Diabetes Fundamentals Series Beverly Dyck Thomassian RN MPH

Diabetes Fundamentals Series Beverly Dyck Thomassian, RN, MPH, BC-ADM, CDE President, Diabetes Education Services www. Diabetes. Ed. net 2019

Welcome to Diabetes Fundamentals � Series of 6 courses designed to provide you with the building blocks of diabetes care � Within 24 hours of the live broadcast, we will have the recorded version posted on our Diabetes Education University (DEU). � Updated Power. Point handouts will have 2019 in the Description � Earn CE certificate by taking post test and survey on our DEU Site. � Please contact Anne with any questions! Anne@diabetesed. net

Course Objectives Discuss factors contributing to increased prevalence of diabetes 2. Describe pathophysiological defects associated with the development of diabetes mellitus. 3. Differentiate the different types: prediabetes, Type 1, Type 2 and GDM 4. Discuss new language guidelines 5. Describe the impact of insulin resistance 1.

Foundations of Care �Education �Nutrition �Monitoring �Physical Activity �Psychosocial Care �Medications �Reducing Risk �Getting to Best Possible Health

Improving Care & Promoting Health �Start with patient centered communication. � Incorporate pt preferences, literacy, life experiences �Treatment decisions timely, based on evidence and tailored to individual pt. �Align care with Chronic Care Model to ensure proactive practice and informed, activated patient. �Assess social context, including food insecurity, housing stability, financial barriers and apply to treatment decisions.

CDC Announces 35% of Americans will have Diabetes by 2050 Boyle, Thompson, Barker, Williamson 2010, Oct 22: 8(1)29 www. pophealthmetrics. com

Diabetes in America 2019 � 30. 3 million or > 9. 4% � 24% don’t know they have it � 34 % of US adults have pre diabetes (84 mil)

Age-adjusted Diabetes Prevalence 20 yrs or older, by race/ethnicity— U. S. 2013 -2015

Obesity and Economics in America } 68% overweight or obese } 34% BMI 30 +, 34% BMI 25 -29 } 1/3 of all overwt people don’t get diabetes } We burn 100 cals less a day at work } Overall, food costs ~ 10 -15% of income } Calorie Intake is on the rise

Now, let’s get to the Nitty Gritty

Poll Question 1 �In the fasting state, hyperglycemia is directly related to: a. Increased hepatic glucose production b. Defective insulin stimulation of target tissue glucose disposal c. Decreased adipocyte lipolysis d. Loss of pancreatic alpha-cell function
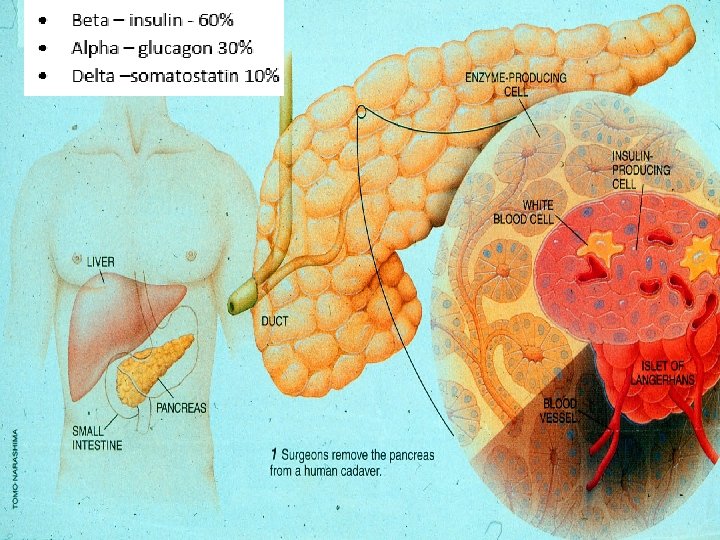
 �Stress hormones (kidney) �Epinephrine (kidney) �Insulin (pancreas)")
Hormones Effect on Glucose Hormone �Glucagon (pancreas) �Stress hormones (kidney) �Epinephrine (kidney) �Insulin (pancreas) �Amylin (pancreas) �Gut hormones - incretins (GLP-1) released by L cells of intestinal mucosa, beta cell has receptors) Effect

Signs of Diabetes �Polyuria �Polydipsia �Polyphasia �Weight loss �Fatigue �Skin and other infections �Blurry vision Glycosuria, H 2 O losses Dehydration Fuel Depletion Loss of body tissue, H 2 O Poor energy utilization Hyperglycemia increases incidence of infection Osmotic changes

Poll Question 2 �Pre-diabetes is defined as a glucose of: a. b. c. d. Fasting BG of 100 -125 mg/dl Any BG above 99 mg/dl Fasting BG 126 -200 mg/dl Fasting BG of 140 mg/dl or more

Natural History of Diabetes Yes! Normal FBG <100 Random <140 A 1 c <5. 7% Prediabetes FBG 100 -125 Random 140 - 199 A 1 c ~ 5. 7 - 6. 4% 50% working pancreas NO Diabetes FBG 126 + Random 200 + A 1 c 6. 5% or + 20% working pancreas Development of type 2 diabetes happens over years or decades

Poll Question 3 �Diabetes is defined as a random glucose of a. 126 -199 mg/dl b. 200 mg/dl or greater c. 140 -199 mg/dl d. 140 mg/dl or greater

Diagnostic Criteria �All test should be repeated in the absence of unequivocal hyperglycemia �If test abnormal, repeat same test to confirm diagnosis on a different day �If one test normal, the other abnormal, repeat the abnormal test to determine status �Medicare still using fasting as criteria for reimbursement for education

A 1 c Test – To diagnose & eval �Measures glycation of RBC’s over 2 -3 months �Weighted mean (50% preceding month) �Each 1% ~ 29 mg/dl �Accuracy: affected by some anemias, hemoglobinopathies �A measurement of glucose in fasting and postprandial states �African Americans may have false lows


Poll Question 4 �Each percentage of A 1 c = how many mg/dl of blood glucose? a. 33 b. 27 c. 17 d. 29
 A 1 c (%) 5")
A 1 c and Estimated Avg Glucose (e. AG) A 1 c (%) 5 6 7 8 9 10 11 12 e. AG 97 126 154 183 212 240 269 298 e. AG = 28. 7 x A 1 c-46. 7 ~ 29 pts per 1% Order teaching tool kit free at diabetes. org Translating the A 1 c Assay Into Estimated Average Glucose Values – ADAG Study Diabetes Care: 31, #8, August 2008

What Kind of Diabetes? �AJ, a 12 year old female admitted to the ICU with a blood glucose of 476 mg/dl and a p. H of 7. 1. � What further questions and or testing is needed to determine if patient has type 1 or type 2 diabetes?

Type 1 Diabetes

What Does Type 1 Look Like? Mary Tyler Moore Nick Jonas Justice Sonia Sotomayor Bret Michaels

Type 1 Rates Increasing Globally � 23% rise in type 1 diabetes incidence from 2001 -2009 �Why? � Autoimmune disease rates increasing over all � Changes in environmental exposure and gut bacteria? � Hygiene hypothesis � Obesity?

Incidence of Type 1 in Youth �General Pop 0. 3% �Sibling 4% �Mother 2 -3% �Father 6 -8% �Rate doubling every 20 yrs �Many trials underway to detect and prevent (Trial Net)

Type 1 – 10% of all Diabetes Genetics and Risk Factors Ø Auto-immune pancreatic beta cells destruction Ø Most commonly expressed at age 10 -14 Ø Insulin sensitive (require 0. 5 - 1. 0 units/kg/day) Combo of genes and environment: Autoimmunity tends to run in families Higher rates in non breastfed infants Viral triggers: congenital rubella, coxsackie virus B, cytomegalovirus, adenovirus and mumps.

How do we know someone has Type 1 vs Type 2? �Type 1 � Positive antibodies � GAD � ICA � IAA and others �Younger people develop quickly �Older people take longer to develop �Body wt and presentation

Autoantibodies Assoc w/ Type 1 Panel of autoantibodies – � � � GAD 65 - Glutamic acid decarboxylase – ICA - Islet Cell Cytoplasmic Autoantibodies IAA - Insulin Autoantibodies

Poll Question 5 What factors would make you suspect type 1 diabetes? a. Pt has a history of celiac disease b. Pt presents with low HDL cholesterol c. Friend tells you she has been eating "tons of sweets“ d. Pt is slightly overweight
 �Thyroid disease")
Type 1 Diabetes Associated with other immune conditions �Celiac disease (gluten intolerance) �Thyroid disease �Addison’s Disease �Rheumatoid arthritis �Other

Type 1 Summary �Autoimmune pancreatic destruction �Need insulin replacement therapy �Often first present in DKA �At risk for other autoimmune diseases �Eval coping strategies

Patti Labelle "divabetic” “I have diabetes, it doesn’t have me”

Path to Type 2 Diabetes

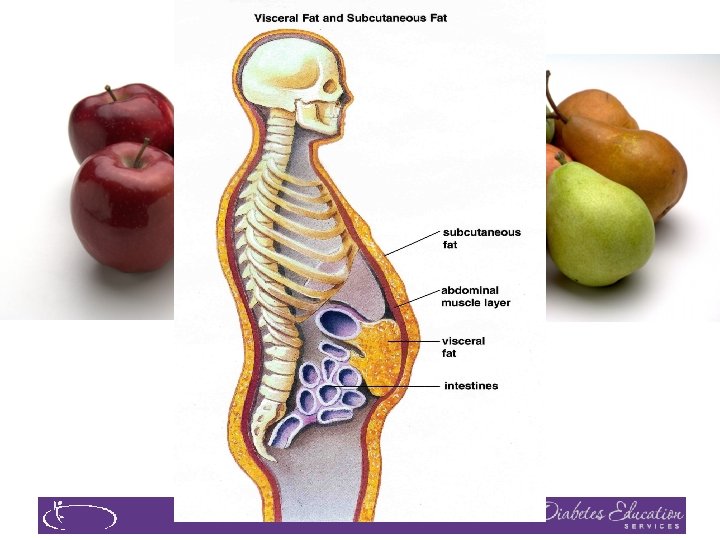
BMI – Visual Image

Insulin Resistance is the Seed

Factors Associated with Insulin Resistance �Abdominal obesity �Sedentary lifestyle �Genetics / Ethnicity �Gestational Diabetes �Polycystic ovary syndrome �Acanthosis Nigricans �Obstructive Sleep Apnea �Cancer American College of Endocrinology, 2001

Acanthosis Nigricans
 �Signals high insulin levels in bloodstream �Patches of darkened skin over")
Acanthosis Nigricans (AN) �Signals high insulin levels in bloodstream �Patches of darkened skin over parts of body that bend or rub against each other � Neck, underarm, waistline, groin, knuckles, elbows, toes � Skin tags on neck and darkened areas around eyes, nose and cheeks. �No cure, lesions regress with treatment of insulin resistance
 1. Start")
Pre Diabetes & Type 2 - Screening Guidelines (ADA Clinical Practice Guidelines) 1. Start screening all people at age 45 or anyone who is overweight (BMI 25, Asians BMI 23 ) with one or > additional risk factor: � � � First-degree relative w/ diabetes Member of a high-risk ethnic population Habitual physical inactivity Pre. Diabetes History of heart disease
 Risk factors cont’d")
Diabetes 2 - Who is at Risk? (ADA Clinical Practice Guidelines) Risk factors cont’d �HTN - BP > 140/90 �HDL < 35 or triglycerides > 250 �history of Gestational Diabetes Mellitus � Polycystic ovary syndrome (PCOS) � Other conditions assoc w/ insulin resistance: � Severe obesity, acanthosis nigricans (AN)

Poll Question 7 �Frequent skin and yeast infections in people with diabetes are: a. A sign of poor hygiene b. Due to poor diet c. A sign of ongoing hyperglycemia d. A result of high sugar intake

Signs of Diabetes �Polyuria �Polydipsia �Polyphasia �Weight loss �Fatigue �Skin and other infections �Blurry vision Glycosuria, H 2 O losses Dehydration Fuel Depletion Loss of body tissue, H 2 O Poor energy utilization Hyperglycemia increases incidence of infection Osmotic changes
 with")
What is Type 2 Diabetes? �Complex metabolic disorder …. (Insulin resistance and deficiency) with social, behavioral and environmental risk factors unmasking the effects of genetic susceptibility. New Diagnosis? Call 800 – DIABETES to request “Getting Started Kit” www. Diabetes. org

Natural Progression of Type 2 Diabetes Postprandial glucose Plasma Glucose Fasting glucose 126 mg/d. L Insulin resistance Relative -Cell Function Insulin secretion -20 -10 0 10 20 Years of Diabetes Prior to diagnosis Adapted from Bergenstal et al. 2000; International Diabetes Center. After diagnosis 30

Ominous Octet Decreased satiation neurotransmission Decreased amylin, -cell secretion 80% loss at dx Increased glucagon secretion Increased renal glucose reabsorption Decreased Gut hormones G I I G I G Increase glucose production I I G G G Increased lipolysis G I G Decreased glucose uptake

Life Study – Mrs. Jones is 62 years old, with a BMI of 36 and complains of feeling tired and urinating several times a night. She has an urinary tract infection. Her A 1 c is 8. 3%, glucose 237. She is hypertensive with a history of gestational diabetes. No ketones in urine. �What are her risk factors and signs of diabetes? �You find a few moments to teach and she asks you some questions.
 �No")
What negative words / phrases have you heard regarding people with diabetes? �Cheat(er) �No will power �Diabetic �Lazy, weak �Non-compliant �Train wreck �Frequent Flyer �Non-adherent �Refuses to check blood sugar �Forgot log book again �Refuses to take their meds as directed �Eats junk food �Loves sugar �They brought it on themselves

Language of Diabetes Education Old Way �Control diabetes �Test BG �Patient �Normal BG �Non-adherent, compliant �Refuse New Way �Manage �Check �Participant �BG in target range �Focus on what they are accomplishing �Decided, chose

Terminology matters in medical communication about obesity �For people with BMI >30, preferred terms � “person with elevated BMI”. � “person with obesity” � “person with excess weight” �For descriptions of BMI >40 � “class III obesity” � “severe BMI” and � “extreme BMI” Pearl RL, et al. JAMA Surg. Sept 2018; doi: 10. 1001/jamasurg. 2018. 2702
 �Imparts hope �Respectful, inclusive �Neutral, �Fosters collaboration nonjudgmental �")
Let’s use language that (is) �Imparts hope �Respectful, inclusive �Neutral, �Fosters collaboration nonjudgmental � Based on fact, actions or biology � Free from stigma between person and provider �Avoids shame and blame

Guiding Language Principles Strength Based Person-first �Emphasize what �Words that indicate people know, what they can do. �Focus on strengths that empower people awareness �Sense of dignity �Positive attitude toward person with disability

Mrs. Jones asks you What Do You Say? �What is diabetes? �They say I am a diabetic because I am obese? �How am I going to control this? �What is a normal blood sugar? �Do I have to test my blood sugars? �My doctor told me to stay away from white foods. Is that true?

Look Beyond Diabetes � ACE – Adverse Childhood Experiences � Feelings around their diabetes � Cultural traditions, family system. � Social, religious and employment influences � Personal factors: attitudes, cognitive factors, literacy, learning styles, health beliefs � Depression, anxiety � Mental illness � Addiction issues

Empowerment Defined �“Helping people discover and develop their inherent capacity to be responsible for their own lives and gain mastery over their diabetes”. �Posits: � Choices made by the person (not HCPs) have greatest impact. � PWD are in control of their self-management � The consequences of self-management decisions affect PWD most. It is their right and responsibility to be the primary decision makers.

Traditional vs Empowerment Based Traditional Empowerment �DM is a physical illness �DM is biopsychosocial �HCP is viewed as �PWD is viewed as teacher responsible for outcomes �Emotional issues are separate components �Lack of goal attainment is viewed as failure �Behavior change are externally problem solver /self manager �Experiences are integral with clinical content �Lack of goal attainment is a learning experience �Behavior change is internally motivated

Diabetes is also associated with �Fatty liver disease �Obstructive sleep apnea �Cancer; pancreas, liver, breast �Alzheimer’s �Depression

Other Types of Diabetes �Gestational �Other specific types of diabetes

Other Causes of Hyperglycemia �Steroids �Agent Orange �Tube feedings / TPN �Transplant medications �Cystic Fibrosis Regardless of cause, requires treatment �Insulin always works �Sign of pancreatic malfunction

Poll Question 8 �Which of the following is true about gestational diabetes? A. GDM can be identified in the first trimester. B. Children of women w/ GDM are at greater risk of type 1 C. The rates of GDM are decreasing D. Women can decrease their risk of getting GDM

Gestational DM ~ 7% of all Pregnancies �GDM prevalence increased � ∼ 10– 100% during the past 20 yrs �Native Americans, Asians, Hispanics, African-American women at highest risk �Immediately after pregnancy, 5% to 10% of GDM diagnosed with type 2 diabetes � Within 5 years, 50% chance of developing DM in next 5 years.

Increasing Prevalence – A public health perspective �Body weight before and during pregnancy influences risk of GDM and future diabetes �Children born to women with GDM at greater risk of diabetes �Focus on prevention

Screen Pregnant Women Before 13 weeks �Screen for undiagnosed Type 2 at the first prenatal visit using standard risk factors. �Women found to have diabetes at their initial prenatal visit treated as “Diabetes in Pregnancy” �If normal, recheck at 2428 weeks

Postpartum after GDM � 50% risk of getting diabetes in 5 years �Screen at 6 -12 wks post partum �Repeat at 3 yr intervals or signs of DM � Encourage Breast Feeding � Decreases risk of diabetes in mom 50% � Encourage weight control � Encourage exercise � Make sure connected with health care � Lipid profile/ follow BP � Preconception counseling

Key points �At the center of diabetes is someone living with it everyday. �Focus on their successes �Coach and support

Thank You �Discover more articles and info in your Student Center Resources Tab �Please contact us with any questions �Diabetes. Ed. University. com
- Slides: 68