Diabetes and Proteinuria Dr Ruba Nashawati Diabetes q

Diabetes and Proteinuria Dr. Ruba Nashawati

Diabetes q Leading cause of ESRD q 30% 40% � DN q DN Risk type I = type II

Familial Cluster Type I 83% 1 st degree relative Type II 74% 1 st degree relative

Renal Injury Hemodynamic Hyperperfusion Glucose balance Hyperproliferation 4

Diabetic Nephropathy 5

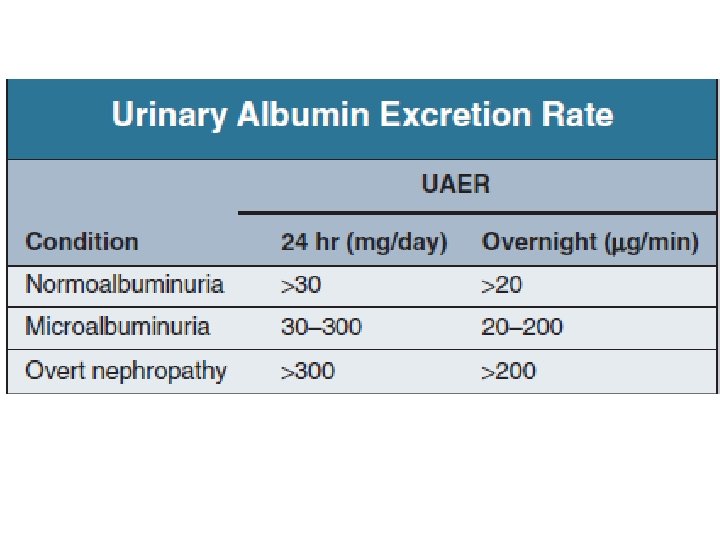
Clinical syndrome Persistent Albuminuria >300 mg/24 hr � GFR � HTN Cardiovascular Morbidity And Mortality

Proteinuria 8

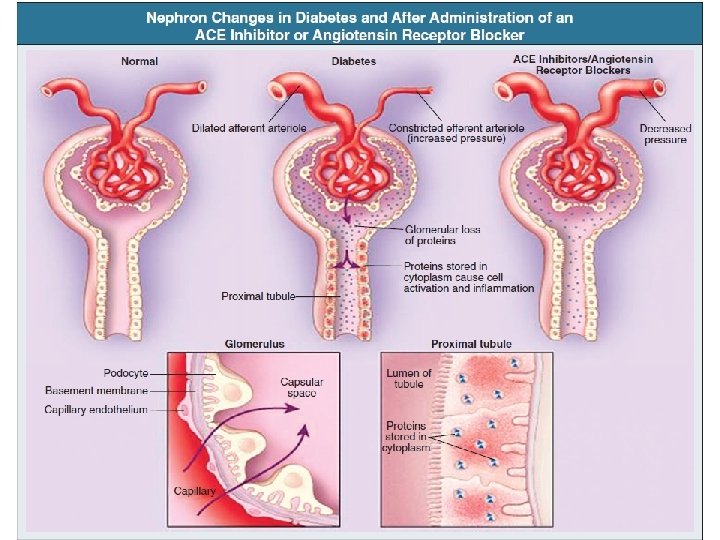
Glomerular Barrier tubule q Normally, the larger Proteins are excluded at the glomerular barrier q Smaller proteins can pass, but are mostly Reabsorbed 9

Leaky Glomerular Barrier tubule Large Proteins are able to pass by the abnormal glomerular barrier 10

11
 Plasma proteins Nonplasma Proteins Albumin 12 Tamm-Horsfall protein 40 Immunoglobulin")
PLASMA PROTEINS EXCRETION (mg/day) Plasma proteins Nonplasma Proteins Albumin 12 Tamm-Horsfall protein 40 Immunoglobulin G 3 Other non–renal <1 Immunoglobulin A 1 All Nonplasma proteins 40 Immunoglobulin M 0. 3 Light chains χ 2. 3 λ 1. 4 β-Microglobulins 0. 12 Other plasma proteins 20 All plasma proteins 40 Total Proteins 80 ± 24 12

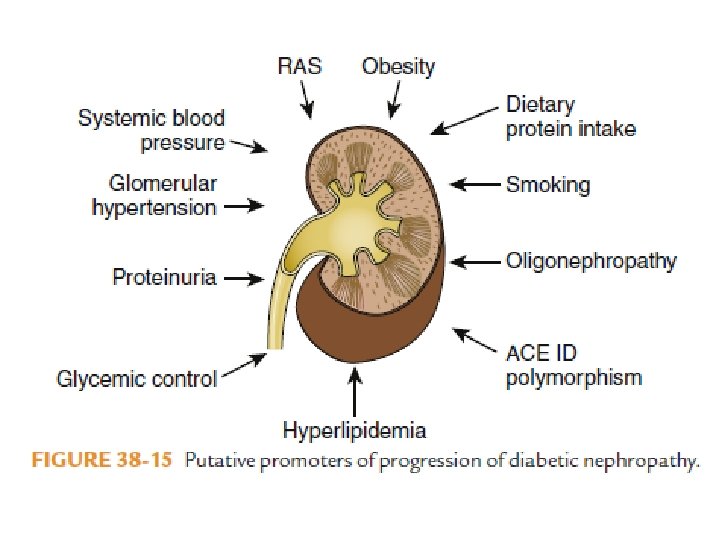
� Systemic Hypertension Hyperperfusion � Capillary Pressure � Glomerular Hydrostatic Pressure Proteinuria 13

Renin-Angiotensin-Aldosterone System Sites of action: 1. Podocytes 2. Mesangial cell 3. Endothelial cell 4. Renal vessels 5. Tubular cell
 1. Proliferation 2. Hypertrophy 3. Matrix Expansion 4.")
Renin-Angiotensin-Aldosterone System Hemodynamic Nonhemodynamic (Mediates Cell) 1. Proliferation 2. Hypertrophy 3. Matrix Expansion 4. Cytokine(TGF-β)synthesis

Diagnosis 17

Edema often 1 st symptom DN 18

Urine Dipstick Only Albumin � Insensitive in Microalbuminuria � 19

Spot Urine Albumin/Creatinine Ratio Easy � Yearly � Control DM patient � 20

Gold standard 21

Albuminuria 22
 � persists over 3 -6 month")
Microalbuminuria �� Albumin excretion (30 to 300 mg/day) � persists over 3 -6 month � 24

25

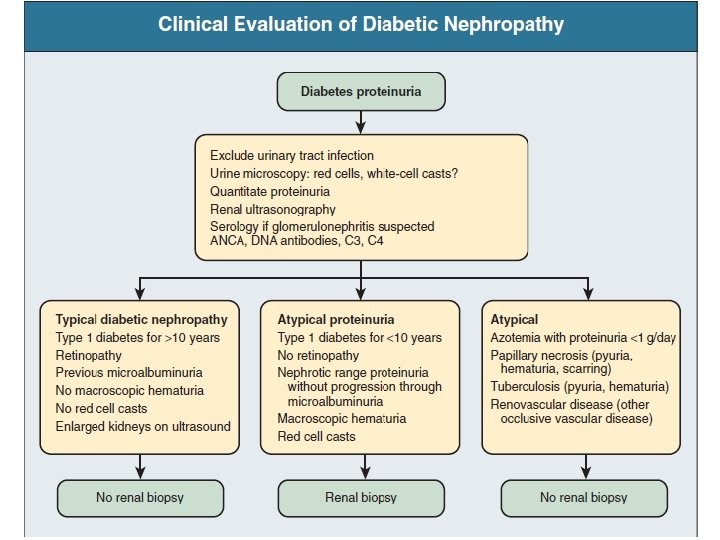
Clinical Evaluation Of Diabetic Nephropathy 26

Treatment Of Diabetics With Microalbuminuria Or Overt Nephropathy 29

Goal Reduce Progression of Nephropathy + Minimize the risk for CV events the rate of

31

Diabetic Nephropathy

corrected Good Glycemic Control ACEi

Anti Hypertensive Agents 34

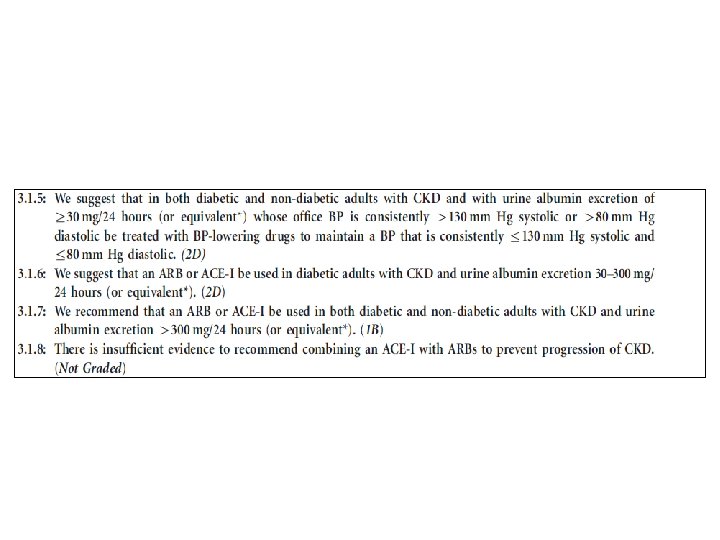
ACEi /ARBs Hypertensive + Diabetic Normotensive + Nondiabetic + Ratio>30 mg/g 35

ACEi /ARBs v Don’t prevent Proteinuria v Reverse the progression of Proteinuria 60% 36

ACEi /ARBs v Stop �Cr >30% �K AKI v CKD = not contraindication 37

ACEi /ARBs Check Creatinine day 3 week 2 38

Diuretics Loop diuretics Thiazide Aldosterone Antagonist 39
 Are Anti Proteinuric 40")
Calcium Channel Blocker Only Nonhydropyridin CCB (Diltiazem , Verapamil) Are Anti Proteinuric 40

B-Blocker 41

Direct Renin Blocker Aliskiren 42

Glycemic Control 44

Strict DM+DN � HBA 1 c 7. 0% Type I Evidence Based 45

More aggressive in 1. Young 2. Short DM Duration 3. High Life Quality 4. Risk Of Hypoglycemia 46

Treatment Of Dyslipidemia 47

1. Usually �HDL + �Tg 2. Type II +Non-Dialitic �statine 3. ESRD �too late 48

Goal 1. 2. DM �LDL <100 mg/dl DM +CVD �<70 mg/dl 49

Non Pharmacologic 50

� Low Protein Diet 0. 8 g/Kg/Day � K + Na Restriction � Life Style Modification 51

Other New 52
 +ARBs � MMF � Fish Oil")
� Peroxisome Proliferation Activated Receptors � Thiazolidinedione (Pioglitazone) +ARBs � MMF � Fish Oil 53

Take Home Messages 54

Proteinuria � Early discover � DM control � ARBs /ACEi as Detected 55

56

57
- Slides: 56