Diabetes Dr Isazadehfar Assistant Professor of Community and

Diabetes Dr. Isazadehfar Assistant Professor of Community and Preventive Medicine
 is a group of diseases characterized by high")
What is diabetes? Diabetes mellitus (DM) is a group of diseases characterized by high levels of blood glucose resulting from defects in insulin production, insulin action, or both. The term diabetes mellitus describes a metabolic disorder of multiple aetiology characterized by chronic hyperglycaemia with disturbances of carbohydrate, fat and protein metabolism The effects of diabetes mellitus include long–term damage, dysfunction and failure of various organs

Carbohydrate Digestion

Diabetes mellitus may present with characteristic symptoms such as thirst, polyuria, blurring of vision, and weight loss. In its most severe forms, ketoacidosis or a non–ketotic hyperosmolar state may develop and lead to stupor, coma and, in absence of effective treatment, death. Often symptoms are not severe, or may be absent, and consequently hyperglycaemia sufficient to cause pathological and functional changes may be present for a long time before the diagnosis is made.

Diabetes Long-term Effects Retinopathy with potential blindness Nephropathy→ renal failure Neuropathy → foot ulcers amputation Charcot joints autonomic dysfunction Cardiovascular disease Peripheral vascular disease Cerebrovascular disease

Types of Diabetes ¡ Type 1 Diabetes Mellitus ¡ Type 2 Diabetes Mellitus ¡ Gestational Diabetes ¡ Other types: v MODY (maturity-onset diabetes of youth) v Secondary Diabetes Mellitus
 or juvenile-onset diabetes. Account for 5% to")
Type 1 diabetes Insulin-dependent diabetes mellitus (IDDM) or juvenile-onset diabetes. Account for 5% to 10% of all cases of diabetes develops when the body’s immune system destroys pancreatic beta cells usually strikes children and young adults, although disease onset can occur at any age Risk factors may include: autoimmune, genetic, and environmental factors

Type I Diabetes Low or absent endogenous insulin ¡ Dependent on exogenous insulin for life ¡ Onset generally < 30 years ¡ Onset sudden ¡ l Symptoms: 3 P’s: polyuria, polydypsia, polyphagia

Type I Diabetes Cell
 or adultonset diabetes account for about 90%")
Type 2 diabetes non-insulin-dependent diabetes mellitus (NIDDM) or adultonset diabetes account for about 90% to 95% of all cases of diabetes It usually begins as insulin resistance, a disorder in which the cells do not use insulin properly. As the need for insulin rises, the pancreas gradually loses its ability to produce insulin. is associated with older age, obesity, family history of diabetes, history of gestational diabetes, impaired glucose metabolism, physical inactivity, and race/ethnicity African Americans, Hispanic/Latino Americans, American Indians, and some Asian Americans and Native Hawaiians or Other Pacific Islanders are at particularly high risk for type 2

Type II Diabetes ¡ Insulin levels may be normal, elevated or depressed l l l ¡ Characterized by insulin resistance diminished tissue sensitivity to insulin impaired beta cell function (delayed or inadequate insulin release) Often occurs >40 years

Type II Diabetes

Type II Diabetes Risk factors: family history, sedentary lifestyle, obesity and aging ¡ Controlled by weight loss, oral hypoglycemic agents and or insulin ¡

Gestational diabetes A form of glucose intolerance that is diagnosed in some women during pregnancy More frequently among African Americans, Hispanic/Latino Americans, and American Indians. It is also more common among obese women and women with a family history of diabetes During pregnancy, gestational diabetes requires treatment to normalize maternal blood glucose levels to avoid complications in the infant After pregnancy, 5% to 10% of women with gestational diabetes are found to have type 2 diabetes Women who have had gestational diabetes have a 20% to 50% chance of developing diabetes in the next 5 -10 years

Other types of DM ¡ Other specific types of diabetes result from specific genetic conditions (such as maturityonset diabetes of youth), surgery, drugs, malnutrition, infections, and other illnesses ¡ Such types of diabetes may account for 1% to 5% of all diagnosed cases of diabetes

Secondary DM Secondary causes of Diabetes mellitus include: Acromegaly Cushing syndrome Thyrotoxicosis Pheochromocytoma Chronic pancreatitis Cancer

Drug induced hyperglycaemia: ◦ ◦ ◦ Atypical Antipsychotics Beta-blockers → Inhibit insulin secretion Calcium Channel Blockers → Inhibits secretion of insulin Corticosteroids → Cause peripheral insulin resistance and gluconeogensis Fluoroquinolones - Inhibits insulin secretion Niacin → increased insulin resistance

◦ ◦ ◦ Phenothiazine → Inhibit insulin secretion Protease Inhibitors → Inhibit the conversion of proinsulin to insulin Thiazide Diuretics → Inhibit insulin secretion due to hypokalaemia

What goes wrong in diabetes? ¡ Multitude of mechanisms l Insulin Regulation ¡ Secretion ¡ Uptake or breakdown ¡ l Beta cells ¡ damage

Action of Insulin on the Cell Metabolism

Action of Insulin on Carbohydrate, Protein and Fat Metabolism ¡ Carbohydrate Facilitates the transport of glucose into muscle and adipose cells ¡ Facilitates the conversion of glucose to glycogen for storage in the liver and muscle. ¡ Decreases the breakdown and release of glucose from glycogen by the liver ¡

Action of Insulin on Carbohydrate, Protein and Fat Metabolism ¡ Protein Stimulates protein synthesis ¡ Inhibits protein breakdown; diminishes gluconeogenesis ¡

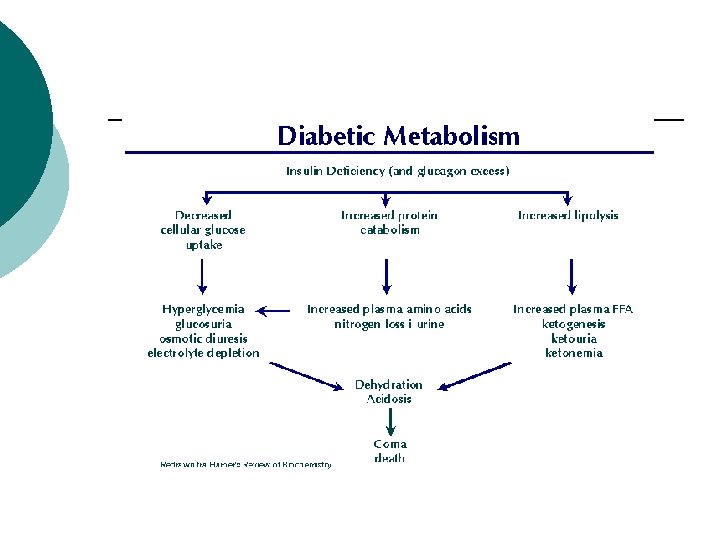
Action of Insulin on Carbohydrate, Protein and Fat Metabolism ¡ Fat Stimulates lipogenesis - the transport of triglycerides to adipose tissue ¡ Inhibits lipolysis – prevents excessive production of ketones or ketoacidosis ¡

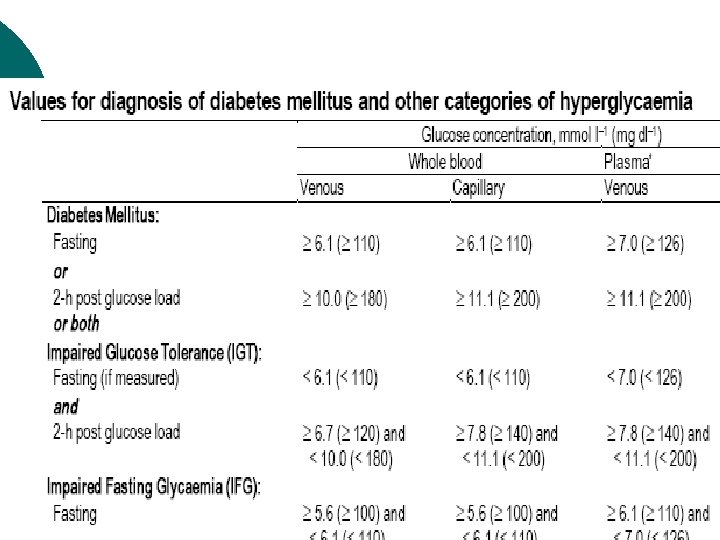
Screening for Diabetes Fasting Blood Glucose Significance Action <110 Normal Retest in 3 years >110 & <126 IGT 1. Additional Testing 2. Check risk factors 3. MNT >126 Diabetes likely 1. Confirm by 2 nd FBG 2. Treat DM

Management of DM ¡ The major components of the treatment of diabetes are: A • Diet and Exercise B • Oral hypoglycaemic therapy C • Insulin Therapy

A. Diet is a basic part of management in every case. Treatment cannot be effective unless adequate attention is given to ensuring appropriate nutrition. Dietary treatment should aim at: ◦ ◦ Ensuring weight control Providing nutritional requirements Allowing good glycaemic control with blood glucose levels as close to normal as possible Correcting any associated blood lipid abnormalities
 The following principles are recommended as dietary guidelines for people")
A. Diet (cont. ) The following principles are recommended as dietary guidelines for people with diabetes: Dietary fat should provide 20 -30% of total intake of calories but saturated fat intake should not exceed 10% of total energy. Cholesterol consumption should be restricted and limited to 300 mg or less daily. Protein intake can range between 10 -20% total energy (0. 8 -1 g/kg of desirable body weight). Requirements increase for children and during pregnancy. Protein should be derived from both animal and vegetable sources. Carbohydrates provide 50 -60% of total caloric content of the diet. Carbohydrates should be complex and high in fibre. Excessive salt intake is to be avoided. It should be particularly restricted in people with hypertension and those with nephropathy.

Exercise Physical activity promotes weight reduction and improves insulin sensitivity, thus lowering blood glucose levels. Together with dietary treatment, a programme of regular physical activity and exercise should be considered for each person. Such a programme must be tailored to the individual’s health status and fitness. People should, however, be educated about the potential risk of hypoglycaemia and how to avoid it.

Management of Diabetes Mellitus ¡ Nutrition ¡ Blood glucose ¡ Medications ¡ Physical activity/exercise ¡ Behavior modification

Medical Nutrition Therapy Maintain short and long term body weight ¡ Reach and maintain normal growth and development ¡ Prevent or treat complications ¡ Improve and maintain nutritional status ¡ Provide optimal nutrition for pregnancy ¡

Nutritional Management for Type I Diabetes ¡ Consistency and timing of meals ¡ Timing of insulin ¡ Monitor blood glucose regularly

Nutritional Management for Type II Diabetes Weight loss ¡ Smaller meals and snacks ¡ Physical activity ¡ Monitor blood glucose and medications ¡

Diabetes Control and Complications Trial ¡ Conventional l 1 - 2 insulin injections, self monitoring B. G routine contact with MD and case manager 4 X/year. ¡ Intensive l l therapy: 3 or more insulin injections, with adjustments in dose according to B. G monitoring, planned dietary intake and anticipated exercise.

Diabetes Control and Complications Trial ¡ Results: l l ¡ 76% 60% 54% 39% reduction in in retinopathy neuropathy albuminuria microalbuminuria Implication: Improved blood glucose control also applies to person with type II diabetes.

Nutrition Recommendations ¡ Carbohydrate l ¡ 60 -70% calories from carbohydrates and monounsaturated fats Protein l 10 -20% total calories

Nutrition Recommendations ¡ Fat l l l ¡ <10% calories from saturated fat 10% calories from PUFA <300 mg cholesterol Fiber l 20 -35 grams/day

B. Oral Anti-Diabetic Agents There are currently four classes of oral antidiabetic agents: i. Biguanides ii. Insulin Secretagogues – Sulphonylureas iii. Insulin Secretagogues – Non-sulphonylureas iv. α-glucosidase inhibitors v. Thiazolidinedione (TZDs) ¡

B. 2 Combination Oral Agents Combination oral agents is indicated in: ¡ Newly diagnosed symptomatic patients with Hb. A 1 c >10 ¡ Patients who are not reaching targets after 3 months on monotherapy

Different Diabetes Complications Macro vascular ¡ Micro vascular ¡ Neuropathy ¡ Infections ¡

Macro vascular Complications

Macro-vascular Complications ¡ ¡ ¡ Ischemic heart disease Cerebrovascular disease Peripheral vascular disease Diabetic patients have a 2 to 6 times higher risk for development of these complications than the general population

Macro-vascular Complications The major cardiovascular risk factors in the nondiabetic population (smoking, hypertension and hyperlipidemia) also operate in diabetes, but the risks are enhanced in the presence of diabetes. Overall life expectancy in diabetic patients is 7 to 10 years shorter than non-diabetic people.

Hypertension in Type 1 and 2 Diabetes Type 1 Develop after several years of DM Ultimately affects ~30% of patients Type 2 Mostly present at diagnosis Affects at least 60% of patients

Goals of Treatment of Hypertension Lower target for diabetic patients than nondiabetic patients: 130/85 vs. 140/90

Dyslipidaemia in DM Most common abnormality is HDL and Triglyserides ¡ A low HDL is the most constant predictor of CV disease in DM ¡ Target lipid values: LDL <2. 6 mmol/l, HDL >1. 15 mmol/l, TG < 2. 5 mmol/l ¡

Micro vascular Complications

Eye Complications ¡ v v Cataracts Non enzymatic glycation of lens protein and subsequent cross linking Sorbitol accumulation could also lead to osmotic swelling of the lens but evidence of involvement in cataract formation is less strong
: - Background - Pre-proliferative - Proliferative - Advanced diabetic eye")
Eye Complications Retinopathy (stages): - Background - Pre-proliferative - Proliferative - Advanced diabetic eye disease - Maculopathy ¡ Glaucoma ¡

Background Retinopathy ¡ ¡ ¡ Micro aneurisms Scattered exudates Hemorrhages (flame shaped, Dot and Blot) Cotton wool spots (<5) Venous dilatations Background retinopathy
 Fibrous proliferation (on disc,")
Proliferative Retinopathy ¡ ¡ ¡ New vessels (on disc, elsewhere) Fibrous proliferation (on disc, elsewhere) Hemorrhages (preretinal, vitreous) Panretinal photo-coagulation
 Diabetes has become the most common cause of end stage renal")
Diabetic Nephropathy (DN) Diabetes has become the most common cause of end stage renal failure in the US and Europe ¡ About 20 – 30% of patients with diabetes develop evidence of nephropathy ¡ The prevalence of DN is higher in Black Americans than in Whites (Figures for South Africa is not available) ¡

Stages of DN Stage I glomerular filtration and kidney hypertrophy Stage II u-albumin excretion < 30 mg/24 h Stage III Microalbuminuria (30 – 300 mg/24 h)
 Stage IV Overt nephropathy (> 300 mg/24 h, positive u")
Stages of DN (cont) Stage IV Overt nephropathy (> 300 mg/24 h, positive u dipstick) Stage V ESRD characterized by blood urea and creatinine levels, hyperkalaemia and fluid overload
 Autonomic neuropathy Mononeuropathy Proximal motor neuropathy")
Diabetic Neuropathy Sensorimotor neuropathy (acute/chronic) Autonomic neuropathy Mononeuropathy Proximal motor neuropathy

Specific Infections ¡ ¡ ¡ Community acquired pneumonia Acute bacterial cystitis Acute pyelonephritis Emphysematous pyelonephritis Perinephric abscess Fungal cystitis ¡ ¡ Necrotizing fasciitis Invasive otitis externa Rhinocerebral mucormycosis Emphysematous cholecystitis

Self-Care Patients should be educated to practice self-care. This allows the patient to assume responsibility and control of his / her own diabetes management. Self-care should include: ◦ ◦ ◦ ◦ Blood glucose monitoring Body weight monitoring Foot-care Personal hygiene Healthy lifestyle/diet or physical activity Identify targets for control Stopping smoking
- Slides: 61