Diabetes complicating pregnancy Challenges in diagnosis and therapyof

Diabetes complicating pregnancy: Challenges in diagnosis and therapyof import to the Neonatologist Robert S. Egerman, MD, FACOG Professor Obstetrics & Gynecology, Maternal Fetal Medicine, General Internal Medicine

Financial Disclosures • None

Objectives: • Recognize the challenges of diagnosing and treating gestational diabetes • Compare various therapies for gestational diabetes and their neonatal effects • Evaluate the utility and hazards of supplemental progesterone for the prevention of preterm birth

Objectives: g in h t e • Recognize the challenges of diagnosing and treating gestational m diabetes o s s i t h t e • Compare various therapies for gestational diabetes and their g f o neonatal effects m t e u h o t • Evaluate the utility and hazards of supplemental progesterone for the l e u f v prevention of preterm birth g a n H ani e m

Type 2 Diabetes • Florida • 2. 4 million or 13% have diabetes • 0. 58 million don’t know they have it • 5. 8 million have prediabetes ADA 2018

Diabetes • • • 2 to 4 fold increased risk for MI or stroke Leading cause of blindness Leading cause of ESRD Leading cause of non traumatic amputation $176 billion direct medical costs for 2012 ADA CDC NKF

Diabetes • • • 2 to 4 fold increased risk for MI or stroke Leading cause of blindness Leading cause of ESRD Leading cause of non traumatic amputation $245 Billion direct medical costs for 2012 ADA CDC NKF

Ratner, J Clin Endocrinol Metab, 2008

3234 patients, Prediabetes, 2/3 female 1. Control 2. Metformin 850 mg bid 3. Lifestyle 7% weight reduction, 150 min exercise weekly

- 31% - 58% DPP Research Group, N Engl J Med 2002

1 5 Years since DPP 10 DPP Research Group, Lancet 2009

Ratner, J Clin Endocrinol Metab, 2008

Insulin and Incretins Glucagon Glucose Insulin

Insulin and Incretins Glucagon Glucose Insulin

Insulin and Incretins GIP Glucagon Glucose GLP Glucose Insulin

Insulin and Incretins GLYBURIDE GIP Glucagon Glucose GLP METFORMIN Glucose Insulin INSULIN

Insulin and Incretins GLYBURIDE GIP Glucagon Glucose GLP METFORMIN Glucose Insulin THIAZOLINEDIONE INSULIN

Insulin and Incretins GLYBURIDE GIP Glucagon Glucose GLP METFORMIN Glucose Insulin THIAZOLINEDIONE INSULIN DPP-4 Inhibitors-liptins GLP-1 Recept Agonists- tides

Insulin and Incretins GLYBURIDE GIP Glucagon Glucose GLP METFORMIN Glucose Insulin THIAZOLINEDIONE INSULIN DPP-4 Inhibitors-liptins GLP-1 Recept Agonists- tides SGLT-2 Inhibitors- gliflozin

Insulin and Incretins GLYBURIDE GIP Glucagon Glucose Amylin analog-lintide GLP METFORMIN Glucose Insulin THIAZOLINEDIONE INSULIN DPP-4 Inhibitors-liptins GLP-1 Recept Agonists- tides SGLT-2 Inhibitors- gliflozin

Case • A NICU consultation is sought for a 26 yo P 0101 at 32 weeks presents with preterm labor • Her pregnancy is complicated by A 2 gestational diabetes treated with glyburide as well as a shortened cervical length [at 21 weeks gestation] managed with 17 OHP • She had a prior spontaneous onset of labor and delivery at 35 weeks • She is normotensive, her BMI is 40 kg/m 2 and her accucheck is 168 mg/d. L. Cervix is 4 cm dilated and EFW is 2410 grams or 96% • The parents ask you how do we get the best neonatal outcome?

Metabolic changes pertinent to pregnancy Peripheral insulin resistance Decreased glucose disposal

Progesterone h. CS Adipokines Diet Microbiome Weight B cell dsyfunction Gestational diabetes

Maternal Risks • Cesarean section • Macrosomic infant, birth trauma • Shoulder dystocia • Preeclampsia • Ketosis • Type 2 diabetes

Longer term complications • • National Collaborative Perinatal Project 28, 358 mother infant pairs, 484 gest DM Followed for 7 years of age Larger BMI of child ages 4 & 7; controlled for – Birth weight – Maternal BMI – Race – Socioeconomic status • Children of mothers with gestational diabetes had a 61% increased risk for being overweight Baptiste-Roberts, Matern Child Health J 2012
 2/4 C & C (100 gm) 2/4 HAPO")
Diagnosing gestational diabetes NDDG (100 gm) 2/4 C & C (100 gm) 2/4 HAPO (75 gm) 1/3 Fasting 105 95 92 1 hour 190 180 2 hour 165 153 3 hour 145 140

Diagnosing gestational diabetes
")
NHANES III Retinopathy (%)
")
NHANES III Retinopathy (%)

Diagnosing gestational diabetes ? ?

Diagnosing gestational diabetes Sample time FPG 1 -h PG 2 -h PG OR 1. 5 1. 75 2. 0 90 167 142 92 180 153 95 191 162 Coustan, Am J Obstet Gynecol 2010

The debate Professor Gerard H. A. Visser Utrecht, The Netherlands “ Tell me how many [gestational diabetes patients] you want, and I will give you the formula. ”

Criteria for diagnosis • ACOG 2 step approach • 471 records 5. 5% Gestational Diabetes • IADPSG 1 step approach • 332 records 16% Gestational Diabetes • No differences in perinatal outcomes Ogunleye, J Matern Fetal Neonatal Med 2016

Criteria for diagnosis Ogunleye, J Matern Fetal Neonatal Med 2016

Criteria for diagnosis Ogunleye, J Matern Fetal Neonatal Med 2016

Criteria for diagnosis Feldman, Obstet Gynecol 2016

Criteria for diagnosis Feldman, Obstet Gynecol 2016


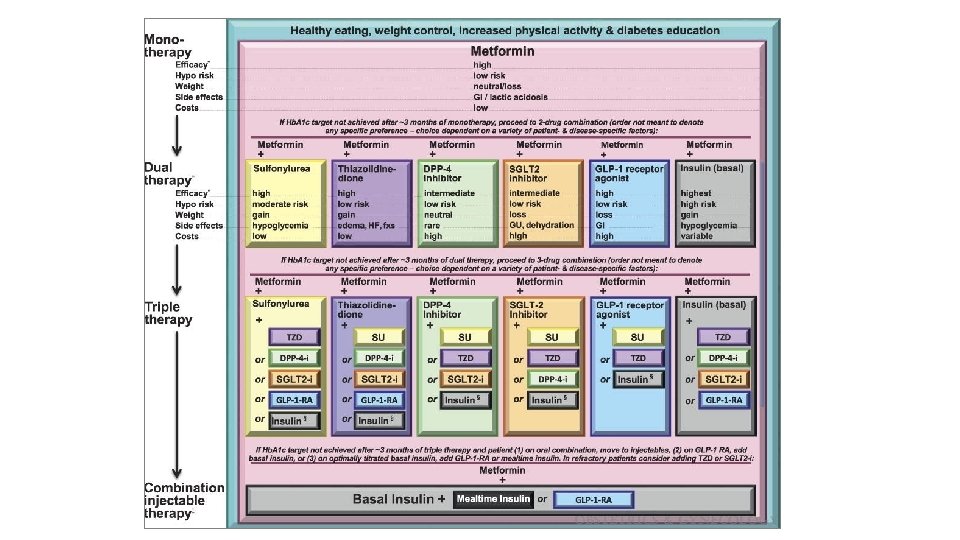
Hypoglycemics

Hypoglycemics Langer, N Engl J Med 2000

Hypoglycemics Langer, N Engl J Med 2000

Hypoglycemics 4982 4191 Castillo, JAMA Pediatr 2015

Hypoglycemics 4982 Worse control with Glyburide? 4191 Castillo, JAMA Pediatr 2015

Hypoglycemics Rowan, N Engl J Med 2008

Cochrane 2017

Cochrane 2017



Preterm birth prevention • Who is at risk? • Prior preterm birth • Shortened cervical length during current pregnancy • What can we do for prevention? • 17 OH Progesterone [250 mg IM weekly 16 -36 wks] • Vaginal progesterone [90, 100, 200 mg nightly]

Progesterone

Progesterone Glucagon Glucose Progesterone Insulin

Progesterone • 17 a hydroxyprogesterone caproate and Gestational Diabetes • Singletons • Treated n = 557 Gest DM 12. 9% versus 4. 9% • Obese n = 140 • Overweight and obese independent risks • More B mimetics in control group 25% versus 18% (favors control for diabetes) Rebarber, Diabetes Care 2007

Progesterone • 17 a hydroxyprogesterone caproate and Gestational Diabetes • Singletons • Treated n = 293 Gest DM 5. 8 versus 4. 7% Twins • Treated n = 323 Gest DM 7. 4 versus 7. 6% • Obesity independent risk for Gest Diabetes Gyamfi, Am J Obstet Gynecol 2009

Progesterone • 17 a hydroxyprogesterone caproate and Gestational Diabetes • Singletons • Treated n = 110 Gest DM 10. 9 versus 3. 6% • Obese n = 42 • BMI not an independent risk for Gest DM Waters, Obstet Gynecol 2009

Progesterone • 17 a hydroxyprogesterone caproate and Gestational Diabetes • Singletons • Treated n = 491 Gest DM 13. 8% versus 9. 6% • Obese n = 491 Egerman, J Obesity 2014

Progesterone- so does it work?

Progesterone

Progesterone • Neonatal outcomes after exposure to 17 OH P versus unexposed • No differences in low birth weight, macrosomia, respiratory complications, jaundice, hypoglycemia Delivery age weeks 17 OH P None 32 -33. 9 221 451 34 -35. 6 698 1314 36 -37. 9 1797 3554 38 -41 1709 3836 Ramsey, unpublished

Summary • Maternal glucose control is necessary • The optimal agent is unclear • Glyburide is less preferred than insulin or metformin • Long term metabolic effects on offspring may be concerning • The efficacy of 17 OH progesterone is unclear • There may be a trade off with maternal dysmetabolism and efforts to prevent preterm delivery when using progesterone
- Slides: 62