Diabetes and the Surgical Patient Original Author Tammy

Diabetes and the Surgical Patient Original Author Tammy Lucht RN CDE Jeff Worrell, CRNA Susan Martin, Cardiac Rehab/Diabetes RN
 Compare normal glucose metabolism with that of type 1 and type 2")
Objectives 1) Compare normal glucose metabolism with that of type 1 and type 2 diabetes 2) Describe how stress, anesthesia, medications impact blood glucose levels 3) Describe the perioperative nursing management of the patient with diabetes 4) Discuss the impact of hyperglycemia on morbidity and mortality of the surgical patient

Overall Numbers, Diabetes and Pre Diabetes- ADA Statistics �Prevalence : 2015 30. 3 Million American or 9. 4% of the population, Approx. 1. 25 mil. American Children and Adults have Type 1 diabetes (29. 1 mil in 2014) �Undiagnosed: Of the 30. 3 mil, 23. 1 mil were DX and 7. 2 mil were undiagnosed (improvement) 8. 1 mil in 2014 �Prevalence in Seniors: 65 or older diagnosed and undiagnosed 25. 2 or 12 million �New cases: 1. 5 million each year �Prediabetes 84. 1 million 18 or older ( 86 million 2014) �Deaths: 7 th leading cause Under reported… 10 -15% of deaths have DM listed as an underlying cause of death
 of Hospital Discharges with Diabetes as Any -Listed Diagnosis, United States,")
Number (in Thousands) of Hospital Discharges with Diabetes as Any -Listed Diagnosis, United States, 1988– 2009. From 1988 to 2009, the number of hospital discharges with diabetes as any-listed diagnosis increased from 2. 8 million to nearly 5. 5 million http: //www. cdc. gov/diabetes/statistics/dmany/fig 1. htm

Diabetes and Surgery � 25% patients with diabetes will require surgery �Mortality rates in these patients have been estimated to be up to 5 x’s higher than in patients without diabetes �Infections account for 66% of postop complications and 25% of perioperative deaths
 Kidneys aid sugar reabsorption into blood stream In pancreas: Beta")
Normal Glucose Metabolism (5) Kidneys aid sugar reabsorption into blood stream In pancreas: Beta cells release insulin in response to glucose rise; Alpha cells release glucagon when glucose is low

Glucose Tolerance Categories 2 -hr PG on OGTT FPG mg/d. L 126 100 and <126 <100 Fasting Plasma Glucose Diabetes Mellitus Impaired Fasting Glucose Normal mg/d. L Oral Glucose Tolerance Test 200 Diabetes Mellitus 140 and <200 Impaired Glucose Tolerance <140 Normal The Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Diabetes Care. 2004; 25(suppl): S 5

Goals for Glycemic Control: FPG, PPG and A 1 C Goal plasma blood glucose ranges for people without diabetes Goal plasma blood glucose ranges for people with diabetes Before breakfast (fasting) Before lunch, supper and snack Two hours after meals Bedtime < 100 < 110 < 140 < 120 80 - 130 < 180 90 - 150 A 1 C (also called glycosylated hemoglobin A 1 c, Hb. A 1 c or glycohemoglobin A 1 c) < 6% < 7% Time of Check http: //www. joslin. org/info/goals_for_blood_glucose_control. html

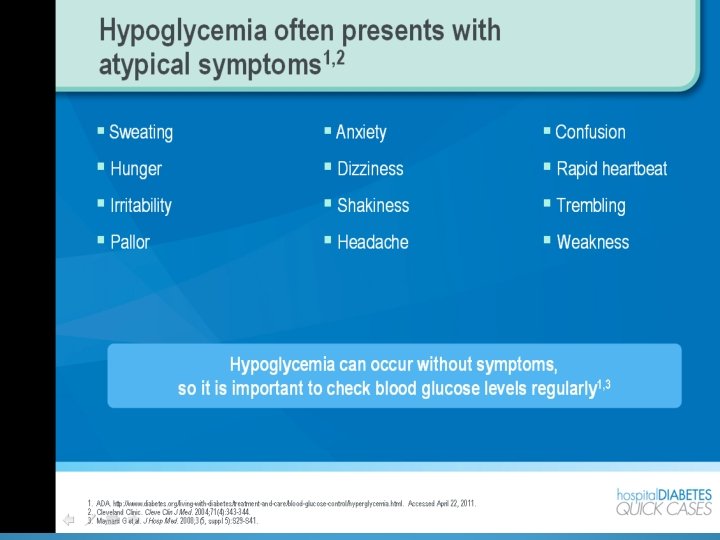
Signs and Symptoms �Polyuria �Polydypsia �Polyphasia �Wounds slow to heal �Fatigue �Blurry vision �Or~ no symptoms at all

Type 1 v. s. Type 2 Diabetes Age of onset Type 1 DM (< 10%) < 40 Type 2 DM (> 90%) > 40 DKA Yes No Weight Usually lean 80% overweight Cause Autoimmune or No autoimmune unknown markers

Pathophysiology of T 1 DM antibodies attack islets!

Pathophysiology of Type 1 Diabetes Loss of -cell mass Insufficient endogenous insulin Absolute insulin deficiency ADA. Diabetes Care. 2002; 25(suppl 1): S 1

Pharmacologic Treatment for Type 1 Diabetes �Type 1= absolute insulin deficiency �SOME insulin will be required when: �Carbohydrates are consumed…Insulin: CHO ratio/Insulin Sensitivity Factor for a correction factor �To correct for hyperglycemia �Basal insulin vs bolus insulin �Inadequate insulin administration DKA

VIACYTE - PANCREAS IN A CAPSULE ENCAPSULATION RESEARCH Phase I/II clinical trial of a stem cell-derived therapy for patients with Type 1 diabetes has started Encapsulates immature human pancreatic cells derived from stem cell source in an immune-protective device

Multi Dose Insulin Injections Glargine QD + rapid-acting analog AC Breakfast Lunch Insulin Action Dinner Glargine 8: 00 12: 00 18: 00 Time 21: 00

Continous glucose monitor

Insulin Used for 9 hrs • Glucose-responsive insulin. • Glucose sensing enzymes • Studied in animal models
 Glucose (mg/d. L) 350")
Natural History of Type 2 Diabetes Relative -Cell Function (%) Glucose (mg/d. L) 350 300 250 200 150 100 50 PPG Fasting glucose 250 Insulin resistance 200 150 100 Insulin level -cell failure 50 0 – 10 – 5 0 5 10 15 20 Diabetes (yr) 25 30 Bergenstal R et al. In: De. Groot L, Jameson J, eds. Endocrinology. 4 th ed. Philadelphia, Pa: W. B. Saunders Company; 2001: 821. Originally published in Type 2 Diabetes BASICS (Minneapolis, International Diabetes Center, 2000). Adapted with permission from International Diabetes Center (IDC)

Pathophysiology of T 2 DM Hepatic glucose output + Blood glucose diet INSULIN Peripheral Tissue Uptake Type 2 Diabetes = Relative Insulin Deficiency

Sites of Action of Currently Available Therapeutic Options ADIPOSE TISSUE LIVER MUSCLE PANCREAS GLUCOSE PRODUCTION Metformin Thiazolidinediones: Avandia, Actos INTESTINE PERIPHERAL GLUCOSE UPTAKE Thiazolidinediones Metformin Insulin INSULIN SECRETION Sulfonylureas: Glyburide, Glimepiride Non-SU Secretagogues: Repaglinide, Nateglinide GLUCOSE ABSORPTION Alpha-glucosidase inhibitors – slow cho breakdown GLP-1 agonists : Byetta DPP 4 Inhibitors: Janumet – combo with metformin SGLT 2 Inhibitor Invokana Blocks glucose reabsorption from the kidney Kidney
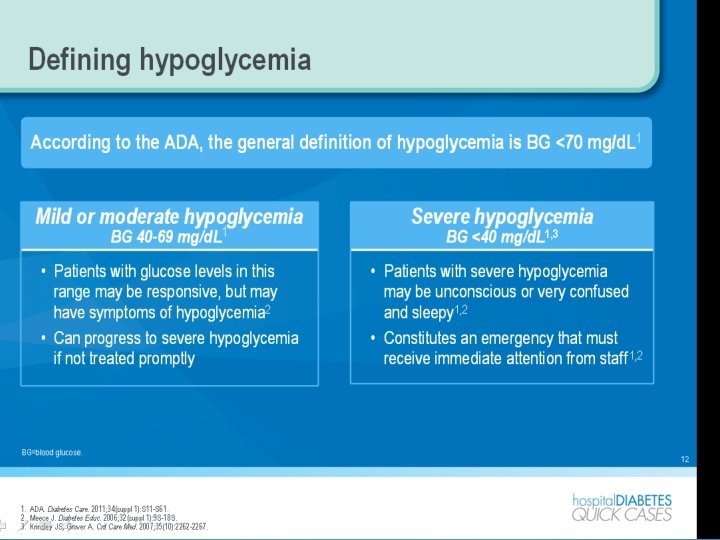

Treating Hypoglycemia: Rule of 15 Hypoglycemia Unawareness �Give 15 grams of carbohydrate orally if alert � 4 oz juice � 8 oz milk � 4 glucose tabs �Wait 15 minutes, re-test �If < 70 mg/d. L: re-treat with 15 grams of carbohydrate �If > 70 mg/d. L: give snack if more than 30 minutes before next scheduled meal �If not alert: give D 50 IV per protocol

Dextrose IV �D 5 W = 5 grams dextrose / 100 ml �D 10 W = 10 grams dextrose / 100 ml �D 25 W = 25 grams dextrose / 100 ml �D 50 W = 50 grams dextrose / 100 ml � 4 calories per gram of glucose �Dextrose is one of two isomers of glucose

Algorithm- Diabetes medication and surgery Patient information Day before surgery Day of Surgery During surgery Considerations for best outcome After surgery

Stress, Anesthesia, Medications Their Impact on Glycemic Control

Hyper-metabolic Stress Response “Stress Hyperglycemia” Initially considered beneficial as a source of energy. However, evidence indicates numerous adverse side effects cause serious clinical outcomes. Hyperglycemia develops in both diabetics and nondiabeteics • Administration of dextrose-containing IV fluids • Hypothermia causes insulin secretion and sensitivity • Increased substrate availability in forms of lactate-the forgotten fuel • Decreased exogenous insulin activity • Heparin administration in cardiac patients. . prevents intercellular synthesis • Administration of glucose containing cardioplegic solutions

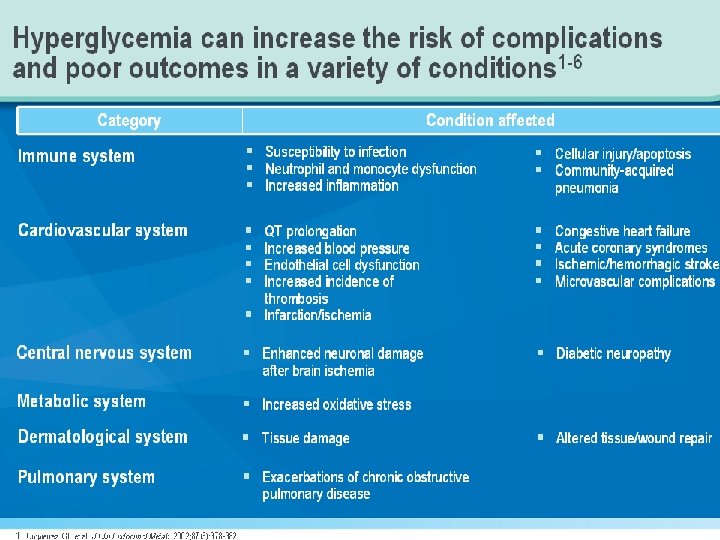
Adverse Affects of Hyperglycemia �Risk of infection increases…abnormal function of monocytes and neutrophils…decrease intracellular bactericidal activity and glycosylation �Blood coagulation is activated by hyperglycemia…as circulating prothrombin fragments and D-dimers increase platelet aggregation and thrombosis occur �Hyperglycemia induces inflammation and activates a pro-inflammatory cytokines �Hyperglycemia abolishes intrinsic myocardial protective mechanisms such as ischemic pre conditioning

Perioperative Management �Surgery impacts BG regulation �Incisional pain, emotional stress, hypothermia, steroids may increase insulin needs, decrease insulin sensitivity �Surgery induces stress response �Release of catecholamines, glucagon, cortisol �These all raise BG by stimulating hepatic glucose release and inhibiting peripheral glucose uptake Increased need for insulin during surgery � Frequently given by IV drip � �Anesthesia impacts BG �Inhaled agents may suppress insulin secretion � Regional blocks may decrease this stress response

Characteristics of Surgery �Minor vs Major … greater metabolic disturbance �Timing …how long pt goes without food, how we dose antidiabetic medications �Duration…longer surgery greater metabolic abnormalities �Types of Anesthesia …Regional and epidural minimal effects on glucose demand

Hemodynamic, Metabolic, and Neuroendocrine Changes During Surgery and Anesthesia in Patients With Diabetes �Release of counter-regulatory hormones (i. e. , epinephrine, cortisol, growth hormone) �Tachycardia and tendency to cardiac arrhythmia �Vasoconstriction and labile blood pressure responses �Elevated peripheral insulin resistance �Reduced insulin secretion �Enhanced hepatic gluconeogenesis �Decreased peripheral glucose utilization �Accelerated adipose tissue and protein catabolism �Electrolyte abnormalities Rizvi. A, J Am Acad Orthop Surg 2010; 18: 426 -435

Consensus Recommendations for Target Inpatient Blood Glucose Concentrations Patient Population Blood Glucose Target Rationale General medical/surgical* Fasting: 90 -126 mg/d. L Random: < 200 mg/d. L Decreased mortality, shorter length of stay, lower infection rates Cardiac surgery* < 150 mg/d. L Critically ill† < 150 mg/d. L Acute neurologic disorders‡ 80 -140 mg/d. L Reduced mortality, reduced risk of sternal wound infections Beneficial effect on shortterm mortality, morbidity; length of stay Lack of data, consensus on specific target; consensus for controlling hyperglycemia *American Diabetes Association. †Society Critical Care Medicine. ‡American Heart Association/American Stroke Association

Current Recommendation for critical ill patients �ADA and AACE…start Insulin Infusion when glucose is persistently greater than 180 mg/d. L aiming for target BG range 140 -180 mg/d. L �American College of Physicians…target 140 -200 mg/d. L “Both societies agree that adverse outcomes, including death and hypoglycemia are increased in patients that receive intensive insulin therapy. Thus, tight control is not recommended. Instead, toleration of mild hyperglycemia appears to benefit outcomes” • Tight control… 80 -110 mg/d. L www. ncbi. nlm. nih. gov Hyperglycemia and Perioperative Glucose Management 2013, Andra E Duncan MD, Cleveland Clinic Lerner College of Medicine

Steroid Meds Impact on BG Control Prednisone induces elevated glucose levels by stimulating glucose secretion by the liver as well as reducing glucose transport into adipose and muscle cells. The overall effect is a reduction in glucose clearance. Elevated glucose levels can lead to glucose toxicity further impairing insulin secretion. �Steroids that are suddenly decreased can cause hypoglycemia �Prednisone: predominant impact is post-meals, taken in am will persist through afternoon �Chronic steroid use suppresses stress response and may lead to severe autonomic derangements unresponsive to vasopressors � Stat administration of IV corticosteroids may be necessary

What do you need to know about your patients with diabetes? � What meds do they take for their diabetes at home or what insulin are they being given on the floor? � What they last take and when? � Insulin : the mainstay of glucose control in hospitalized patients � Basal insulin: glargine (Lantus) � � Meal time insulin: aspart (Novolog), lispro (Humalog), glulisine (Apidra) � � Lasts 3 -6 hrs. , peak at 1 ½-2 hours, hold am of surgery Correction insulin: aspart � � � Lasts 24 hrs. , no pronounced peak, dose may be decreased am of surgery Given to correct hyperglycemia, not in response to food May be given am of surgery May be given subcutaneously or IV (regular insulin only) � Oral agents � Should be held am of surgery, as a rule � Will probably not be used for inpatients � Metformin discontinued 24 -48 hours before surgery

Insulin Administration and the Hospital Insulin pump: Patient is the best resource
 INSULIN INFUSION: Mix 1 U Regular Human Insulin per")
Initiating An Insulin Drip 1) INSULIN INFUSION: Mix 1 U Regular Human Insulin per 1 cc 0. 9 % Na. Cl. Administer via infusion pump (in increments of 0. 5 U/hr). PRIMING: Flush 50 cc of Insulin/NS drip through all IV tubing, before infusion begins (to saturate the insulin binding sites in the tubing) 2) TARGET BLOOD GLUCOSE (BG) LEVELS: 100 -139 mg/d. L 3) BOLUS & INITIAL INSULIN DRIP RATE: Divide initial BG level (mg/d. L) by 100, then round to nearest 0. 5 U for bolus AND initial drip rate Example: Initial BG = 325 mg/d. L: 325 ÷ 100 = 3. 25, rounded ↑ to 3. 5: IV bolus 3. 5 U + start drip @ 3. 5 U/hr

Algorithm- Diabetes medication and surgery Patient information Day before surgery Day of Surgery During surgery Considerations for best outcome After surgery

Considerations � Timing of surgery � Morning preferred � � To avoid long periods of NPO status Need q 2 or q 4 -6 hour BG check � Intra-operative monitoring � Controlled by anesthesia � � IV access makes for easier balance of hypo and hyperglycemia Frequency determined by type of surgery, length of surgery, pre-op BG trends, age, frailty, etc � Post-operative monitoring � BG within range for your institution (generally less than 150 mg/d. L) � Communicate BG readings and treatment in transition of care report � Document last insulin dose, BG check and communicate to receiving RN � Aseptic technique is critical � Decrease incidence of postop infections � Hyperglycemia is a risk factor of increased morbidity and mortality (with or without a diagnosis of diabetes) � Infection causes rise in glucocorticoids, epinephrine and norepinephrine ( increase in heptatic glucose rise in BG). Makes it much more difficult to control BG!

BG Control: Impact on Morbidity and Mortality in Hospitalized Patient

Diabetes is associated with increased risk of postoperative complications and LOS Non Diabetic 14 Diabetics 12 10 8 6 4 2 0 Death Pneumonia Wound INF Sepsis UTI AMI ARF Emery University “Diabetes Care” 33: 1783 -1788, 2010 Thirty-day mortality and in-hospital complication rates in patients with and without diabetes

Hyperglycemia: An Independent Marker of In-Hospital Mortality in Patients with Undiagnosed Diabetes Total In-patient Mortality 30 Mortality (%) 30 20 10 0 * P < 0. 01 16. 0% * 20 10 1. 7% 3. 0% 0 Normoglycemia Known Diabetes Umpierrez GE et al, J Clin Endocrinol Metabol 87: 978, 2002 New Hyperglycemia

Blood Glucose Control Matters �Patients with Diabetes or Hyperglycemia risk higher complication rates with hospitalization �Controlling BG before, during and after surgery is important �Having a transition of care plan for BG control is imperative � If patient is discharging to home: � When did they last receive insulin? � When should their next dose be? What kind of insulin? Documentation, discuss with patient/caregiver � If blood sugars don’t return to goal FOLLOW UP WITH PROVIDER � If patient is going to inpatient setting: � When did they last receive insulin? What kind? � Initiate/resume subcutaneous insulin order: this is VITALLY important for BG control

Algorithm- Diabetes medication and surgery Patient information Day before surgery Day of Surgery During surgery Considerations for best outcome After surgery

Minor Surgery- Morning List Brenda T 1 DM • Average pre-breakfast BSs = 80 Time: 0800 hours Regime: 10 units SA TID and 20 units of • Surgery: WLE and SSG of a skin Lantus lesion Day Before: No Change Morning of: Withhold morning SA insulin Intraoperative • • Post-Op Usual dose AM dose With breakfast Consider: Prevent hypoglycemia Day Before reduce LA by 10 % Day of: monitor BSs closely, Proceed complete by 10 am, delayed breakfast and SA dose

Minor Surgery-delayed morning Blood Sugars trending up Ben Current BSs: 180 mg/dl T 2 DM Time: Delayed 0930 Surgery: Hernia Repair Regime: 70/30 intermediate BID 40 units/20 units Day Before: No Change Morning of: Consider modified Insulin dose Or insulin infusion Intra-Operative Post-Op • Half SA insulin dose • With meal Consider: Due to delay and trending up blood sugars Morning of consider 50% of normal dose Post-Op: Consider late lunch with SA insulin

Major & Minor Surgery-Afternoon Jen 35 yo T 1 DM Surgery: Total Thyroidectomy Time: 1300 Day Before: No change Morning of: Half SA Half LA insulin Regime: 16 units Rapid TID & 24 units Lantus morning Light Breafast Fasting Since 0600 Intraoperative Special Note: T 1 DM never with hold insulin With light breakfast give half of each insulin. Monitor BSs closely Glucose infusion during surgery Post Op: Major procedure Insulin infusion until tolerating food Post-Op

Summary-Morning List No Change Day before: Delayed Withh old Morning of: Insulin Infusion Intra-op: Post-op: Major: Infusion Modified Insulin or Infusion Insulin Infusion Minor: Am dose +breakfast SA Insulin + Meal

Key Principals �Morning surgeries preferred for Diabetics �No change day before. . . May reduce LA Insulins by 10 % �Day of Surgery …May reduce am dose of LA/SA insulin by 50% �Modified insulin infusion for delayed procedures or deranged BSs �Wean Insulin infusions once able to tolerate solids �Never withhold insulin completely in T 1 DM �When in doubt, ASK!!!

Resources �National Institute of Health www. ncbi. nlm. nih. gov �American Diabetes Association www. diabetes. org �American Association of Diabetes Educators �www. diabeteseducator. org �Diabetes In Control �www. diabetesincontrol. com �American Association of Clinical Endocrinologists �www. aace. com
- Slides: 52