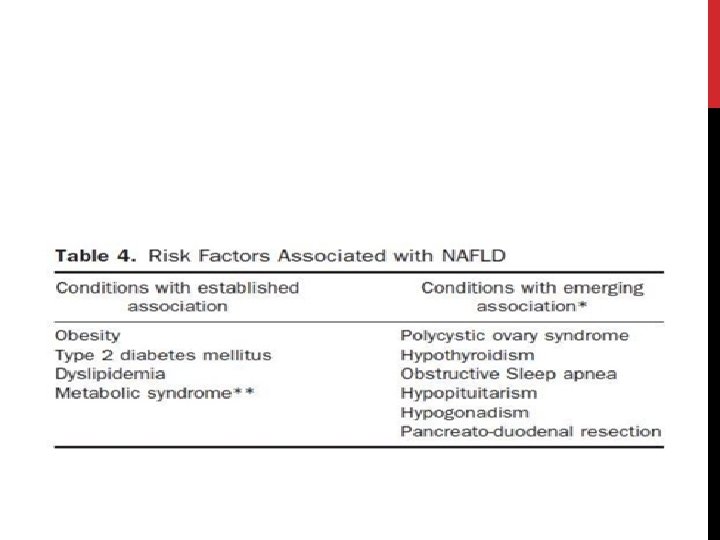
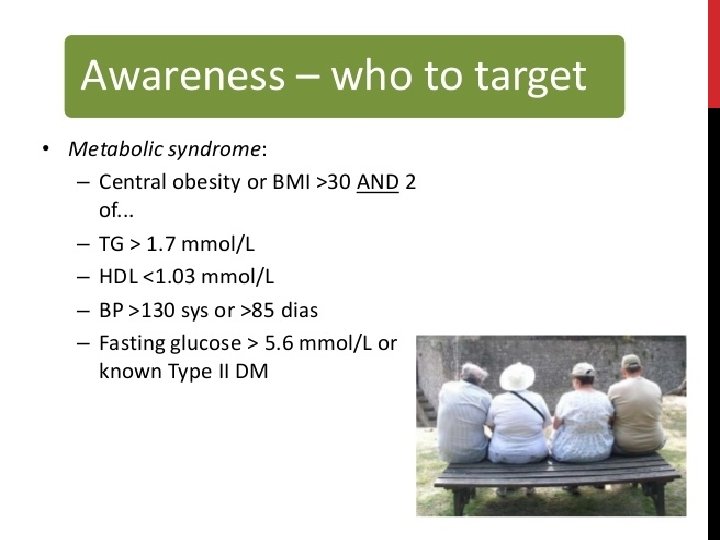
ASSOCIATION WITH OTHER DISORDERS Patients with NAFLD (particularly those with NASH) often have one or more components of the metabolic syndrome: Obesity Systemic hypertension Dyslipidemia Insulin resistance or overt diabetes

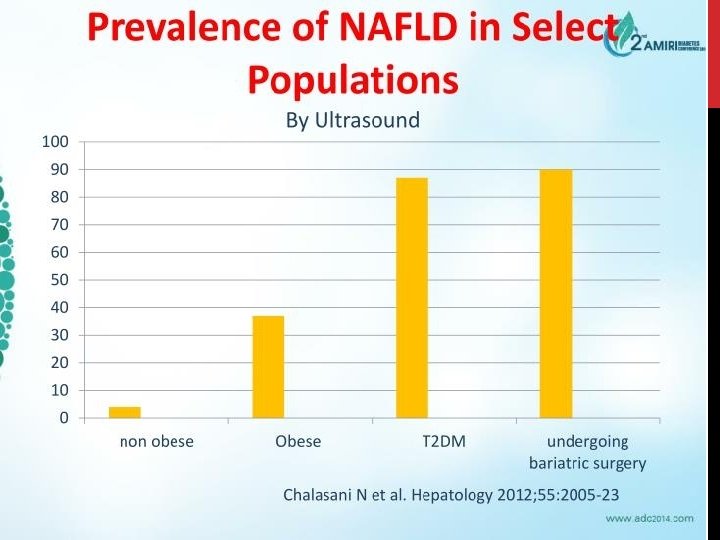
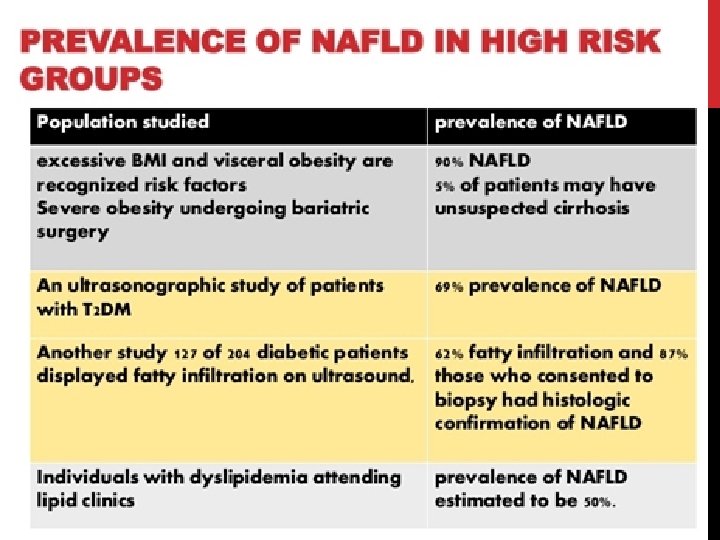
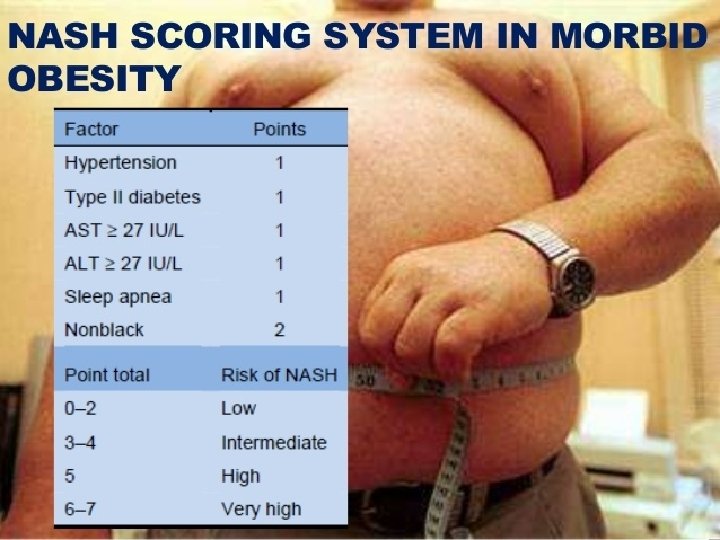
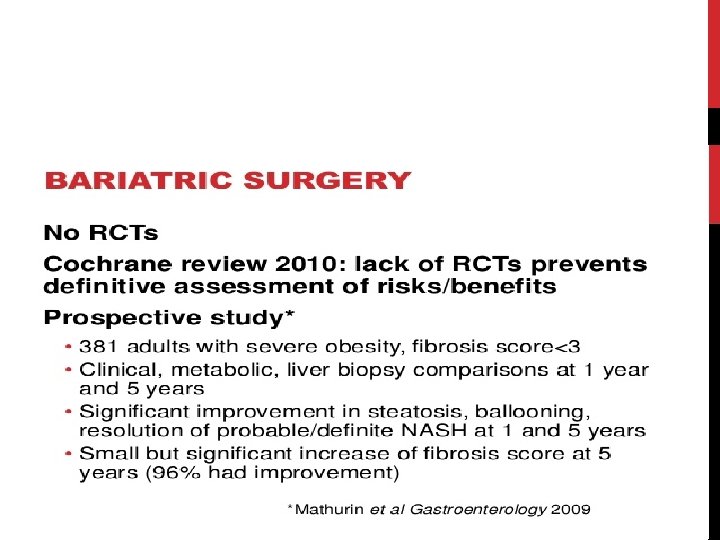
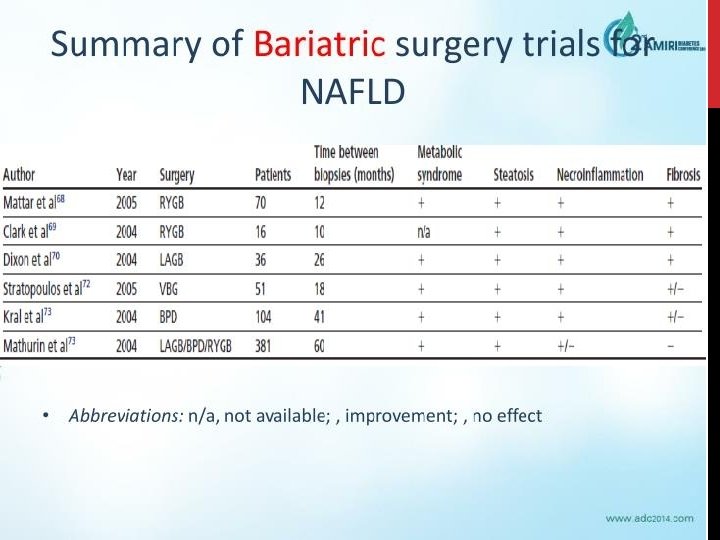
MORBID OBESITY Four studies evaluating > 600 morbidly obese patients undergoing gastric bypass - All patients underwent intraoperative liver biopsies -Prevalence of NAFL ranged from 30 -90% and NASH was documented in 33 -42%. -> 2/3 of morbidly obese patients undergoing gastric bypass surgery have NAFL/NASH

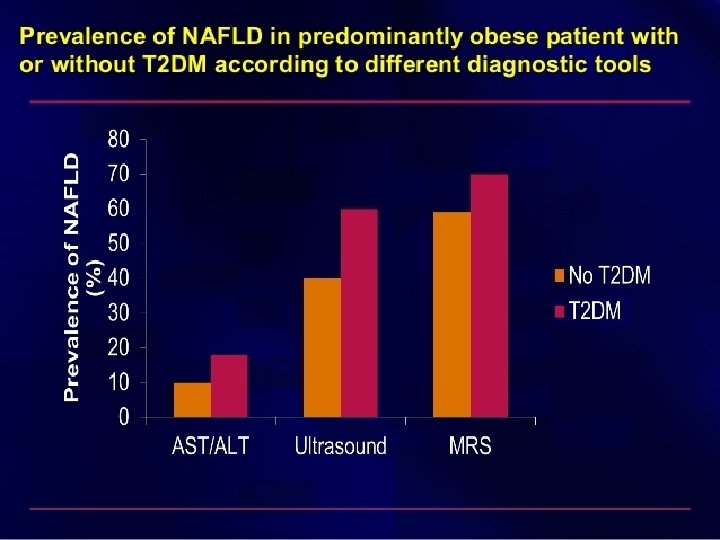
TYPE 2 DIABETES MELLITUS Recent study surveyed 100 patients with type 2 DM and used U/S to screen for NAFLD - Detected fatty liver in 50% of patients -Performed subsequent liver biopsy in those with NAFLD : . NAFL : 13%. NASH : 86%. Fibrosis : 22%

DYSLIPIDEMIA Canadian study used U/S to screen 95 adults with dyslipidemia - Detected fatty liver in 50% - Steatosis was particularly common in individuals with moderate to sever hypertriglyceridemia or mixed dyslipidemia - Hypertriglyceridemia and mixed dyslipidemia increased the risk for hepatic steatosis by ≈5 -fold
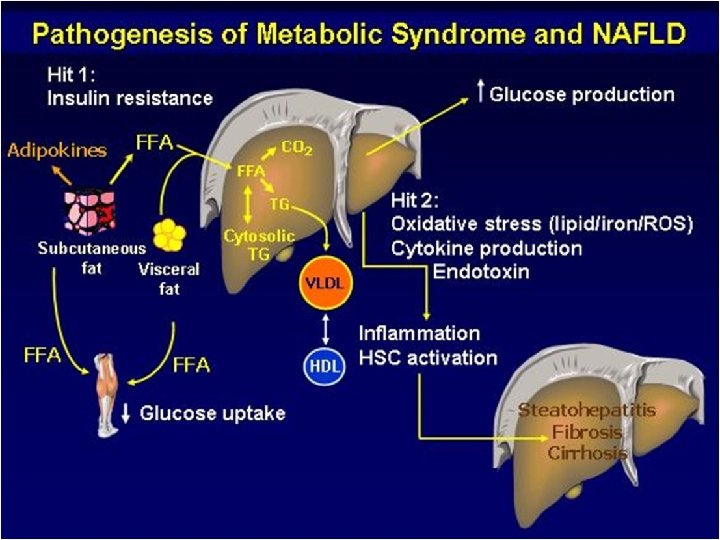

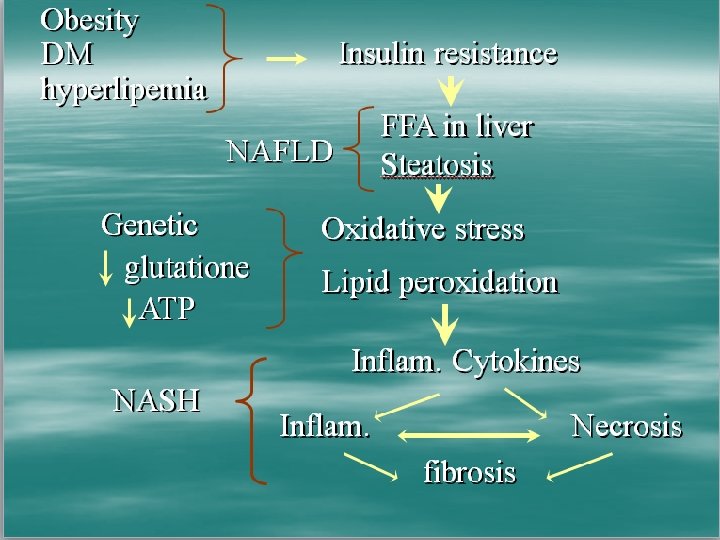
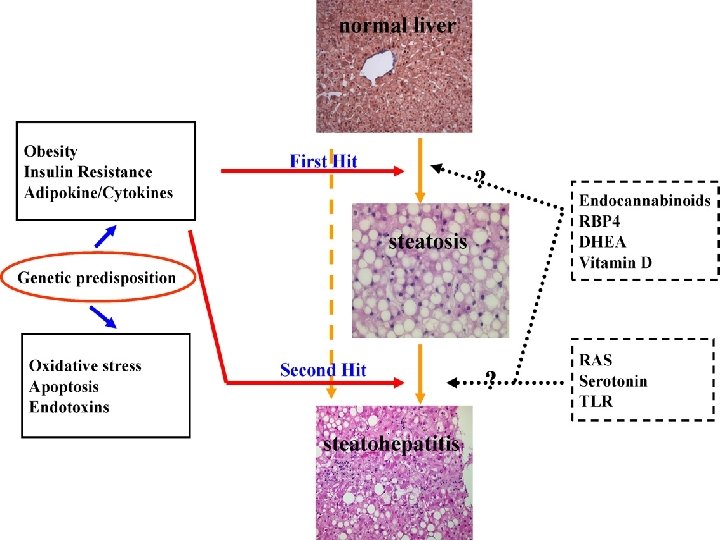
PATHOPHYSIOLOGY Other factors involved in NASH pathogenessis -Bacterial overgrowth. Increased hepatic oxidative stress. Production of ethanol and TNF-ᵅ. Direct activation of inflammatory cytokines and liver macrophages via release of lipopolysaccarides - Leptin -Obesity gene. Regulates food intake and body composition. Leads to hepatic steotosis by promoting insulin resistance or by modulating insulin signalling in hepatocytes

PATHOPHYSIOLOGY : OTHERS Serum and liver iron _ Mitochondrial ᵝ oxidation leads to generation of hydrogen peroxide _In presence of increased iron hydrogen peroxide converted to hydroxyl free radicles _ This leads to oxidative stress and hepatocellular injury

PATHOPHYSIOLOGY : OTHERS TNF – α _Corelates with obesity _Derives from adipose tissue _Decrease phosphorylation of insulin receptor _ Reduce expression of GLUT-4 _Contributes toward insulin resistence _ Also causes chemotaxis, activation of stellate cells, Mallory hyaline formation , collagen synthesis
 2) Obesity – Pt undergoing Bariatric surgery")
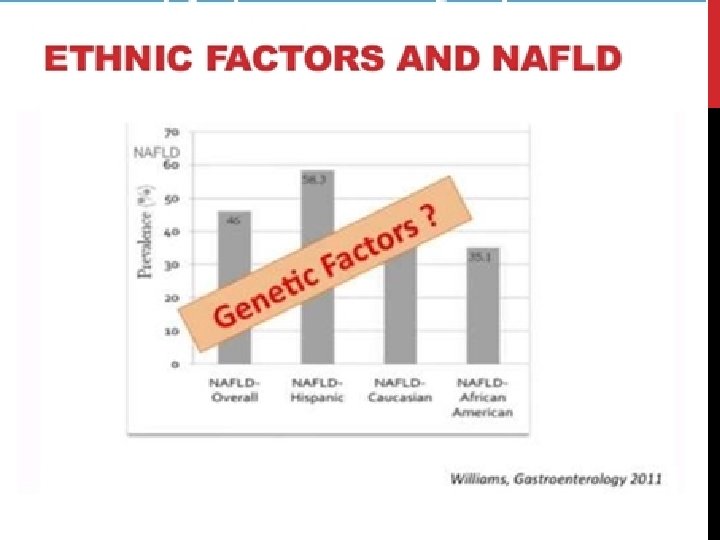
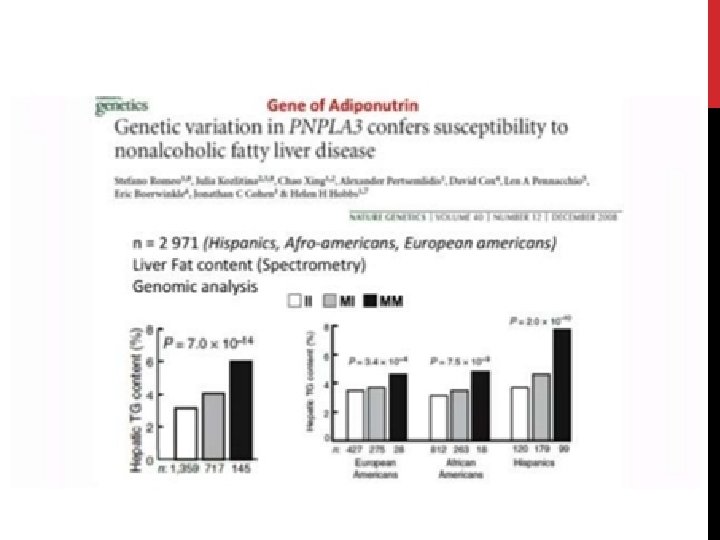
PREDISPOSING FACTORS FOR PROGRESSION OF NAFLD 1) 2) Obesity – Pt undergoing Bariatric surgery (90% steatosis, 30% NASH, 10% advanced fibrosis / cirrhosis) Metabolic conditions – Type 2 DM – 66% will have US evidence of NAFLD – Polycystic ovarian syndrome – 50% 3) Age (may reflect longer standing undiagnosed NAFLD) 4) Gender M>F (? protective effect of oestrogen) 5) Ethnicity – Hispanics > Other white > African Americans 6) Genetics – PNPLA 3 gene (Others include NCAN, GCKR, LYPLAL 1)

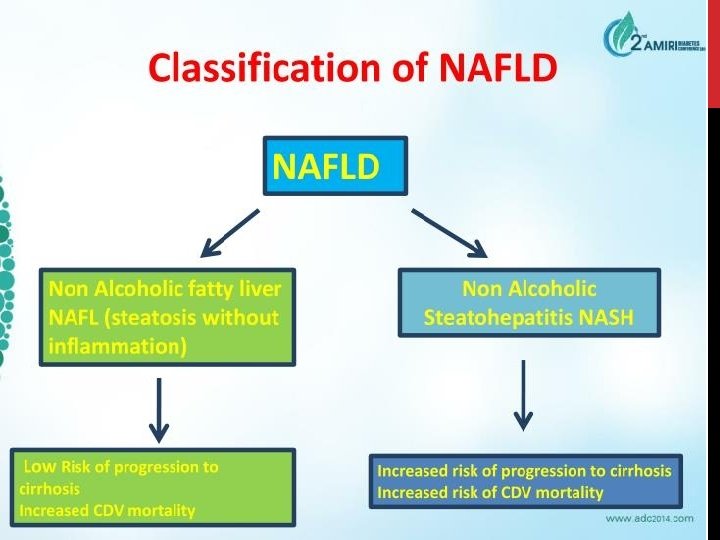
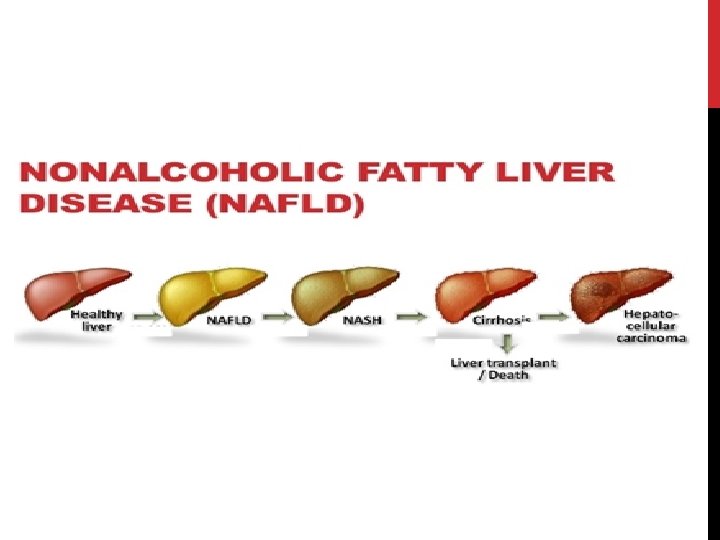
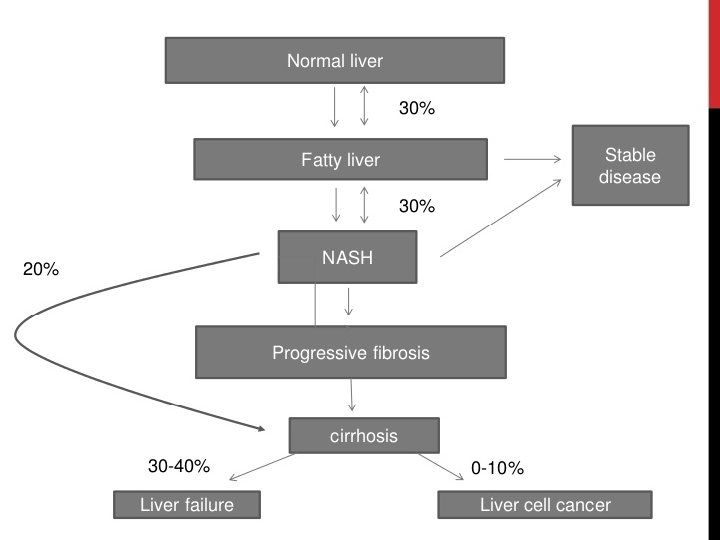
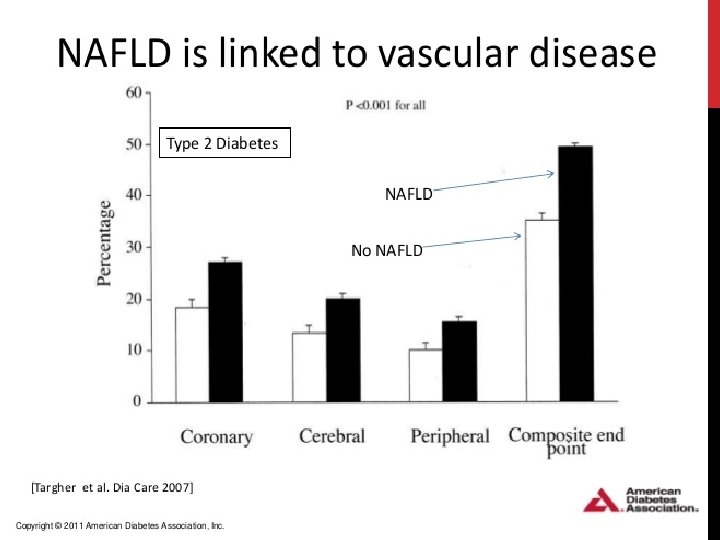
NAFLD - PROGNOSIS • Increased overall mortality compared to matched control populations. • Commonest cause of death in patients with NAFLD, NAFL and NASH is cardiovascular disease. • Increased liver-related mortality rate – increasingly common indication for liver transplantation (15 -20%).
 have a benign liver-related prognosis _1, 5% develop")
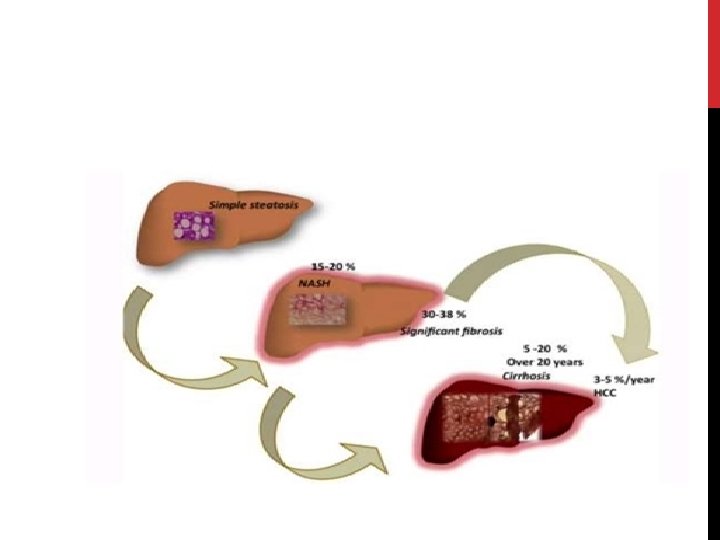
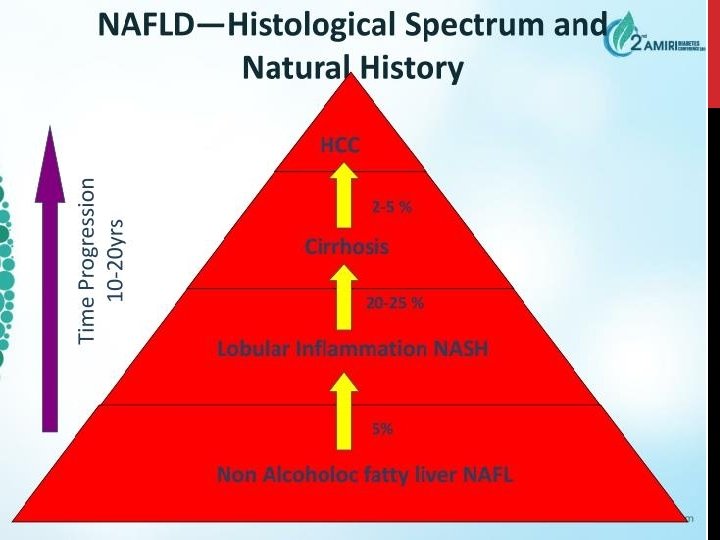
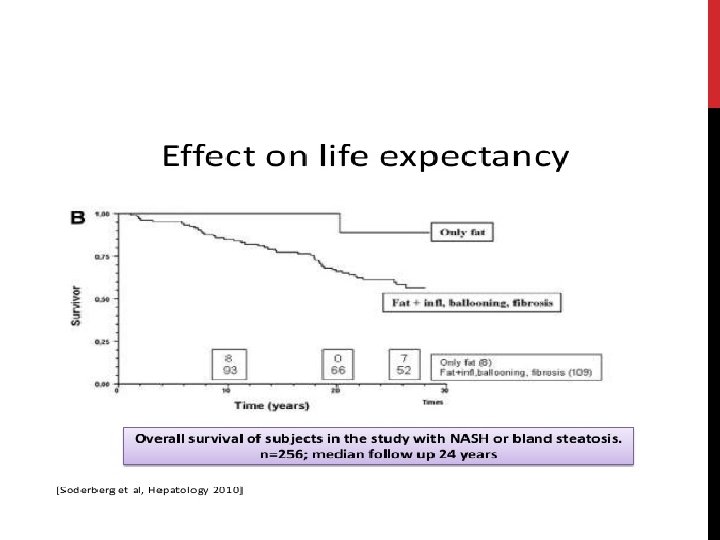
PROGNOSIS Patients with bland steatosis (NAFL) have a benign liver-related prognosis _1, 5% develop cirrhosis _1% die from liver-related causes over 10 -20 years • Almost 30% of patients with NASH and fibrosis become cirrhotic within 5 -10 years _ those with biopsy-proven NASH have a liver-related death rate of ~10% • NASH cirrhosis may develop into HCC - ~13% of cases of all HCC are related to NASH cirrhosis -Endstage NAFLD accounts for ~5 -10% of liver transplants

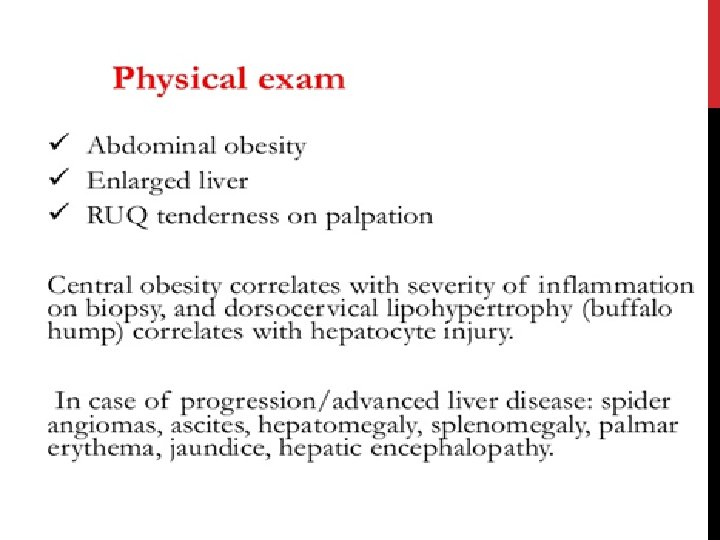
CLINICAL PRESENTATION ü ü Variable clinical presentation Typically asymptomatic , but may have hepatomegaly and abdominal discomfort ü Liver enzymes may be normal in >75% of cases , making them insensitive in detecting NAFLD _When increased , usually only modestly and limited to aminotransferases _ ALT upper limit of normal : <30 in M, <20 in f

WHO TO REFER? Calculate NAFLD fibrosis score or fatty liver index! (Age, BMI, hyperglycaemia, plts, albumin, AST/ALT ratio). – AUROC 0. 85 for advanced fibrosis. (There’s an app!!)
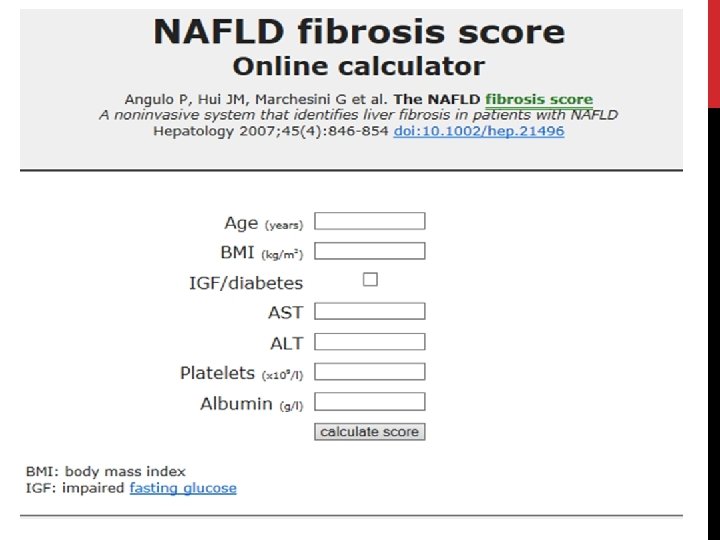

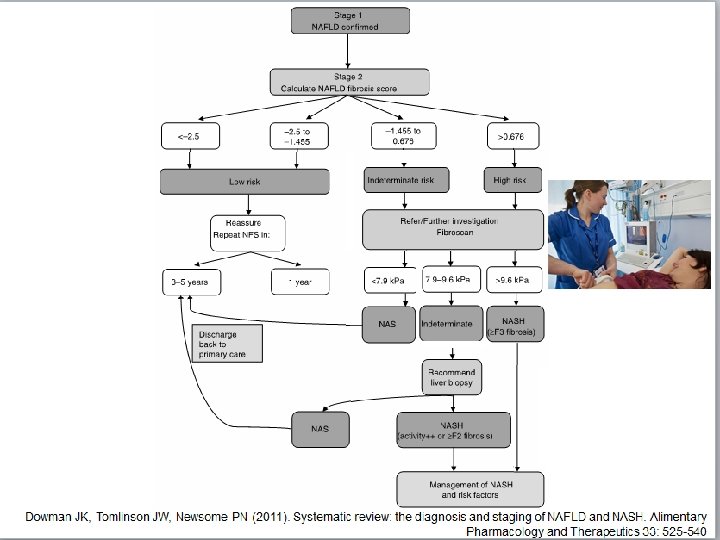
NAFLD FIBROSIS SCORE < -1. 455: predictor of absence of significant fibrosis (F 0 -F 2 fibrosis) ≤ -1. 455 to ≤ 0. 675: indeterminate score > 0. 675: predictor of presence of significant fibrosis (F 3 -F 4 fibrosis)

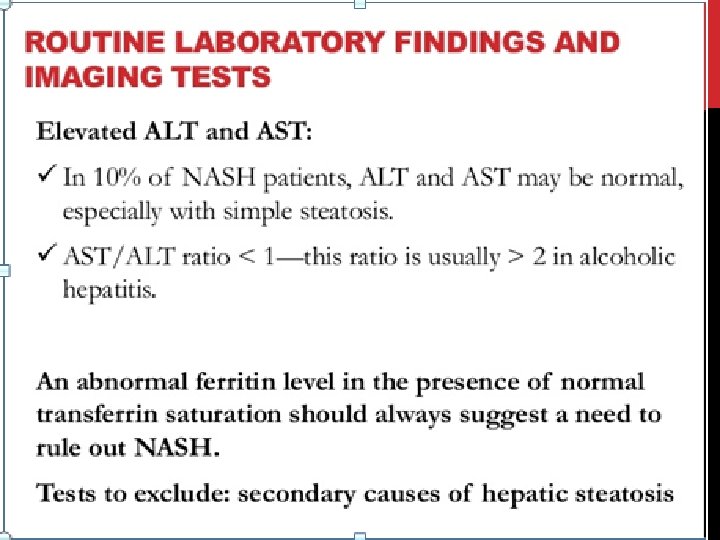
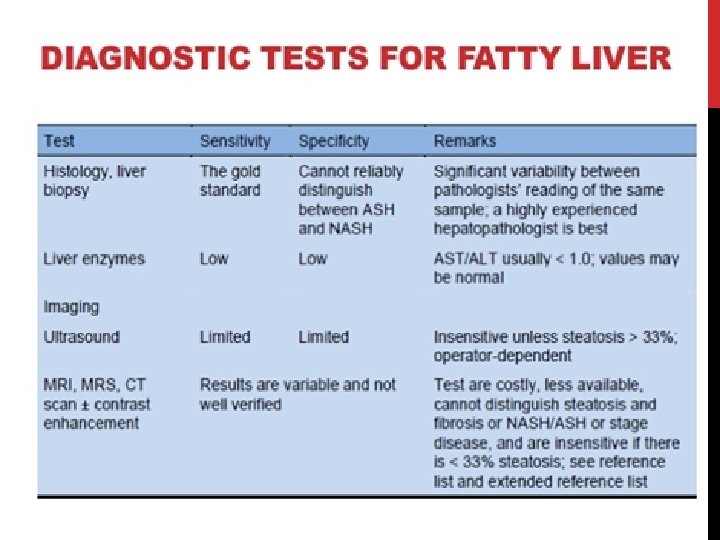
LAB STUDIES No laboratory studies can help definitively establish a diagnosis of fatty liver or NASH Aminotransferases _Elevated AST or ALT _ As much as 10 -fold _ In the absence of cirrhosis , an AST-to- ALT ratio of greater than 2 suggests alcohol use , whereas a ratio of less than 1 may occur in patients with NASH. Alkaline phosphatase _ Can be elevated _Usually less than 2 to 3 times normal
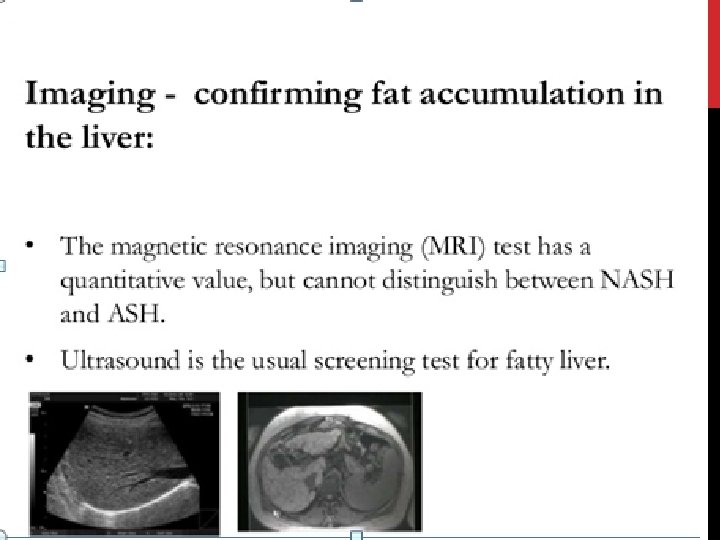
 No imaging studies can differentiate Between the histological subtypes of Benign")
DIAGNOSIS (CONT. ) No imaging studies can differentiate Between the histological subtypes of Benign steatosis or aggressive NASH, or Stage the degree of fibrosis

LIVER BIOPSY A liver biopsy and histopathological Examination are required to establish the diagnosis The diagnosis should be considered in all Patients with unexplained elevations in serum Aminotransferases (eg, with findings negative For viral markers or autoantibodies or with no History of alcohol use).

DOING LIVER BIOPSY IS CONTROVERSIAL Arguments favoring. Exclusion of other cause. To distinguish steatosis from NASH. Determination of prognosis v. Argument against biopsy. Good prognosis. Lack of effective therapy. Risk &cost associated with biopsy
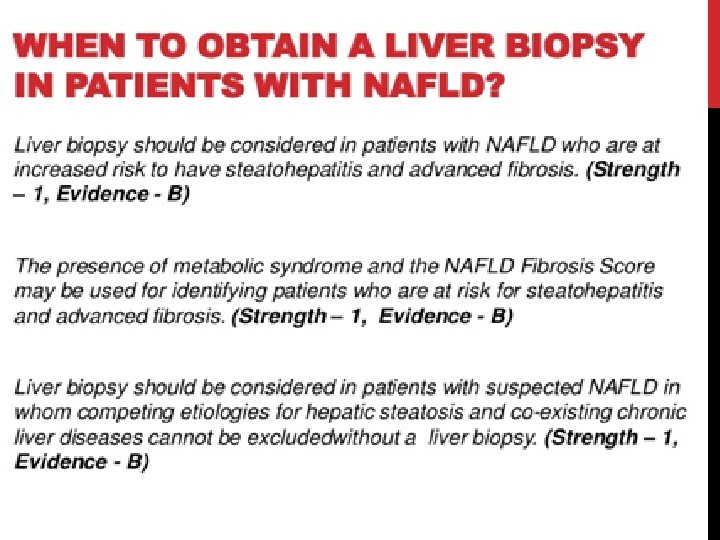

NAFLD DIAGNOSIS Diagnosis of NAFLD requires all of the following: Demonstration of hepatic steatosis by imaging or biopsy Exclusion of significant alcohol consumption Exclusion of other causes of hepatic steatosis
 Characteristic liver biopsy that shows fatty change with inflammation _indistinguishable")
NASH CRITERIA (AGA GUIDELINES) Characteristic liver biopsy that shows fatty change with inflammation _indistinguishable from alcoholic hepatitis • Convincing evidence of negligible alcohol consumption (less than 20 g alcohol per day ) _Detailed history obtained independently by 3 physicians , interrogation of family members • Absence of serologic evidence of Hep. B or Hep C infection _Should not exclude those with evidence of past hep B , HBs. Ag or HCV Ab
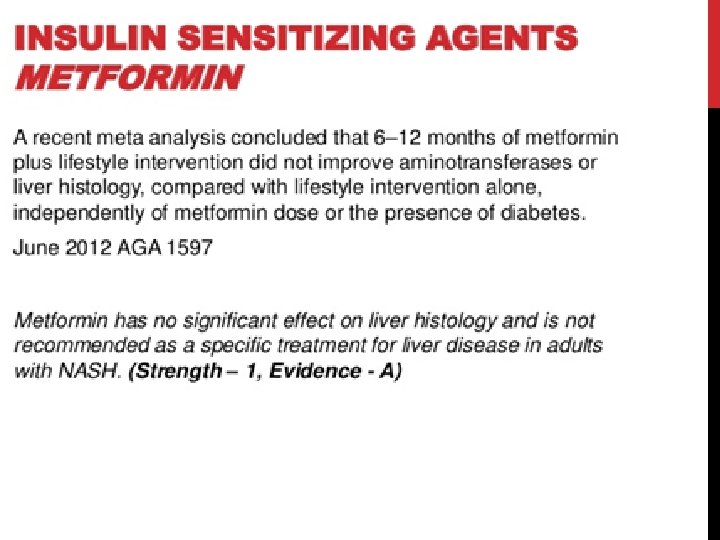
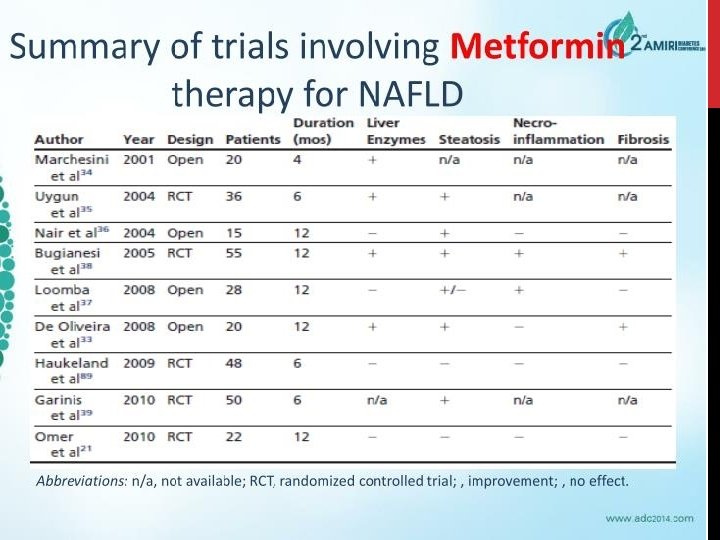
 Metformin • 2) Lipid-lowering agents (statins) – commonest cause")
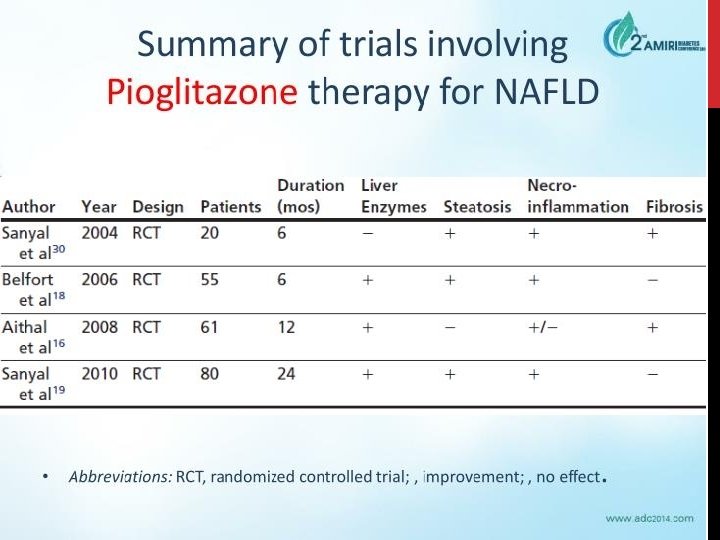
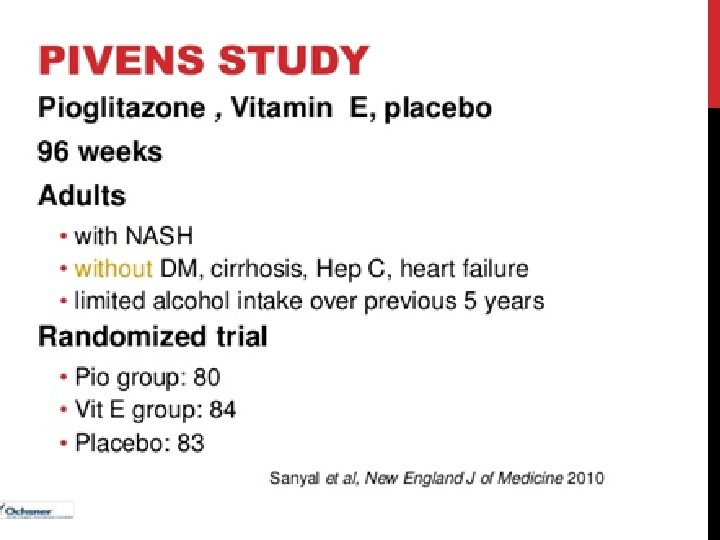
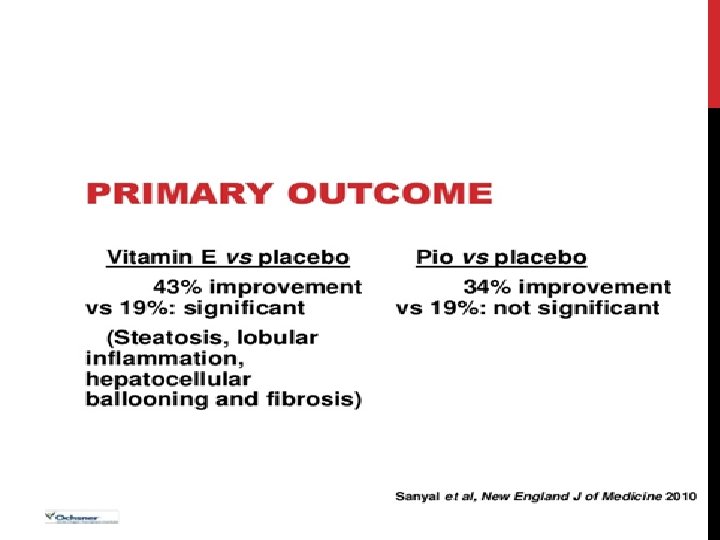
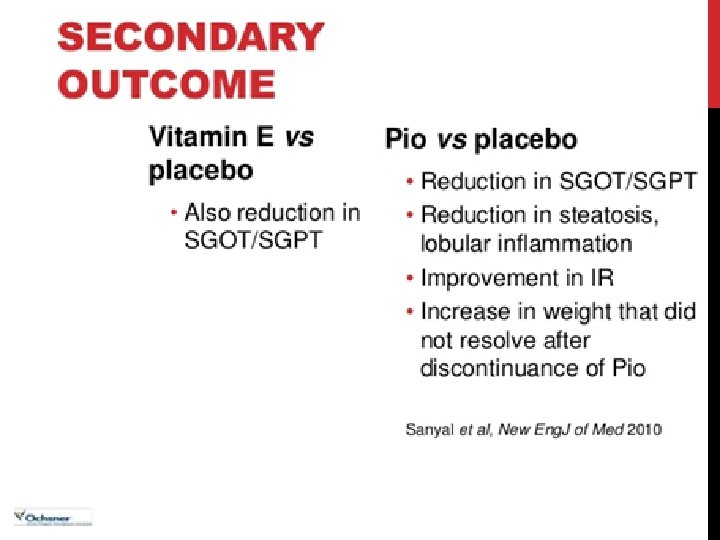
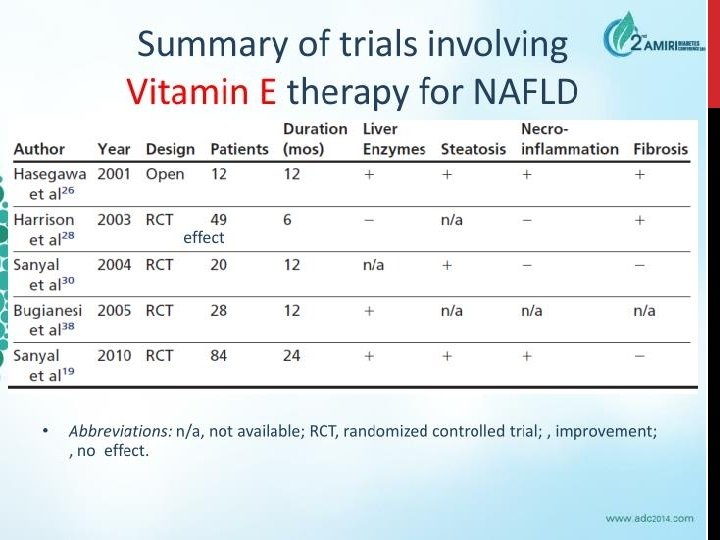
MEDICATION FOR NAFLD • 1) Metformin • 2) Lipid-lowering agents (statins) – commonest cause of death is cardiovascular. – Reduced rate of HCC and improvement in LFTs – Statins are safe in liver disease!! (RCTs) • 3) Vitamin E • PIVENS trial 2010 – Improvement in NASH: 43% vs 19%, p=0. 001 • Considered 1 st line for pharmacotherapy of NASH (not in diabetic patients!) • 4) Thiazolidinediones (pioglitazone) – Improvement in liver histology whilst on drug but may relapse on stopping. Causes weight gain • 5) ? role for Glucagon-like peptide 1 (GLP-1), DPP-4 inhibitors.

- Slides: 94