Diabetes By Sophie Lewis Classification Diabetes Mellulitus DM

Diabetes By Sophie Lewis
 – A syndrome of chronic hyperglycaemia due to relative")
Classification • Diabetes Mellulitus (DM) – A syndrome of chronic hyperglycaemia due to relative insulin deficiency, resistance or both • Diabetes Inspidus (DI) – a condition characterized by excessive thirst and excretion of large amounts of severally dilute urine – 2 common types Central deficiency in ADH and nephrogenic diabetes insipidus caused by insensitivity of the kidneys to ADH

Epidemiology DM affects more than 120 million people worldwide

Anatomy Retroperitoneal organ originating from the foregut Divided into the: • Head • Neck • Body • Tail Blood Supply • Splenic +Hepatoduodenal arteries • Portal + Splenic veins Endocrine gland (islets of Langerhans) • α-glucagon • Β-insulin • δ-somatostatin Exocrine glanddigestive enzymes

Insulin Vs Glucagon

Type 1 Diabetes Absolute insulin deficiency It can present at any age (predominately children, particularly at puberty) Caused by a mix of hereditary (polygenic) and environmental factors (viruses) • HLA-associated immune-mediated organ specific disease (autoantibodies directed at pancreatic islets)

Type 2 diabetes • Insulin resistance and deficiency Combination of genetic and environmental factors Gradual insidious onset Increase in glucose stimulates β cells increase insulin production down regulation of receptors= reduced glucose utilization β cells try to compensate but become exhausted impaired glucose tolerance

Secondary diabetes Diabetes that is a result of another underlying medical condition: • Pancreatic disease-CF, chronic pancreatitis • Endocrine-Cushing’s, Acromegaly, thyrotoxicosis • Drug induced-thiazide diuretics, corticosteriods, TB drugs

Gestational Diabetes which presents for the first time during pregnancy Normal physiology to develop some insulin resistance to allow glucose to reach the fetus but can become exaggerated
 Weight loss Polyuria +Nocturia thirst Subacute (several months)")
Clinical presentation Acute (2 -6 weeks) Weight loss Polyuria +Nocturia thirst Subacute (several months) • Lack of energy • Visual blurring • Pruritus and balanitis (candida infections)

Diagnosis • Clinical presentation • Fasting plasma glucose >7. 0 mmol/l • Random plasma glucose >11. 1 mmol/ • The oral glucose tolerance test (borderline cases and gestational diabetes) • Hb 1 Ac-measures glucose over the past 3 -6 months- >6. 5% or 48 mmol/1 mol

Complications Macroangiography -CVD, MI, Stroke Microangiography • Nephropathy • Neuropathy • Retinopathy
= abnormal function (increase")
Pathophysiology • High glucose glycated proteins (collagen in the interstitial matrix)= abnormal function (increase in LDL absorption atheroma) • Polyol pathway glucose sorbitol fructose (increase in intracellular osmolality influx of water and impairment of the ion pumps) The reaction consume NADPH=free radicals=oxidative stress • Increase in protein kinase C activity VEGF-new vessel production, an increase pro-inflammatory mediators and an increase in endothelin + decrease in NO=vasoconstriction
 Patient")
Nephropathy Hyperinfiltration Increased thickness of the basement membrane (note ACE inhibitors are beneficial) Patient presents with nephrotic syndrome and glomerlusclerosis (Ig. A) -proteinuria, hypoabluminaemia, odema Kimmelstiel-Wilson’s lesion

Neuropathy • Axonal loss= increase in nerve conduction distance • Thickening of the basement membrane Thought to be caused by a combination of oxidative stress and glycated proteins affecting both the nerves and blood supply

Retinopathy • Leaky vessels microaneurysms occlusion of vessels • Haemorrhages • Proliferative and non-proliferative

Treatment Insulin Treatment • Bolus dosage • Short acting • Long acting Infusion devices (disadv-infection and DKA is broken)

Complications • At the injection site-painful, red lesions and lipohypertrophy • Weight gain • Hypoglycaemia – Blood glucose <3 mmol/L – Sweating, tremor, palpitations, pale, drowsy, clumsy, inappropriate behavior, confusion, coma – Treatment • Mild-fasting acting glucose followed by slower releasing glucose • Severe- intramuscular glucagon (1 mg) or IV glucose

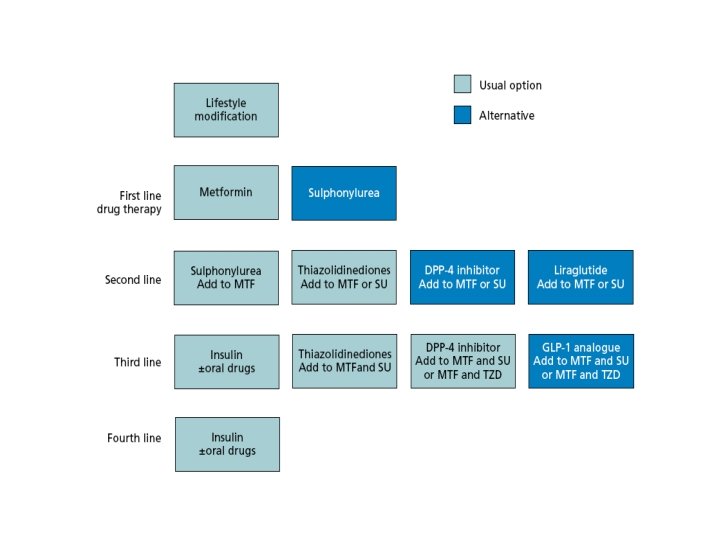
Tablet Treatments Glitazones/thiazolidinediones -regulates the expression of metabolism of GLUT 4 receptors in adipose tissue (increase glucose uptake) roseglitazone Adipose tissue Biguanides -reduce hepatoglucogenesis -increase glucose uptake metformin Liver Pancreas Post-prandial glucose regulation -acts on K+ pump (but different site) nateglinide α-glucosidase -inhibits α-glucosidase in the gut reducing CHO absorption reducing post prandial glucose peaks Sulphonylureas -inhibits ATP dependent K+ pump=Ca 2+ influx -increases the secretion of insulin glicaside Incretins -DDP-4 inhibitor binds to binding site +prevents GLP-1 breakdown -GLP-1 stimulate β-cells Small intestine
 •")
Measuring Metabolic Control • Urine tests (not as good as testing blood glucose) • Home blood glucose testing (finger prick) • Glycosylated haemoglobin (Hb. A 1 c)

DKA Acid/base balance 2 -5% mortality Biggest complication=cerebral oedema Generally only found in patients with type 1 diabetes Acidaemia p. H <7. 3 Triad of symptoms Hyperglycaemia<11. 1 mmol/L Ketonaemia (<3 mmol/L) or ++ urine

Mechanism A lack of insulin rise in glucose in the blood hyperglycaemia proteins Cells Lipids =ketones Ketones produces an acidosis Kussmaul breathing exhuastion coma The plasma glucose reaches the renal threshold causing glucose to be excreted by the kidneys osmotic diuresis and glycosura dehydration coma Insulin is also important in regulating the Na/K pump. Intracellular K becomes low hypokalamic (but noraml levels in blood due to kidneys tight control) Note: need to give K when treating the patient as insulin move K into the cells

Clinical presentations

Treatment • Fluids to correct dehydration-0. 9% saline, 40 mmol K added to each bag, strict fluid balance. NG tubes and catheter with fluid balance chart and check electrolytes and glucose every hour • Insulin-0. 1 U/Kg intravenous insulin infusion, aim to reduce glucose by 3 mmol/L per hour (faster risk of cerebral oedema) • Introduce 10% glucose when BMs <14 -prevent hypos • Treat underlying cause
 • Serum hyperosmolarity (>340) servre intracellular dehydration • Causes")
HONK • Extreme hyperglycaemia (>40) • Serum hyperosmolarity (>340) servre intracellular dehydration • Causes altered mental state, neurological signs, coma is rare • No ketosis as low levels of insulin prevent lipolysis but levels are insufficient to reduce blood glucose • Complications-thromboembolic events, infarctio, cerebral oedema, multiorgan failure • Overall mortality up to 30% (more than DKA-elderly population)
- Slides: 26