Diabetes Endocrine Disorder Pregnancy is diabetogenic 1 Diabetes
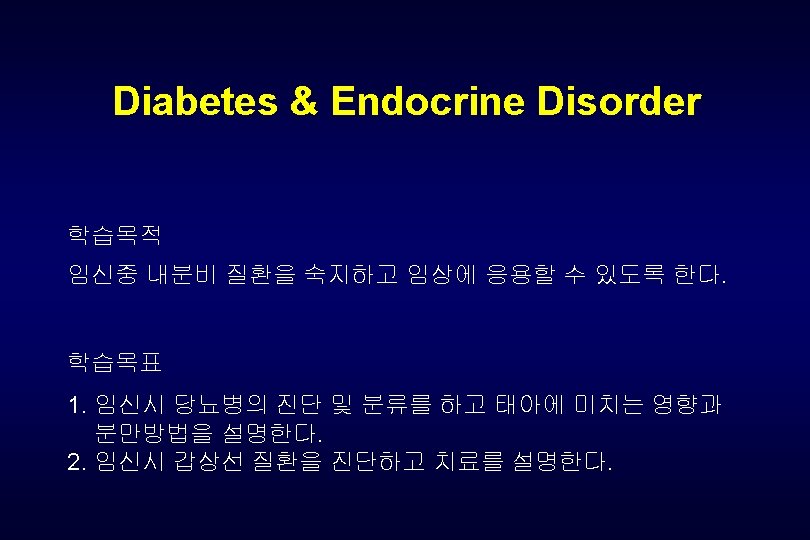

Diabetes & Endocrine Disorder Pregnancy is diabetogenic! 1. Diabetes mellitus Diabetes before preg. (overt diabetes) during preg. (gestational diabetes) Gestational D-M : 5%. . Fasting hyperglycemia Class B. H…. . Mostly overt diabetes Glucosuria : not reflect impaired glucose tolerance but rather augmented glomerular filtration, nonetheless, glucosuria needs more investigation
 Type 1 (Insulin dependent) 2) Type 2 (Noninsulin dependent)")
A. Classification of diabetes 1) Type 1 (Insulin dependent) 2) Type 2 (Noninsulin dependent) Table 1. Characteristics Type 1 Type 2 genetic locus age at onset habitus plasma insulin plasma glucagon Acute Cx insulin Tx sulfonylurea chromosome 6 young(<40) nl to wasted low to absent high, suppressible ketoacidosis response unresponse chromosome 11(? ) older(>40) obese nl to high, resistant hyperosmolar coma resistant response
 Secondary diabetes a) Pancreatic disease (pancreatectomy, pancreatic insufficiency, hemochromatosis)")
A. Classification of diabetes 3) Secondary diabetes a) Pancreatic disease (pancreatectomy, pancreatic insufficiency, hemochromatosis) b) Hormonal (excess counterinsulin hormones…. . Cushigs syndrome, acromegaly, pheochromocytoma) c) Drug-induced (thiazide diuretics, steroid, phenytoin) d) Associated with specific genetic syndromes (lipodystrophy, myotonic dystrophy, ataxia-telangiectasia)
 Impaired glucose tolerance(IGT) chemical, latent, borderline, subclinical diabetes 5)")
A. Classification of diabetes 4) Impaired glucose tolerance(IGT) chemical, latent, borderline, subclinical diabetes 5) gestational diabetes : glucose intolerance with onset during pregnancy
 Risk factors requiring diabetes screening a) obesity(>200 Lb or")
C. Diagnosis during pregnancy 1) Risk factors requiring diabetes screening a) obesity(>200 Lb or 15% of nonpreg. ideal BW) b) positive family history of DM (sibling or parent) c) Hx of stillbirth d) Hx of a large infant delivery (>4000 gm) e) glucosuria f) Hx of unexplained neonatal death g) Hx of prematurity h) Hx of preeclampsia as a multipara i) polyhydramnios j) Hx of traumatic delivery associated with neurologic disorder in infant k) poor reproductive history ( > 3 spontaneous abortions in the 1 st or 2 nd trimester) l) chronic hypertension m) recurrent severe moniliasis n) age > 30 years o) Hx of diabetes in a previous pregnancy
 Screening test: Universal screening risk factor screen between gest.")
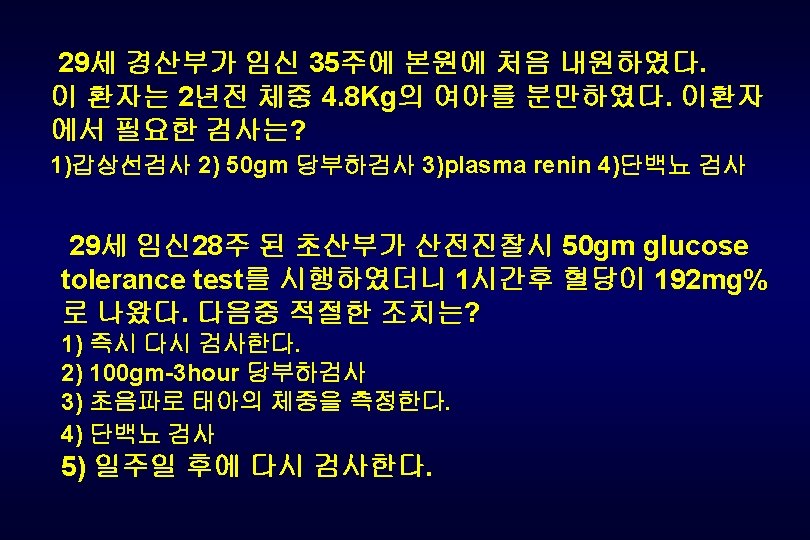
C. Diagnosis during pregnancy 2) Screening test: Universal screening risk factor screen between gest. 24 and 28 주 using 50 gm oral GTT … 1 hour plasma > 140 mg/dl 이면 100 gm OGTT 실시 Table 3. Criteria for diagnosis of gestational diabetes using 100 gm of glucose taken orally Plasma Glucose (mg/d. L) Timing of Measurement National Diabetes Data Group(1979) Carpenter and Coustan (1982) Fasting 1 hr 2 hr 3 hr 105 190 165 145 95 180 155 140

D. Gestational Diabetes gest. diabetes 환자의 50% 이상이 20년 내로 overt diabetes 로 발전되고 그 중 자손에게 obesity , diabetes 의 가능성이 높다. Overt DM : high risk for IUFD gestational DM(A 1) : not apparent but A 2 gest. DM…. . IUFD associated
 increased preeclampsia – eclampsia (× 4) 2) infection more often")
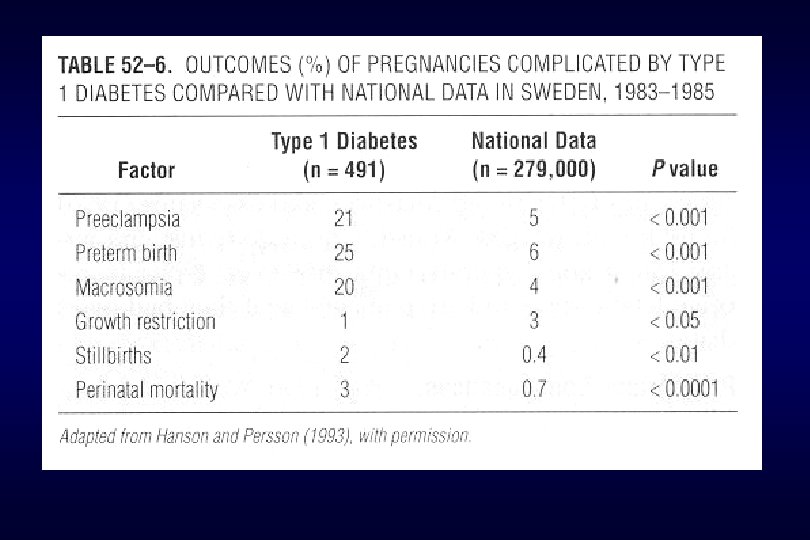
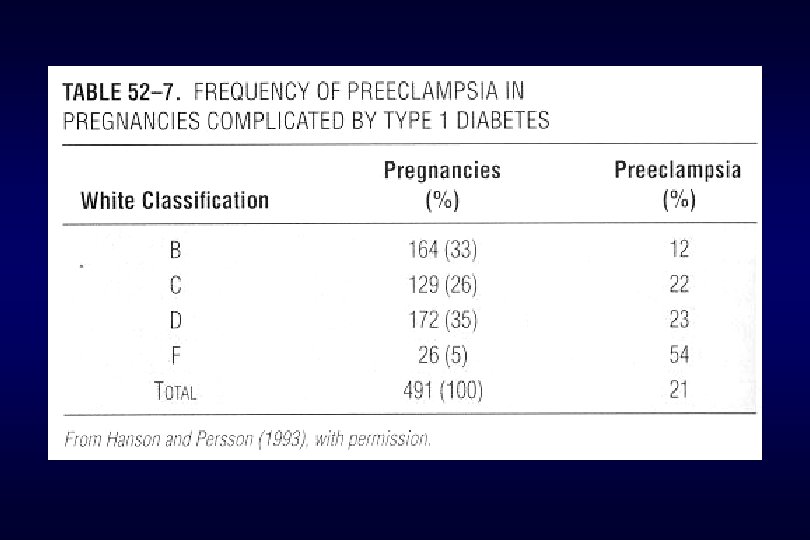
E. Maternal effects 1) increased preeclampsia – eclampsia (× 4) 2) infection more often 3) difficult delivery with injury to the birth canal 4) increased c/sec 5) hydramnios 6) increased maternal mortality
 increased perinatal mortality : unexplained IUFD, congenital anomalies, RDS 2)")
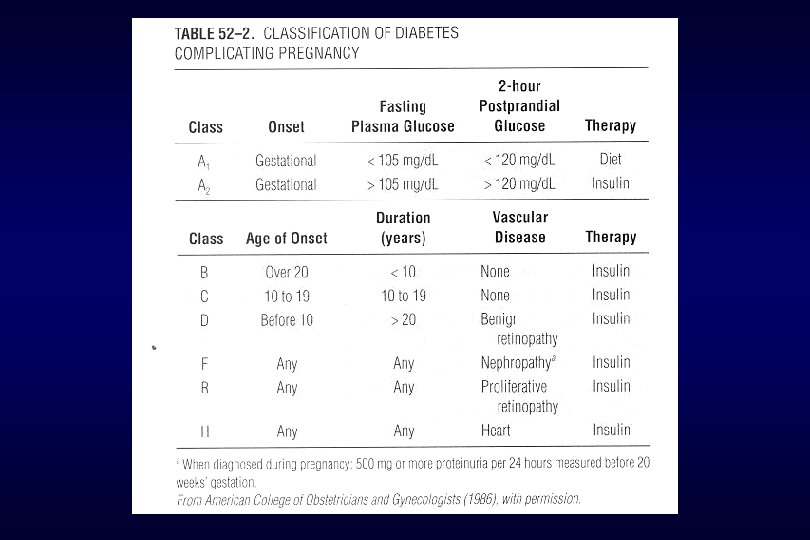
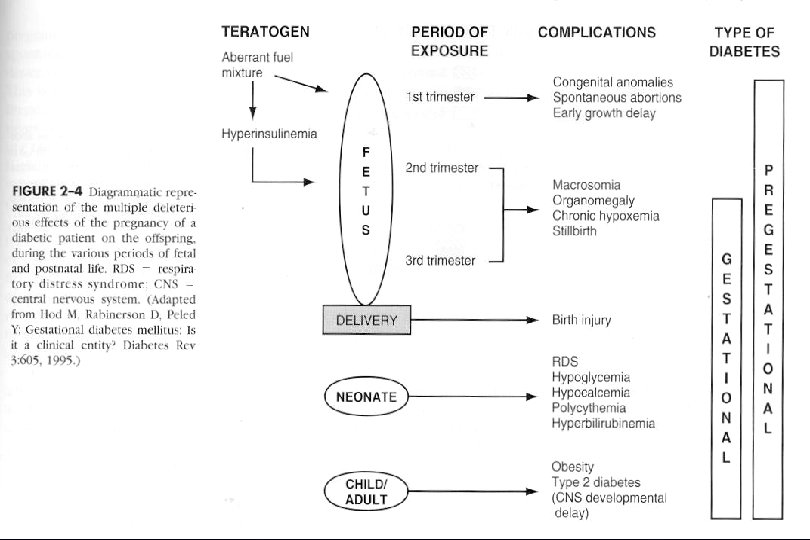
F. Fetal effects 1) increased perinatal mortality : unexplained IUFD, congenital anomalies, RDS 2) increased perinatal morbidity macrosomia, RDS, polycythemia, hypoglycemia, hypocalcemia, hypomagnesemia, hyperbilirubinemia 3) predisposition to diabetes 4) vigorous muscular exertion in insulin requirement 5) after delivery. . decreased in insulin requirement
 abnormal CHO metabolism should be detected and")
H. Management 1. General principles a) abnormal CHO metabolism should be detected and defined precisely b) maternal glycemia control is important factor in determining fetal outcome c) pregnant women with diabetes and fetus should be cared for throughout pregnancy by experienced and skilled individuals d) newborn infant with diabetes should be cared from birth time by experienced individual
 a) diet ( FBS<105 mg,")
H. Management 2. Gestational Diabetes (Class A diabetes) a) diet ( FBS<105 mg, or 2 hour plasma glucose<120 mg유지 ) b) exercise ( upper body C_V training lowers glucose ) c) insulin ( A 2 diabetes ) d) delivered at term ( gest. D. M. which do not require insulin seldom early delivery or intervention) e) but if require insulin, fetal test and manage need as if overt DM f) postpartum management 75 mg oral GT (50% of gest D. M. develop overt DM within 20 yrs) insulin Tx before 24 wks is a powerful predictor of diabetes after preg.

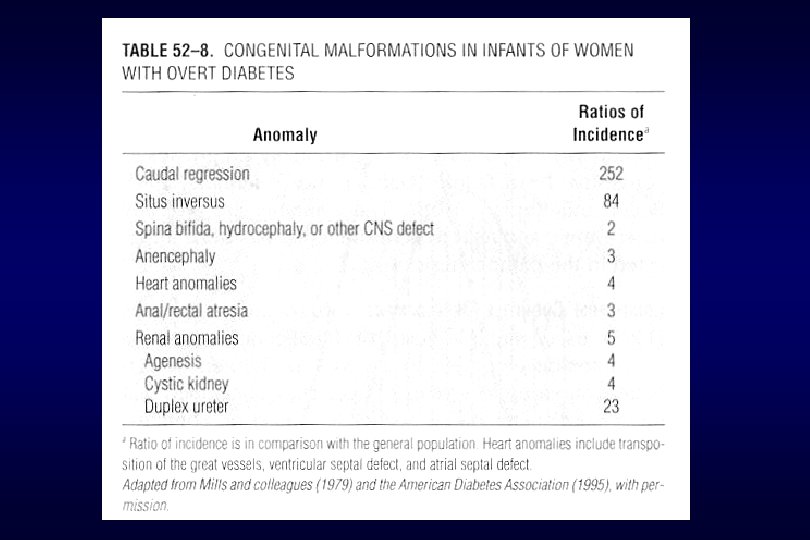
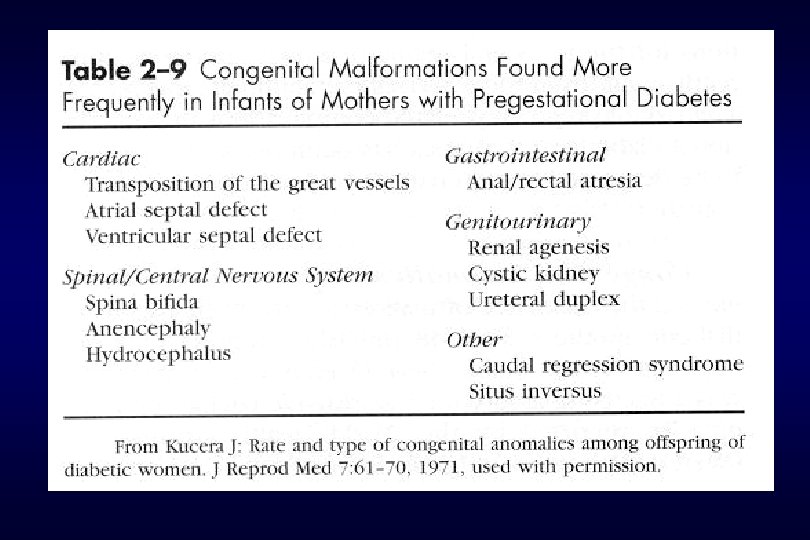
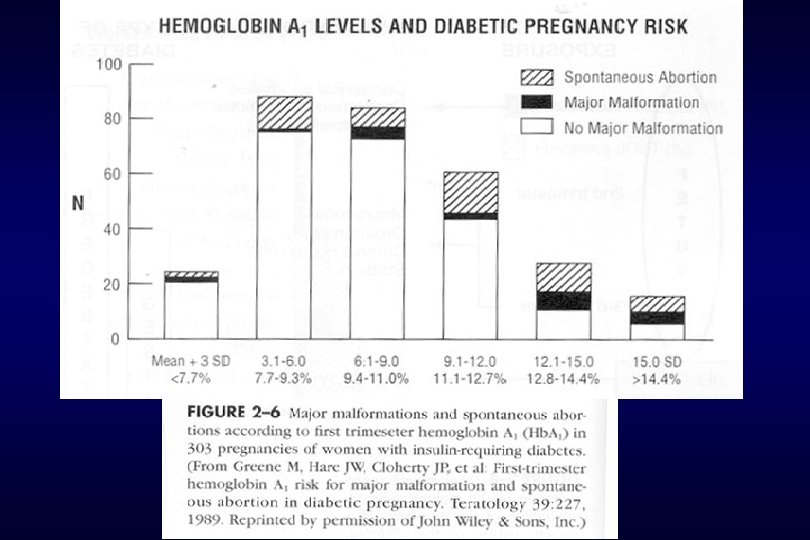
I. Overt Diabetes significant impact on preg. outcome and successful outcome is related to degree of diabetes control and more to intensity of underlying maternal cardiovascular or renal dis. 1. Effect on the fetus fetal death, cong. anomaly, abortion, preeclampsia, preterm, macrosomia, IUGR, Hydramnios, RDS, Hypoglycemia, Hyperbilirubinemia, cardiac hypertrophy, long-term cognitive development, altered fetal growth abortion high : glyco. Hb. A 1 > 12%, persistent FBS > 120 mg Hyperglycemia induces oxidative free-radical molecule…. . embryotoxic antioxidants reduces fetal malformation

I. Overt Diabetes 2. Effect on the mother diabetic retinopathy neuropathy nephropathy preeclampsia ketoacidosis infections

I. Overt Diabetes 3. Management preconception : begin before preg. and specific goals during each trimester normalize blood sugar before conception and early preg. Hb A 1 c>10%…. . high malformation, folate(400 g/d. given) 1 st Trimester : oral hypoglycemic agents : not use……… insulin use 2 nd Trimester : maternal alpha-fetoprotein, sonogram 3 rd Trimester : weekly visit for glucose and evaluated preeclampsia sonogram, fetal surveillance test(26 -32 wk)
 Diet during pregnancy(WT gain 10 -12 kg)")
I. Overt Diabetes 3. Management a) Diet during pregnancy(WT gain 10 -12 kg) cal + 300 Kcal/day protein + 30 gm/day Iron = 30 -60 gm Ca + 400 mg Folic acid + 400 gm Cal 38 cal/kg(2000 -2400) protein 1. 3 g/kg CHO 50 -60% protein 12 -20% saturated fat < 10% polyunsat fat : 10% monounsat fat reminder b) Insulin
 assessment of diabetes control glucose Hb A")
I. Overt Diabetes 3. Management c) assessment of diabetes control glucose Hb A 1 c (<8%)…every 4 -6 wks d) timing of delivery even if preterm labor, not use tocolytic agents : factors determining timing of delivery degree of control of maternal diabetes lung maturity (L/S ration > 2 ) and size of baby presence and severity of preeclampsia other clinical factors(Hydramnios) previous obstetric history adverse fetures on fetal well being test
 Method of delivery class B, C……. c/sec")
I. Overt Diabetes 3. Management e) Method of delivery class B, C……. c/sec criteria for induction of labor : fetus is not excessively large pelvis not contracted parity is not great cervix is soft, effacement, some dilated presenting part is vertex and fixed in the pelvis
 Contraception barriers methods, sterilization oral pill: high")
I. Overt Diabetes 3. Management f) Contraception barriers methods, sterilization oral pill: high in thrombophlebitis, stroke, M. infarction and but low dose pill is low risk progestin implant system(Norplant) IUD: pelvic infection risk is high but ideal devices

2. hyperthyroidism A. Changes in maternal thyroid function during pregnancy Placenta Mother Fetus TBG T 4 T 3 Estrogen TSH FT 3. 4 h. CG TSH Goiter I TRH T 4 T 3 TSH r. T 3 T 2

B. maternal-fetal thyroid relationship and the placental transfer of medication to the fetus Mother HORMONS TRH TSH T 4 T 3 TREATMENT PTU Methimazole Iodine 131 I Lithium Propranolol Placenta Fetus (After 20 weeks) HYPOTHALAM US TRH PITUITARY TSH T 4 RT 3 T 3
 reasons for differentiating signs and symptoms")
2. hyperthyroidism C. Diagnosis during pregnancy 1) reasons for differentiating signs and symptoms of hyperthyroidism during pregnancy a) some degree of heat intolerance is common b) modest tachycardia c) increased plasma thyroxine and radioiodine uptake 2) helpful signs for identifying hyperthyroidism a) excessive tachycardia b) enlarged thyroid gland c) exophthalmos d) failure to gain WT 3) Hormone profile …. increased free T 4

2. hyperthyroidism D. Pregnancy outcome Maternal…. preeclampsia, heart failure Perinatal…. preterm delivery, IUGR, stillbirth, thyroid storm above outcome are high in untreated thyrotoxicosis compared to treated and eutyroid status
 Propylthiouracil(PTU) side effects Mother : agranulocytosis, allergic reaction,")
2. hyperthyroidism E. Management 1) Propylthiouracil(PTU) side effects Mother : agranulocytosis, allergic reaction, arthralgia fetus : goiter hypothyroidism, decreased intellectual development breast feeding : contraindication supplemental thyroid hormone : undesirable 2) subtotal thyroidectomy during 2 nd trimester
 iodine, propranolol iodine : only preceding the time")
2. hyperthyroidism E. Management 3) iodine, propranolol iodine : only preceding the time of thyroidectomy side effects of propranolol fetal distress during labor low Apgar score growth retardation hypoglycemia hyperbilirubinemia
 physical exam, palpable goiter")
2. hyperthyroidism F. evaluation of the newborn infant 1) physical exam, palpable goiter 2) cord blood for T 4, TSH, TSAb G. Effect of thyrotoxicosis on the fetus transient thyrotoxicosis neonatal hypothyroidism…. . fetal goiter

3. hypothyroidism high TSH, low free T 4 pregnancy outcome with overt and subclinical hypothyroidism: preeclampsia, abruptio placentae, anemia, postpartum hemorrhage, cardiac dysfunction, IUGR, stillbirth Tx : Thyroxine subclinical hypothyroidism ; T 4 and T 3… normal, high TSH
 Pregnancy alter the natural history of SLE not accompanied")
1. Systemic lupus erythematosus 1) Pregnancy alter the natural history of SLE not accompanied by increased prevalence of major systemic nonrenal manifestation of SLE 2) are the effects of SLE on renal function exaggerated by Preg. Renal function remained good in the majority in the patients Induced abortion : no deleterious effect on renal function
 Effect of SLE high fetal wastage stillbirth : 24% preterm birth : 33%")
4) Effect of SLE high fetal wastage stillbirth : 24% preterm birth : 33% IUGR 3) Phamacological treatment should be altered during preg. Glucorticoid, azathioprine – same dose to non preg women Increased dosage during labor and postpartum 2 months

B. SLE versus preeclampsia Superimposed preeclampsia : more often in lupus nephropathy Difficulty in differentiation clinically Common in SLE women CNS involvement Thrombocytopenia Vascular and renal involvement

C. Effects on fetus and infant Increased IUGR Neonatal SLE : transplacental Ig. G Cutaneous lupus, thrombocytopenia : transient Autoimmune hemolysis

D. Subsequent reproduction Prolong remission : undertaken pregnancy Advice tubal ligation due to poor prognosis for fetus and mother E. Lupus anticoagulant Increased fetal wastage
 Amelioration of activity of disease :")
2. Rheumatoid arthritis Disease activity diminished during pregnancy(2/3) Amelioration of activity of disease : 62% , no change : 38% Treatment : drug of choice in preg. : aspirin Aspirin effects on fetus : impaired hemostasis, prolonged gestation premature closure of ductus arteriosus
")
NEUROLOGICAL DISORDER 1. Epilepsies A. Factors for increasing risk of seizures in pregnancy 1) N/ V may interfere with ingestion and absorption of anticonvulsants 2) Medication may be withhold during labor delivery and puerperium 3) Phenytoin is cleared more rapidly in pregnancy

B. Effect of anticonvulsant on fetus-infant Aminoglutethimide : D Bromides : D Carbamazepine : C Clonazepam : C Ethosuximide : C Ethotoin : D Felbamate : C Gabapentin : C Lamotrigine : C Magnesium sulfate : B Mephenytoin : C Mephobarbital : D Metharbital : B Methosuximide : D Paramethadione : D Phenobarbital : D Phensuximide : D Phenytoin : D Primidone : D Trimethadione : D Valproic Acid : D
 congenital malformation a) Fetal phenytoin syndrome Craniofacial")
B. Effect of anticonvulsant on fetus-infant 1) congenital malformation a) Fetal phenytoin syndrome Craniofacial anomalies, limb dysmorphosis impaired physical and mental growth congenital heart lesion cleft lip and palate b) deficiency of vit. K – dependent clotting factors in neonate ……. hemorrhagic disease of newborn
carbamazepine trimethadione, valproic acid. . teratogenic 3) counseling")
B. Effect of anticonvulsant on fetus-infant 2)carbamazepine trimethadione, valproic acid. . teratogenic 3) counseling to mother a)stop or not stop anticonvulsant b)folic acid deficiency

2. Cerebrovascular Diseases Ischemic strokes : arterial thrombosis, arterial embolism, vasculitis, moya venous thrombosis Hemorragic strokes: hypertensive, saccular aneurysm, arteriovenous malformation

PSYCHIATRIC DISORDER 1. Classification Major disorder : depression, MDI Schizophrenic disorders Anxiety disorders : obessive-compulsive disorders Personality disorder

PSYCHIATRIC DISORDER 2. Effect of pregnancy on mental illness High recur in puerperium Amitriptyline (D), imipramine(D), fuloxetine(B), chlorpromazine(D), clozapine(B), haloperidol(C), diazepam(D), lithium(D), most-teratogenic

1. Physiological Skin changes in Pregnancy A. hormonal changes due to increase the Plasma availability of estrogen. progesterone, androgen. B. changes in concentrations of some adrena 1 cortisol aldosterone, and deoxycorticosterone. C. enlargement of the intermediate lobe of the pituitary gland. and elevated plasma level of melanocyte-stimulating hormone(MSH)

1. Physiological Skin changes in Pregnancy D. production of pro-opiomelanocortin from p. Iacenta 1 extracts; a source of - - melanocyte-stimulating hormone. Hyperpigmentation ; linea nigra, cholasma, me. Iasma Nevi ; en. Iarged and darken. confused for a ma 1 ig 1 ant me. Ianoma changes in hair growth vascular changes : spider angiomas. palmar erythema, capillary hemangiomas epulis of pregnancy : growth of gum capillaries. pyogenic granuloma

Linea Nigra

2. Pruritic Urticarial Papules and Plaques of pregnancy A. intensely pruritic cutaneous eruption in late pregancy B. more common in nulliparas and seldom recurs in subsequent pregnancies C. periumbi 1 cal area. spread to thighs and extremities D. no vesicle. no bullae, and negative immunofluorescence E. no adverse perinatal morbidity, and regress within 1 to 4 weeks of following delivery

Pruritic Urticarial Papules and Plaques of Pregnancy

3. Papular Eruption of Pregnancy A. small pruritic papules, excoriated lesion on the forearms and trunk B. no vesicle and bullae, not recur in subsequent pregnancy

4. Herpes Gestationis A. pruritic blistering skin eruption in multiparous women B. recur in subsequent pregnancy more severe C. large, tense vesicle and bullae D. herpes gestaionis serum factor : C 3 and Ig. G deposition at basement membrane E. preterm delivery, SGA, transient enonatal lesion (5 -10%)

5. Impetigo Herpetiformis A. sterile pustule, erythematous patchs and mucus membrane involved B. microabscess formation and secondary infection, sepsis C. systemic steroid with antimicrobials

6. Acne vitamin A ; increase in birth defects, at least 25, 000 to 50, 000 IU daily (ACOG) isotretinoin ; vitamin A isomeres, prescribed for severe cystic acne, highly teratogenic etretinate ; used to treat psoriasis, category X long elimination times. more than 2 years after cessation of therapy tretinoin ; category B, topically applied gel for acne vulgaris
 the ovaries may be removed")
Principles of Cancer Therapy during Pregnancy A. Surgery 1) the ovaries may be removed safely after 8 weeks’ gestation because placental progesterone production is adequate. 2) diagnostic and staging operation ; defer until the second-trimester 3) therapeutic surgery should be performed regardless of gestation B. radiation therapy 1) cell death, carcinogenesis, genetic effects of fetus generation 2) adversed effects of high-dose radiation ; microcephaly, mental radiation 3) the most critical time ; 8 and 15 weeks 4) less than 0. 05 Gy ; negligible risk for major malformation 5) therapeutic radiation ; contraindicated because of fetal death or damage head and neck, supradiaphragmatic areas with abdominal shielding ; relatively safer
 antineoplastic drugs category D")
Principles of Cancer Therapy during Pregnancy C. chemotherapy ; 1) antineoplastic drugs category D 2) potentially teratogenic susceptibility between 5 and 10 weeks’ gestation(10%) 3) breast feeding is not recommended D. Ovarian function and fertility after cancer therapy 1) depressed follicular maturation and ovarian fibrosis 2) depends on women’s age and the drug dose given 3) peripubertal ovary ; resistant to effects of chemotherapy 4) if preserved fertility, not increased incidence of abortion, fetal chromosomal damage, or fetal anomalies
 delays in diagnosis")
2. Breast Carcinoma A. Effects of pregnancy on breast cancer 1) delays in diagnosis due to hormonal influence 2) during lactation ; more advanced stages of cancer at diagnosis and worse prognosis 3) interruption of pregnancy ; no influence on the course B. Diagnosis and treatment 1) prompt an aggressive plan by fine-needle aspiration or open biopsy 2) mammography ; negligible for fetal risk (less than 0. 01 Gy) 3) surgery ; radical mastectomy or total mastectomy, not delayed 4) radiotherapy ; not recommended because abdominal scatter is considerable 5) adjuvant chemotherapy with node-positive cancer
 no difference in recurrence or")
2. Breast Carcinoma C. pregnancy following breast cancer 1) no difference in recurrence or distance metastasis 2) advise a delay of 2 to 3 years

3. Lymphoma and Leukemia Hodgkin disease ; limit diagnostic radiographic studies susceptible to infection and sepsis non-Hodgkin lymphoma ; rare, 5 -1 -% of HIV infected persons develop a lymphoma A. Leukemia 1) improved survival rate by remission with chemotherapy 2) preterm delivery, stillbirth, congenital leukemia 3) termination is not recommended to improve the prognosis. 4) infection and hemorrhage at the time of delivery 5) anemia, neutropenia, thrombocytopenia
 pregnancy is associated with increased melanocyte-stimulating")
3. Lymphoma and Leukemia B. Malignant Melanoma 1) pregnancy is associated with increased melanocyte-stimulating hormone 2) changes in contour, surface elevation, discoloration, itching, bleeding, or ulceration; biopsy recommended 3) future pregnancies ; avoided for 3 to 5 years after treatment 4) metastatic to the fetus or placenta ; one third of malignancies
 1. 3 per 1000 for CIN")
4. Genital cancer A. Cervical intraepithelial neoplasia 1) 1. 3 per 1000 for CIN and 1 per 2000 pregnancies for invasive carcinoma 2) colposcopic evaluation ; well exposed transformation zone due to physiologic eversion 3) conization during pregnancy ; less satisfactory 4) mild dysplasia – colposcopically no lesion ; repeat smear and follow up moderate to severe dysplasia – biopsy – confirmed intraepithelial neoplasia – allowed to deliver vaginally and given definitive treatment after delivery
 2) 3) 4) difficult")
4. Genital cancer B. invasive carcinoma of the cervix 1) 2) 3) 4) difficult to accurate identification of extent of cancer similar survival rate for pregnant and nonpregnant women mode of delivery ; not affect maternal survival radical hysterectomy plus pelvic lymphadenectomy before 20 weeks ; hysterectomy with the fetus in situ in later pregnancy ; hysterotomy first 5) early in pregnancy ; external irradiation- spontaneous abortion second trimester ; hysterectomy and 1 weeks later radiation therapy endometrial carcinoma ; rare, women past the reproductive age
 1 of every 100 pregnant women ;")
4. Genital cancer C. ovarian carcinoma 1) 1 of every 100 pregnant women ; surgical exploration for an adnexal mass(ACOG) 2) increased detection because of ultrasonography 3) not alter the prognosis 4) complete surgical staging, higher proportion of low-malignant potential tumors 5) endodermal sinus tumor ; elevated maternal serum AFP

4. Genital cancer D. Vulvar cancer ; papillomavirus association any suspicious vulvar lesion should be biopsied

Some causes of fetal and neonatal infections Intrauterine Transplacental - rubella, CMV, V-Z, coxackie, parvovirus, HIV, syphilis, listeriosis, toxoplasmosis, malaria Ascending chorioamnionitis - bacteria associated with PROM Intrapartum Maternal exposure - gonorrhea, herpesvirus, chlamydia, papilloma virus, group B streptococcus, HBV, HIV External contamination - staphylococcus, coliforms Neonatal Human transmission - staphylococcus, viruses Respiratory equipment and catheters - staphylococcus, coliforms

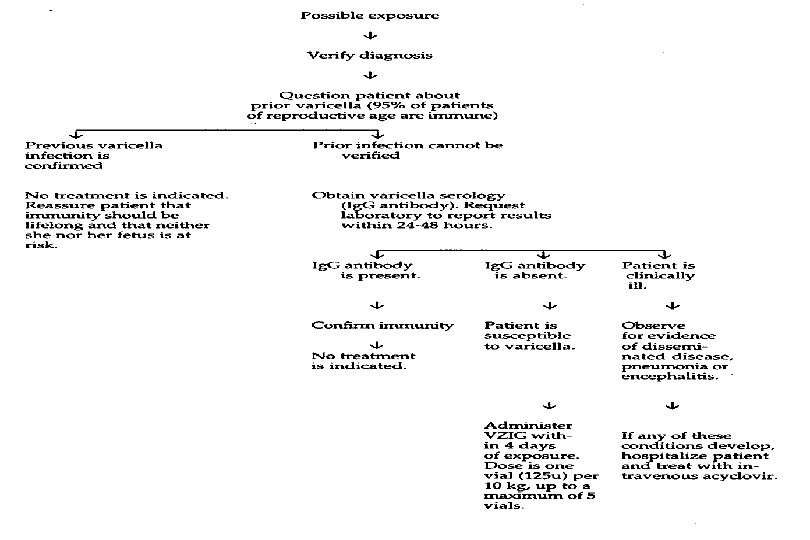
II. Viral Infections 1. Varicella-zoster • DNA herpes virus • Most adults have acquired chickenpox during childhood and are immune • Arvin and Paryani, 1986 4 of 43, infected pregnant women developed pnemonitis. • Varicella infection in adults or pregnant woman is more severe. • Latent in dorsal root ganglia after primary infection (chickenpox) > reactivation > zoster infection

Maternal chickenpox during pregnancy may cause congenital malformation by transplacental infection --- chorioretinitis, cerebral cortical atrophy, hydronephrosis, cutaneous and bony leg defects 13 -20 weeks : highest risk ( 1 -2% congenital malformation ) Enders, 1994 1373 women, no clinical evidence of congenital varicella infection after 20 weeks
 VZIG 125 U/10 kg within 96 hours VZIG to neonate ---- maternal")
Prevention 1) VZIG 125 U/10 kg within 96 hours VZIG to neonate ---- maternal clinical disease within 5 days before delivery or 2 days postpartum 2) Attenuated live-virus vaccine All children (1 -12 yrs) Not recommended for pregnant women Treatment Acyclovir --- serious ill adults and neonates

2. Influenza • Orthomyxoviridae family • influenza A is more serious than B • CDC, 1995 Vaccination is recommended for pregnant women who have underlying disease and heath-care workers are exposed. Safe for pregnant women • Amantadine within 48 hrs of onset of Sx --- specific activity against influenza A • No congenital malformation neural tube defect ( Lynberg, 1994 ) schizophrenia ( Kunugi, 1995 ) • Common cold had a four to fivefold increased risk of anencephaly ( Kurppa, 1991 )
 single stranded RNA virus of family Paramyxoviridae erythematous maculopopular rash most")
3. Rubeola (Measles) single stranded RNA virus of family Paramyxoviridae erythematous maculopopular rash most adult are immune to measles Siegel, 1973 not teratogenic but increase in prematurity and first trimester abortion Passive immunization ----s. IG 5 ml IM within 3 days in infection before birth Vaccination is not done during pregnancy. Susceptible woman is recommended routine postpartum vaccination

4. Enterovirus infections • RNA piconavirus including poliovirus, coxsachivirus, echovirus • Replicate in the enteric tract • Dahlquist, 1995 Maternal enteroviral infection is a risk factor for childhood-onset diabetes • fecal-oral route, resiratory, transplacentally, birth process
 Coxsachivirus • Browen and Karunas, 1972 • --- congenital malformation ^ • hepatitis,")
1) Coxsachivirus • Browen and Karunas, 1972 • --- congenital malformation ^ • hepatitis, myocarditis, encephalomyelitis, fetal death • Strong and Young, 1995 • --- clinical chorioamnionitis associated with maternal • coxsachie viremia • Dommergues, 1994 • --- fetal ventriculomegaly, cardiomyopathy in a stillborn
 Poliovirus • Siegel and Goldberg, 1955 --- pregnant women were more susceptible and")
2) Poliovirus • Siegel and Goldberg, 1955 --- pregnant women were more susceptible and higher death rate • Inactivated subcutaneous polio vaccine is recommend for susceptible pregnant women who travel to endemic area • Harjulehto, 1989 --- live oral polio vaccine without harmful fetal effects

5. Parvovirus Human B 19 parvovirus causes erythema infectiosum, or fifth disease Single-stranded DNA virus replication in rapidly proliferating cells transient aplastic crisis in Pts with hemolytic anemia specific Ig. M Ab Brown, 1994 --- B 19 parvovirus is tropic for erythroid cells only persons with P antigen are susceptible Maternal hydrops syndrome --- preeclampsia-like disease related to large placenta mass in 25 weeks pregnancy with fetal hydrops ( Ville, 1995 )

• Rogers, 1993 --- spontaneous abortion 2/80 • Tiessen, 1994 --- congenital anomalies • Radis, 1990 --- fetal loss rate 5% in 39 infected women • Wright, 1994 --- early fetal death is not associated with hydropic change but is common in fetal dying after mid-pregnancy • positive serology, USG > hydrops > fetal transfusion ( Peters, 1990 ; Thorp, 1994 )
 maternal rubella-- congenital malformations Minor import in")
6. Rubella Gregg, 1941, 호주의 안과의사 (1942) maternal rubella-- congenital malformations Minor import in absence of pregnancy, but pregnant wastage and severe congenital anomalies in pregnancy postpartum of fetuses with rubella infection compared with congenital rubella syndrome < 12주 : 80% 12 - 16주 : 25% > 16주 : congenital defect are rare.

Fig 58 -2
 • CIx : febrile illness")
• Live attenuated virus vaccination (15 -18 yrs) • CIx : febrile illness immunosuppression before or during pregnancy(90 days) allergy to neomycin • Immunized women within 3 months of conception have no evidence that vaccine induces malformations. • Specific Ig M Ab • serial sampling 에서 4배 이상 증가하는 Ig G for 2 -3 weeks • amniocentesis, cordocentesis, CVS

fig

Congenital rubella syndrome : includes one or more of following 1. Eye lesion. Including cataracts, glaucoma, microphthalmia, other anormalies 2. Heart disease. Including PDA, septal defects, pulmonary artery stenosis 3. Sensorineural deafness 4. CNS defects including meningoencephalitis 5. Retarded fetal growth 6. Thrombocytopenia and anemia 7. Hepatitis, hepatosplenomegaly, jaundice 8. Chronic diffuse interstitial pneumonitis 9. Osseous changes 10. Chromosomal abnormalities

Extended rubella syndrome --- Asymptomatic infants 1/3 second or third decade of life type I DM progressive panencephalitis Infants born with congenital rubella may shed the virus for many months and threat to other infants or susceptible adults. No therapy Ig effects are controversy

7. Cytomegalovirus • DNA herpesvirus • most common cause of perinatal infection • primary infection, periodic reactivation with viral shedding • Yow and Demmler, 1992 20 yrs, 50000 newborn many have died and most of the survivors have severe handicaps ; mental retardation, blindness, deafness • Pregnancy not increase the risk or severity

Asymptomatic but 15% fever Fowler, 1992 susceptible women 1 -4% transmitted to fetus 40% cytomegalic inclusion disease 10% Maternal immunity does not prevent recurrence nor congenital infection.

Cytomegalic inclusion disease = Congenital CMV infection 1. Low birth weight 2. Intracranial calcification 3. Microcephaly 4. Chorioretinitis 5. Mental and motor retardation 6. Sensorineural deficits 7. Hepatosplenomegaly 8. Jaundise 9. Hemolytic anemia 10. Thrombocytopenic purpura

specific Ig M Ig G titer 4배 이상 증가 Amniocentesis, Cordocentesis Sono, CT, MRI --- ventriculomegaly cerebral calcification microcephaly fetal hyperechoic bowel No therapy, No vaccine

II. Bacterial infections. 1. Group B streptococcus • group B -hemolytic streptococcus is common in women in vagina and rectum • Regan, 1991 15 -20% of 8000 pregnant women had a low genital tract culture positive • Preterm labor, PROM, chorioamnionitis, puerperal sepsis, fetal infection, postpartum osteomyelitis and mastitis

Neonatal sepsis Early onset disease : within 6 -12 hours of birth respiratory distress, shock, apnea mortality : 25% neurological sequelae Late onset disease : a week or more after birth serotype III organism meningitis : most common neurological sequelae

Steigman, 1978 Pc G 50000 U IM at birth as prophylaxis ACOG, 1996 ; CDC, 1996 1) Screening-based approach--- 35 -37 weeks routine culture (+) intrapartum Pc. G IM 2) Risk-factor approch Risk factor : 1. preterm labor 2. p. PROM 3. Prolonged ROM > 18 hrs 4. Sibling affected by symptomatic group B streptococcal infection 5. Intrapartum maternal fever
 aerobic motile bacillus • Food-borne transmission")
2. Listeriosis • Listeria monocytogenes : gram (+) aerobic motile bacillus • Food-borne transmission : cabbage, milk, cheese • Asymptomatic, febrile illness stimulate labor ( Yonekra, 1986 ) meconium passage in fetal infection disseminated granulomatous lesion with microabscesses ( Topalovski, 1993 )

Motality 50 % in neonatal infection Dx : blood culture Combination of ampicillin and gentamicin Maternal antimicrobial treatment may be effective for fetal infection. ( Linnan, 1988 )
 Salmonellosis • Major cause of food-borne illness •")
3. Salmonella and Shigella infection 1) Salmonellosis • Major cause of food-borne illness • Diarrhea, abdominal pain, fever, chill, N/V • IV fluid hydration Typhoid fever • salmonella typhi • Dily, 1990 abortion, preterm labor ( 80% ) fetal mortality (60%) maternal mortality (20%) • chloramphenicol • Antityphoid vaccine --- no harmful effect
 Shigellosis • Blood stool-diarrhea • Abdominal cramping, tenesmus, fever • Self-limited • careful")
2) Shigellosis • Blood stool-diarrhea • Abdominal cramping, tenesmus, fever • Self-limited • careful attention of dehydration • Bactrim

III. Protozoal infections 1. Toxoplasmosis • Toxoplasma gondii • infected raw or undercooked meat contact with oocytes in infected cat feces • Transplacental transfer --- 모체감염이 있는 경우에만 congenital infection • Wong and Remington, 1994 risk of fetal infection : 50% 1 st trimester : 10% 2 nd trimester : 60%

• Low birth weight, anemia, hepatosplenomegaly, icterus, neurologic impairment, mental retardation, intercranial calcification, hydrocephaly, microcephaly, chorioretinitis • Ig G titer 4배 이상 증가 • Ig M : recent infection • Spiramycin --- 3 g/day

2. Malaria • Plasmodium ; vivax, ovale, malariae, falciparum • fever, chill, headache, myalgia, hemolytic anemia, jaundice • renal failure ( black water syndrome ), coma, death • Abortion, preterm labor, fetal death • Involve the placenta without affecting fetus • ( Jones, 1950 ) • Antimalarial drugs are not contraindicated during pregnancy • 치료 : Chloroquine, quinidine, mefloquine • Prophylaxis : chloquine 300 g/week P. O. • Mefloquine, doxycycline is contraindication during pregnancy
substance abuse 2)human immunodeficiency virus")
1. Syphilis A. continued prevalence of syphilis at delivery 1)substance abuse 2)human immunodeficiency virus infection 3)lack of prenatal care 4)treatment failure and reinfectlon
cervical chancre, condy. Ioma lata. 2)fetal death. congenital syphilis")
1. Syphilis B. Clinical manifestation 1)cervical chancre, condy. Ioma lata. 2)fetal death. congenital syphilis 3)large and pa 1 e p 1 acenta; decreased in the number of blood vessel
VDRL or RPR test at the first prenatal care 2)PCR")
1. Syphilis C. Diagnosis 1)VDRL or RPR test at the first prenatal care 2)PCR for detection of T. pallidum in amniotic fluid-100% specific 3)hepatosplenomegaly, edema, ascites, and hydrops in fetus 4)jaundice with petechiae or purpuric skin lesion, Lymphadenopathy, snuffles Pneumonia, myocarditis and nephrosis in neonate

1. Syphilis D. Treatment; to eradicate maternal infection as well as to prevent congenital syphilis (2% tx failure) 1) penicilllin; treatment of choice Benzathine penicillin G, 240만 units IM 1 wk second dose (1년이상된 syphilis or neurosyphilis; 1주간격으로 3번 IM) 2) erythromycin; may be curative in the mother but my not prevent congenital syphillis 3) clinical stigma despite recommended treatment during pregnancy; 20% of newborn 4) counseling and testing for antibody to human immunodeficiency virus 5) maternal serological tlter follow up monthly 6) congenital syphilis; CSF examination, monthly follow up until negative test
latent syphillis of more than 1 -year duration")
1. Syphilis • E. Lumbar puncture 1)latent syphillis of more than 1 -year duration 2)any neuo. Iogical symptoms or treatment failure 3)sero. Iogical titer of 1: 32 or higher 4)nonpenicillin therapy is planned 5)concomitant humanimmunodeficiency viral infection

A B A: chancroid ulcer B: Treponema pallidum identified using species-specific fluoroscein-conjugated monoclonal antibody

A B A: primary syphilitic chancre of the cervix B: primary chancre of the tongue

A B A: secondary syphilitic rash of the palm and sole B: secondary syphilitic rash of palm

A B A: pustular and macular lesions in secondary syphilis B: psoriasiform secondary syphilis

A B A: perivulvar and perianal condyloma latum in secondary syphilis B: mucus patches involving the tongue in secondary syphilis

A B A: congenital syphilis “snuffles” crusting and purulent nasal discharge B: diffuse diskoid lesion
 concomitant chlamydia 1 infection (about 40%) 2) limited to the lower")
2. Gonorrhea 1) concomitant chlamydia 1 infection (about 40%) 2) limited to the lower genital tract but developed salpingitis before 12 weeks 3) spontaneous abortion. preterm de. Iivery, prematurely ruptured membrane, chorioamnionitis, and postpartum infectlion、 4) screening test at the first prenatal visit and repeat culture after 28 weeks in high risk population 5) ceftriaxone, spectinomycin, and erythromycin
 a. Itered sexual practices. Cultural customs 2) engorged")
• Disseminated gonococcal infection 1) a. Itered sexual practices. Cultural customs 2) engorged pe. Ivic vasculature 3) altered immunostatus of pregnancy prophylaxis against eye infection; ceftriaxone 25 to 50 mg/kg IV or IM as a single dose not appropriate topical antibiotic preparation

A A: gonococcal urethritis Gram-negative intracellular diplococci B B: non-gonococcal urethritis absence of Gram-negative diplococci

A A: Neisseria gonorrheae microscopic feature note gram-negative diplococci B B: Neonatal gonococcal conjunctivitis note profuse purulent exudate
lymphogranuloma venereum, urethritis, mucopuru 1 ent cervicitis, and acute salpingitis")
3. chlamydial Infection • 1)lymphogranuloma venereum, urethritis, mucopuru 1 ent cervicitis, and acute salpingitis 2)asymptomatic infection but perinatal transmission; neonatal conjunctivitls a nd pneumonia

A B Chlamydia trachomatis infection A: mucopurulent cervicitis, note pus mixed with mucus B: before and after treatment with doxycycline
recent chlamydia| infection with anti-chlamydia Ig. M antibody positive; preterm")
3. chlamydial Infection • 3)recent chlamydia| infection with anti-chlamydia Ig. M antibody positive; preterm labor prematurely ruptured membranes 4)screenig test with DNA probe and polymerase chain reaction ; cheaper and quicker 5)erythromycin, azithromycin ; category B
 type 1(nongenital infection) type 2(genital infection) 2)primary infection; 50%of")
4. Herpes simplex virus 1) type 1(nongenital infection) type 2(genital infection) 2)primary infection; 50%of risk in neonatal infectlon recurrent infection; fewer in number, less tender and shorter period and on 1 y 4 to 5% of risk
tissue culture, Tzanck smear. and PCR 4)acyclovir; topica. I")
4. Herpes simplex virus • 3)tissue culture, Tzanck smear. and PCR 4)acyclovir; topica. I 1 y used, ora. I preparation-not been clear. Iy estabilished A. Neonatal disease; across the placenta 1)disseminated, with involvement of major viscera 2)localized; central nervous system, eyes. skin, or mucosa 3)asymptomatic
")
A B Primary HSV lesion A: cervical mucus is clear, not purulent, small vesicle(allow) B: severe HSV-2 cervicitis

Primary genital herpes of the vulva neonatal HSV infection ulcers and cruste lesions on the buttocks
asymptomatic recurrences are more common than detected")
4. Herpes simplex virus • Antepartum management 1)asymptomatic recurrences are more common than detected recurrent infection 2)cesarean delivery ; primary or recurrent lesion are visualized near the time 3) No lesion, no cesarean
 1) prevalence among the childbearing women ; 1 to")
5. Acquired immunodeficiency syndrome (AIDS) 1) prevalence among the childbearing women ; 1 to 2 per 1000 in 1994 2) CD 4 surface antigen-receptor for virus- shortening cell life by infection drops the number of T cell-imunosuppression
 • 3)incubation period; 2 to 3 months asymptomatic viremic")
5. Acquired immunodeficiency syndrome (AIDS) • 3)incubation period; 2 to 3 months asymptomatic viremic period; l 0 years dlagnosed AIDS; other opportunistic infection. CD 4 count of less than 200/ul dying within 2 years 4)ELISA; screening test, sensitivity of over 99. 5% Western b!ot; highly specific, but false negative result due to more antibody is required immunoflurescence assay, PCR, viral culture
 A. Maternal and fetus-infant infection 1)the rate of perinatal")
5. Acquired immunodeficiency syndrome (AIDS) A. Maternal and fetus-infant infection 1)the rate of perinatal transmission of Hl. V ; 13 to 40% 2)risk factors ; maternal p 24 antigenemia, CD 4+ count Iess than 700/ul, 3)transp|acenta|infection or contracted at birth 4)membrane rupture for more than four hour ; 14 to 25% increased Vertica. I transmission breast feeding; 10 to 20% increased de 1 ivery before 34 weeks; four times more common
 B Prevention of transmission 1)the health-care workers ; appropriated")
5. Acquired immunodeficiency syndrome (AIDS) B Prevention of transmission 1)the health-care workers ; appropriated barries percautions and if exposed ; zidovudine prophy. Iaxsis 2)antivral therapy ; decreased perinatal transmission but less clear 3)Cesarean section ; decreased perinatal transmission but less clear 4)breast feeding ; not recommanded in HIV positive women 5)combination of nucleoside analogue with protease inhibitor

A B A: cervicovaginal candidiasis note the white nonhomogeneous curd-like, clumped exudate B: trichomonal vaginitis and ectocervicitis “strawberry cervix” showing petechiae on the ectocervix C: profuse purulent vaginal discharge due to trichomoniasis color is yellow when viewed on a white swab C
human papinomavirus type 6 and 11 2)condylomata acuminata; increased in number")
6. Human papillomavirus 1)human papinomavirus type 6 and 11 2)condylomata acuminata; increased in number and size during pregnancy and difficult to perform vaginal delivery or episiotomy 3)laryngea| papillomatosis in children ; type 6. 11 - aspiration infected material at de. Iivery
drying of the external genitalia; inhibit pro. Iiferation of the warts")
6. Human papillomavirus 4)drying of the external genitalia; inhibit pro. Iiferation of the warts trichloroacetic acid: topicaly applied 1 -3 times weekly cryotherapy, laser ablation podophy. Ilin resin, 5 -FU cream, interferon ; should not be used in pregnancy
- Slides: 138