DIABETES and PREGNANCY PRESENTER LAMIN F JARJU 5

DIABETES and PREGNANCY PRESENTER LAMIN F JARJU 5 th yr medical student

OUTLINE v Bibliography v Introduction v Definition v Types of diabetes v Pathophysiology of DM v Physiology of insulin resistance in pregnancy v C/f and investigations v Risk factors for development of DM in Pregnancy v Maternal and Neonatal complications of Diabetic pregnancy v Importance of screening for DM in Pregnancy v Antenatal and intrapartum management v Key Points v The End

Bibliography Ø Obstetrics by Ten teachers 18 th edition Edited by Philip N Baker Ø Current Diagnosis and treatments in Obs and Gynae 10 th edition Ø Excerpted from Mosby's Medical Encyclopedia. Copyright (c) 1994 -5, 1996, 1997 Ø Some articles downloaded from the internet

Some facts ü Diabetes is the most common medical complication of pregnancy ü DM affects approximately 6% of the U. S. population; ü it is the leading cause of irreversible blindness and chronic renal failure. ü Diabetes is found worldwide, and the incidence is increasing rapidly. ü Diabetes is undiagnosed in nearly 1 -3 rd of adults with the condition

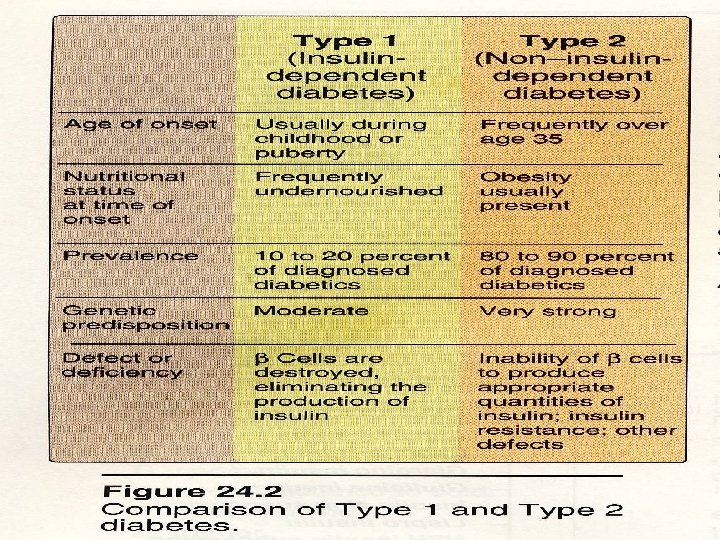
Some facts ü Type I accounts for 10% to 15% of cases, and the age of onset is primarily childhood or adolescence. ü Type II accounts for 85% to 90% of cases, and onset generally occurs after age 40. ü Preexisting (type 1 or type 2) diabetes mellitus affects approximately 1– 3 per 1000 pregnancies ü GDM complicates approximately 4% of pregnancies

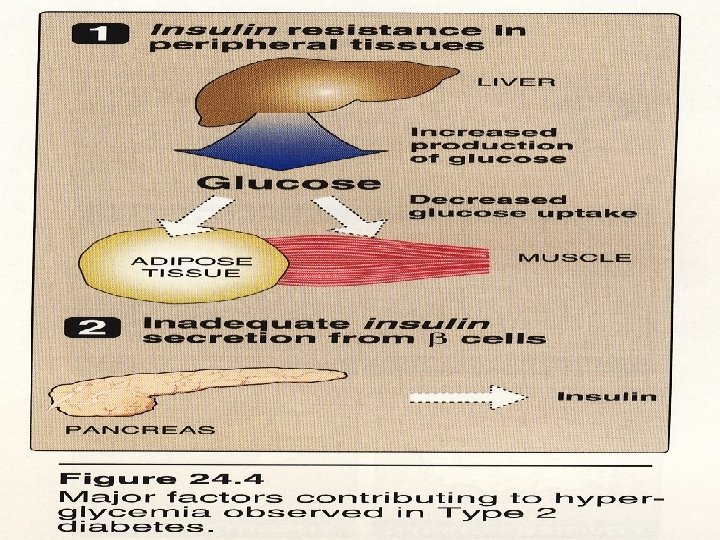
DIABETES MELLITUS ØA disease complex characterized by persistent hyperglycemia caused by insufficient insulin production or resistance to the metabolic action of insulin. ØDiabetes mellitus (DM) is generally classified as insulindependent (IDDM, type I), non-insulin-dependent (NIDDM, type II), or secondary diabetes mellitus. ØWHO: FBS>7. 0 mmol/l RBS>11. 1 mmol/l
, defined as glucose intolerance with onset or")
GESTATIONAL DIABETES MELLITUS Gestational Diabetes Mellitus (GDM), defined as glucose intolerance with onset or first recognition during pregnancy: q. Is linked with future developments of diabetes mellitus in women postpregnancy.

Table 18– 3. Diagnostic Criteria for Gestational Diabetes Mellitus. 100 -g Glucose Load (mg/d. L) 75 -g Glucose Load (mg/d. L) Fasting 95 95 1 hour 180 2 hour 155 3 hour 140 — Diagnosis based on 2 values above listed cutoff values

Insulin resistance in Pregnancy Anti-insulin environment is aided by: Ø Placental lactogen - Like growth hormone - Increases lipolysis and FFA - Increases tissue resistance to insulin Ø Increased unbound cortisol Ø Estrogen and Progesterone may also exert some antiinsulin effects Ø Prolactin levels are increased 5 - to 10 -fold during pregnancy and may impact carbohydrate metabolism Ø These changes are most marked during the third trimester

Risk factors for the development of diabetes in Pregnancy Ø Obesity (body mass index >30) Ø Family history of diabetes Ø Previous baby >4. 5 kg Ø Previous unexplained stillbirth Ø Previous congenital abnormality Ø Prior history of GDM Ø Patients older than 25 yrs Ø Patients with polycystic ovary syndrome Ø Heavy glycosuria (>2+)

C/F Ø Polydipsia Ø Polyuria Ø Polyphagia Ø Weight loss Ø Lethargy Ø Pruritus vulvae or balanitis

Investigations Ø FBS Ø Screening urine for proteinuria Ø Serum urea and electrolytes Ø Liver biochemistry Ø Cholesterol and TAG level ( fasting blood)
 Ø Retinopathy (progression) Ø Coronary")
Maternal complications of diabetic Pregnancy Ø Nephropathy (temporary worsening) Ø Retinopathy (progression) Ø Coronary artery disease Ø Hyperglycemia/hypoglycaemia/ketoacidosis Ø Pre-eclampsia Ø Infection Ø Thromboembolic dz Ø Premature labour Ø Polyhydramnios

Maternal Hyperglycemia Ø Causes fetal hyperglycemia Ø Leading to fetal hyperinsulinaemia Ø Fetal hyperinsulinaemia - even short periods (1 -2 hours) lead to detrimental consequences in: – fetal growth – fetal well-being

Fetal Hyperinsulinaemia Ø Promotes storage of excess nutrients - macrosomia Ø Increased catabolism of excess nutrients - energy usage and fetal oxygen storage Ø Episodic fetal hypoxia, catecholamines causing: - hypertension, - cardiac remodelling and hypertrophy, - Erythropoietin, RBCs, haematocrit causing poor circulation and hyperbilirubinaemia

Causes of Neonatal complications Ø Congenital abnormalities -- cardiac -- neural tube defect Ø Macrosomia -- birth asphyxia -- traumatic birth injury eg brachial plexus injury -- shoulder dystocia Ø Respiratory distress syndrome Ø Hypoglycaemia Ø Hypomagnesaemia Ø Polycythaemia Ø Hyperbilibinaemia leading to jaundice

Table 18– 1. Some Congenital Anomalies of Infants of Diabetic Mothers. Cardiac Atrial septal defects Ventricular septal defects Transposition of the great vessels Coarctation of the aorta Tetralogy of Fallot Truncus arteriosus Dextrocardia Cardiomegaly Central nervous system Neural tube defects Anencephaly Holoprosencephaly Renal Hydronephrosis Renal agenesis Ureteral duplication Gastrointestinal Duodenal atresia Anorectal atresia Omphalocele Spinal Caudal regression syndrome, sacral agenesis
 Ø Increased hyperbilirubinaemia Ø Increased hypoglycemia Ø")
Macrosomia (Greater than 90 precentile, 4200 grammes) Ø Increased hyperbilirubinaemia Ø Increased hypoglycemia Ø Increased acidosis Ø Increased birth trauma q. Macrosomnia as a child and glucose intolerance in adulthood

Screening for diabetes in Pregnancy Screening for diabetes in pregnancy can be justified to diagnose previously unrecognised cases of pre-existing diabetes and to identify a group of women who are at risk of developing NIDDM later in life

Facts to achieve a smooth pregnancy Ø Following an appropriate meal plan Ø Frequent self-monitoring of blood glucose (SMBG) Ø Administer insulin injections and knowing how to adjust the doses depending on results of SMBG Ø Controlling/treating hypoglycemia Ø Adding or maintaining an appropriate level of physical activity

Antenatal Management Ø Pregnant women with diabetes should be managed in a joint clinic with an obstetrician and a physician Ø The aim of treatment is to maintain the blood glucose level as near normal as possible, a combination of diet and insulin Ø In women with IDDM, this will usu require 3 or 4 daily doses of insulin or the newer rapidly acting insulin analogues Ø All women in diabetes should be instructed in selfmonitoring with their own glucose meters Ø Long-term control maybe checked using gycosylated hemoglobin or fructosamine measurement

Antenatal Management Ø Input from a dietician is also important and often a nurse or midwife specialist will act as an adviser to adjust d dose of insulin Ø Obstetric management is aimed at ensuring that the appropriate screening tests are performed Ø Nuchal translucency scanning Ø Detailed ultrasound assessment for fetal anomalies Ø Fetal echocardiography Ø Serial growth scans recommended to detect fetal macrosomia Ø Ultrasound may also alert the to developing of polyhydramnios

Antenatal Management Ø Biophysical profile checks ( fetal body movements, fetal muscle tone and the amt of amniotic fluid) Ø Concern for fetal well-being should lead to increased surveillance with doppler ultrasound and CTG Ø In principle, if pregnancy goes well, management attempts to achieve a vaginal delivery btw 38 -40 wks gestation Ø CS rate amongst diabetic women is often as high as 50% due to macrosomia or maternal complications such as pre-eclampsia Ø The management of preterm labour or polyhydramnios is particularly difficult in diabetic pregnancies

Antenatal Management Ø Tocolytics such as ritodrine or salbutamol are themselves diabetogenic and will tend to elevate blood glucose levels Ø In addition, the administration of IM steroids to improve fetal lung maturation will also tend to elevate blood glucose levels Ø Under this circumstances, increasing doses of insulin and glucose infusion maybe appropriate to ensure normoglycaemia

Severe Hyperglycemia & Ketoacidosis Ø During pregnancy, severe hyperglycemia and ketoacidosis are treated exactly the same as in the nonpregnant state. Ø Insulin therapy, Ø careful monitoring of potassium level, and Ø fluid replacement are crucial for maternal survival. Ø Fetal heart rate monitoring often demonstrates recurrent late decelerations, but these improve as maternal ketoacidosis is corrected

Intrapartum Management Ø During either induced or spontaneous labour, normoglycaemia should be maintained using a sliding scale of insulin Ø Glucose infusion is provided to all patients in labor as 5% dextrose in lactated Ringer's solution or a similar crystalloid Ø Blood glucose level should be tested at hourly intervals Ø Continuous fetal monitoring is advised and fetal scalp blood sampling should be undertaken in the presence of an abnormal CTG

Intrapartum Management Ø If fetal macrosomia is suspected, operative vaginal delivery should be considered with great caution, if at all. Ø Intravenous fluid bolus prior to conduction anesthesia should not contain glucose!!! Ø If a repeat cesarean delivery or other elective surgery is planned, the patient can take her evening insulin doses on the preceding night, but she cannot take the morning dose. Ø The morning of surgery, glucose level is monitored and basal insulin needs usually are treated with continuous intravenous insulin to maintain a glucose between 70 and 120 mg/d. L.

Postpartum Care Ø Following delivery, the insulin requirements of established diabetes will rapidly fall and return to pre-pregnancy levels Ø Women with gestational diabetes should stop their insulin at delivery and glucose tolerance test is performed 6 wks ff delivery to ensure the diabetes has resolved Ø The glucose levels should be kept below 140– 150 mg/d. L to assist the patient in healing. Ø Breastfeeding is encouraged, and snacks can be used to decrease the risk of hypoglycemia.

Postpartum Care Ø If hypoglycemic agents are necessary postpartum, insulin is continued for those women who are breastfeeding, Ø whereas oral agents can be used in the non– breastfeeding mothers. Ø Postpartum weight loss is encouraged. Ø All patients with a history of diabetes or with risk factors should be re-evaluated prior to the next planned pregnancy.
 can be reduced with good blood")
Key Points Ø The incidence of large babies(macrosomia) can be reduced with good blood glucose control Ø Gestational diabetes has a very high recurrence rate in subsequent pregnancies Ø The commonest congenital abnormalities are cleft palate, sacral agenesis and cardiac defects Ø Reduced fetal movements at or near term in women with diabetes with a non-reassuring CTG should lead to delivery as a priority (esp if there abnormal ultrasound finding)

THE END THANKS FOR YOUR KIND ATTENTION GOD BLESS YOU!!!!!!
- Slides: 33