Diabetes Its Relevance to Retinopathy Screening Dr John

Diabetes & Its Relevance to Retinopathy Screening Dr John Doig Consultant Diabetologist DRS Clinical Lead Forth Valley

Diabetes & Its Relevance to Retinopathy Screening • • • What is diabetes Diagnosis Types of Diabetes Treatment Complications – Acute metabolic – Macrovascular – Microvascular • Managing Risk Factors

What is Diabetes Mellitus • Diabetes = excessive production of urine • mellitus = honeyed • Life-long illness associated with various complications – Blindness – Heart disease – Kidney disease – Damage to the feeling in the limbs (peripheral neuropathy).

Diabetes Mellitus • characterised by high blood sugar levels, disturbances of carbohydrate, fat and protein metabolism • absolute lack or a relative deficiency in insulin action and/or insulin secretion • Prevalence increasing – Scottish Survey 2001 – Forth Valley 2006 – Some practices = 2. 1 % = 4. 1 % = 5. 0 %

Management of Diabetic Patient • Main Issues – Diagnosis – Glycaemic Control – Screening • Microvascular Complications • Macrovascular Complications – Diabetes related issues / Education • Driving, Work, Pregnancy • Injection sites, Diet, Monitoring

Diagnosis • Symptoms – Osmotic Symptoms & Fatigue – Weight loss / gain – Infection – Neuropathic Symptoms – Visual Upset – Cardiovascular symptoms
 Random Plasma Glucose")
Diagnosis: Diagnostic Criteria Fasting Plasma Glucose >7. 0 (on 2 occasions*) Random Plasma Glucose >11. 1 (on 2 occasions*) (1 occasion if symptomatic) Fasting Plasma Glucose 2 hr post 75 g glucose 6. 1 - 6. 9 = IFG 7. 8 - 11. 1 = IGT > 11. 1 = DM

Type of Diabetes • Type I – Young < 35 – Thin + weight loss – Rapid onset – Ketonuria – Autoimmune – B Cell failure – Insulin Dependent • Type 2 – Older > 35 – Overweight – Onset months – Strong FH – Complications – – – Insulin resistance Late B Cell failure Hyperinsulinaemia Metabolic syndrome Cardiovascular Disease

Other types of Diabetes • Gestational • Drug induced – Steroids, Atypical Neuroleptics • Metabolic – Haemachromatosis, Cushings, Acromegaly • Pancreatic disease • MODY (Genetic) • Stress hyperglycaemia

Treatment • Diet • Oral Hypoglycaemic Agents – Sulphonylureas – Biguanides – Alpha 1 glucosidase inhibitors – Thiazolidinediones(Glitazones or Insulin sensitisers) – Exenatide GLP-1 agonists – DPP 4 Inhibitors Gliptins • Insulin – Soluble, Biphasic, Intermediate / Long acting

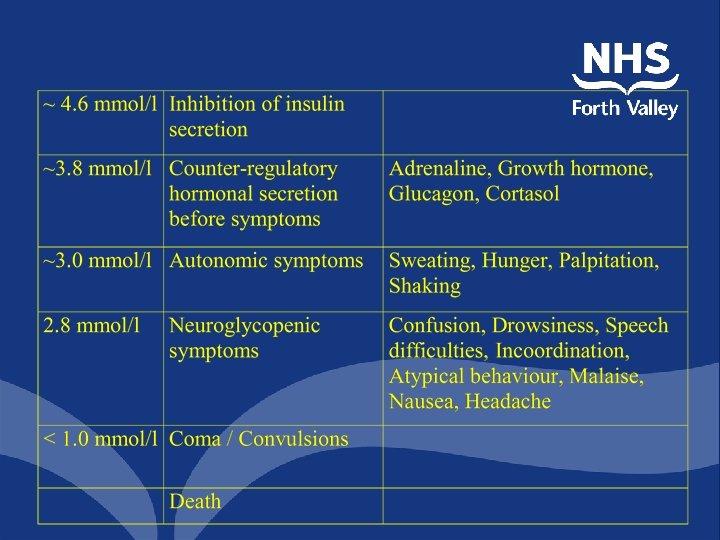
Acute Metabolic Complications • Diabetic Ketoacidosis • Hyper Osmolor Nonketotic Coma • Lactic Acidosis • Hypoglycaemia

Hypoglycaemia • • Common side effect of Insulin or Sulphonylureas Does not occur with Metformin, Acarbose or TZD’s Minor hypos often go unreported (Self treated) Severe hypos occurs in 25 -30 % of patients each year • Coma occurs in ~ 10 % of patients each year

Causes of hypoglycaemia Management Errors Inadequate Carbohydrate Altered Kinetics Increased Sensitivity Factitious Lipohypertrophy, Site massage, Heat, Cold, Antibodies, Renal, Exercise, Human insulin Addison’s disease, Hypothyroidism, Hypopituitarism, Changes in gonadal steroids, Pregnancy

Risk factors for severe hypoglycaemia • Insulin treatment regimen Intensified High insulin doses • Impaired awareness of hypoglycaemia Acute Chronic (Preceding hypoglycaemic episodes) (Central autonomic failure) • Long duration of diabetes • Increasing age of patient • Sleep, Excessive alcohol consumption

Morbidity of hypoglycaemia • CNS Coma and Convulsions Transient motor deficits Permanent brain damage Cerebral Oedema • CVS Arrhythmia Myocardial ischaemia Stroke • Fractures, Vitreous haemorrhage

Treatment of hypoglycaemia • Treated immediately by oral glucose 10 -20 g • If unable to swallow then – Intravenous glucose 50 ml 20% – Intravenous glucose 25 ml 50 % – Subcutaneous glucagon 1 mg • Patients usually recover within minutes • Failure to do so may be due to cerebral oedema • On recovery encourage consumption of complex carbohydrate • Identify cause & take appropriate action / patient to contact diabetes care team.

Macrovascular Complications • Coronary Artery Disease • Peryipheral Vascular Disease • Cerebro Vascular Disease – Hyperlipidaemia – Hypertension – Obesity

Cumulative Hazard for Any CVD Endpoint CARDS Relative Risk = -32% (95% CI -45, -15) p=0. 001 Cumulative Hazard (%) 20 Placebo 189 events 15 Atorvastatin 134 events 10 5 0 0 Placebo 1410 Atorva 1428 1 2 3 4 4. 75 1334 1372 1275 1337 992 1040 621 663 287 306 Years

All Cause Mortality Hazard ratio 5 p<0. 0001 1 0. 5 12% decrease per 10 mm Hg decrement in BP 110 120 130 140 150 160 170 Updated mean systolic blood pressure UKPDS 36. BMJ 2000; 321: 412 -19

HOT: Events in relation to target blood pressure. Diabetic patients

All Cause Mortality Hazard ratio 5 p<0. 0001 1 14% decrease per 1% decrement in Hb. A 1 c 0. 5 0 5 6 7 8 9 Updated mean Hb. A 1 c UKPDS 35. BMJ 2000; 321: 405 -12 10 11
 –")
Cardiovascular Disease Prevention • Improved cardiovascular risk with: – Improved glycaemic control (Metformin) – Improved BP control (Target < 140/80) – Addition of long acting ACEI if high risk – Lipid reduction – All secondary preventative measures • Aspirin, B Blocker

Microvascular Complications • Diabetic Retinopathy • Diabetic Nephropathy – Microalbuminuria – Macroalbuminuria – Renal impairment • Diabetic Neuropathy – Sensory - Ulceration, Neuroarthropathy – Motor – Foot deformity – Autonomic – GI upset, Hypotension, ED

Diabetic Eye Disease • Diabetic eye complications major cause of visual loss. • Most important preventable cause of blindness in Europe. • Accounts for about 90 % of blindness in diabetic patients. • St. Vincent Declaration 5 year targets 1989 – Incidence of blindness due to diabetes should be reduced by one third or more. • Duration of diabetes is the most important predictor.

Prevalence of Retinopathy • • In young persons with duration less than 5 yrs In patients > 30 yrs with duration 5 yrs Duration 10 yrs Duration 20 yrs rare 20 % 40 -50 % 90 % • Approx 30% of diabetic population have DR • Prevalence of visual impairment in UK ? 2 -5 %?

Diabetic Retinopathy • Approx 10 -15 % of patients progress to sight threatening retinopathy – Pre proliferative retinopathy – Proliferative retinopathy – Vitreous haemorrhage – Maculopathy • Other sight threatening disease more common in diabetes – Cataract – Macular Degeneration – Glaucoma

Risk Factors for Diabetic Retinopathy • • duration of diabetes poor glycaemic control raised blood pressure increasing number of microaneurysms microalbuminuria and proteinuria (nephropathy) raised triglycerides and lowered haematocrit pregnancy

Modifiable Risk Factors for Prevention of DR • Glycaemic Control – 1. 7 % reduction in Hb. A 1 c (8. 9% vs 7. 2%) – 76 % risk reduction for developing DR – 43 % risk reduction for retinopathy progression • Blood Pressure Control • Smoking

Evidence For Good Control • 1993 DCCTHb. A 1 c 8. 9 vs. 7. 2 % – Reduced risk of developing: • Retinopathy 76 % • Microalbuminuria 39 % • Clinical neuropathy 60 % • 1998 UKPDS Hb. A 1 c 7. 9 vs. 7. 0 % – Reduced risk of: • Retinopathy 21% • Microalbuminuria 33% • Myocardial Infarction 16 %

UKPDS Blood Pressure Control Study in 1148 Type 2 diabetic patients a tight blood pressure control policy which achieved blood pressure of 144 / 82 mm. Hg (vs 154/87) gave reduced risk for any diabetes-related endpoint 24% p=0. 0046 diabetes-related deaths 32% p=0. 019 stroke 44% p=0. 013 heart failure 56% p=0. 0043 microvascular disease 37% p=0. 0092 retinopathy progression 34% deterioration of vision 47% p=0. 0038 p=0. 0036

Microvascular Endpoints 15 Hazard ratio 10 p<0. 0001 1 37% decrease per 1% decrement in Hb. A 1 c 0. 5 0 5 6 7 8 9 Updated mean Hb. A 1 c UKPDS 35. BMJ 2000; 321: 405 -12 10 11

Sight Threatening Retinopathy • No visual symptoms when most amenable to treatment • If visual symptoms present then prognosis poorer • Potocoagulation will abolish new vessels in 80 % and prevent blindness in >50% after 10 years • Photocoagulation will salvage vision in 50 -60 % • Vitrectomy may be effective in restoring meaningful vision > 6/36

Detection of Diabetic Retinopathy • Retinopathy is detected in its earliest and most treatable form only by clinical examination of eyes. • Ideally suited to screening programs • Screening must be comprehensive, of high sensitivity (>80%) and specificity (>95%). Should include measurement of visual acuity. Clear line of referral. • Various options:

Performance of screening • • • General Practitioners Hospital Physician Non Mydriatic Camera Diabetologist Ophthalmology registrar • 2 Field retinal photographs • Combined 5 field + direct Sensitivity 41 67 67 70 75 Specificity 89 96 98 97 97 89 97 86 95

Patients with retinopathy • Aim for – Good glycaemic control Hb. A 1 c < 7. 0% – Good BP control <130/70 – Lipid control / Statin Cholesterol <4. 0 – Stop smoking – Correct anaemia
- Slides: 36