Diabetes and Pregnancy Karen Playforth MFM Associate Professor

Diabetes and Pregnancy Karen Playforth, MFM Associate Professor, Department of OB/GYN September 14 th, 2018

Karen Playforth, MD, MFM I have no conflicts of interest to disclose.


Overarching Objective • Upon completion of this activity, participants will be able to: • Explain the potential impact of metabolic syndrome or diabetes on the reproductive health of females

Specific Objectives • Upon completion of this activity, participants will be able to: • Recognize the importance of preconception counseling in patients with preexisting diabetes mellitus and of post-partum testing and counseling of patients with gestational diabetes mellitus; • List the complications of pregnancy associated with poorly controlled preexisting diabetes mellitus in the first trimester of pregnancy; • Name the complications of pregnancy common to both preexisting and gestational diabetes mellitus; • Describe the baseline lab work and evaluations done in pregnancy for preexisting and gestational diabetes mellitus patients and why; • Recall the goals for blood glucose control in pregnancy and why; • Restate the recommendations for monitoring and delivery timing for pregnancies complicated by diabetes; • Explain the bigger picture of diabetes and the reproductive health of women.

Epidemiology

Epidemiology • Approximately 7% of pregnancies are affected by ANY TYPE of diabetes • Preexisting diabetes complicates ~1 % of pregnancies in US • Type 1 DM accounts for 5 -10% of patients diagnosed with diabetes in the general population • Incidence of Type 2 DM is very dependent on the population studied • Gestational diabetes (GDM) accounts for 86% of diabetes in pregnancy Yang JE, Cummings EA, O'Connell C, Jangaard K: Fetal and neonatal outcomes of diabetic pregnancies. Obstet Gynecol 2006. ACOG Practice Bulletin Number 190, February 2018. ACOG Practice Bulletin Number 60, March 2005.

Epidemiology • Total of 30. 2 million people, or 12. 2% of the U. S. population, have diabetes • 23 million people with diagnosed diabetes • 7. 2 million people with undiagnosed diabetes • 14. 9 million, or 11. 7 %, of all women age 18 years or older have diabetes Data source: 2011– 2014 National Health and Nutrition Examination Survey and 2015 U. S. Census Bureau data.

11. 1% of Kentucky women are diagnosed with diabetes Data source: 2011– 2014 National Health and Nutrition Examination Survey and 2015 U. S. Census Bureau data.

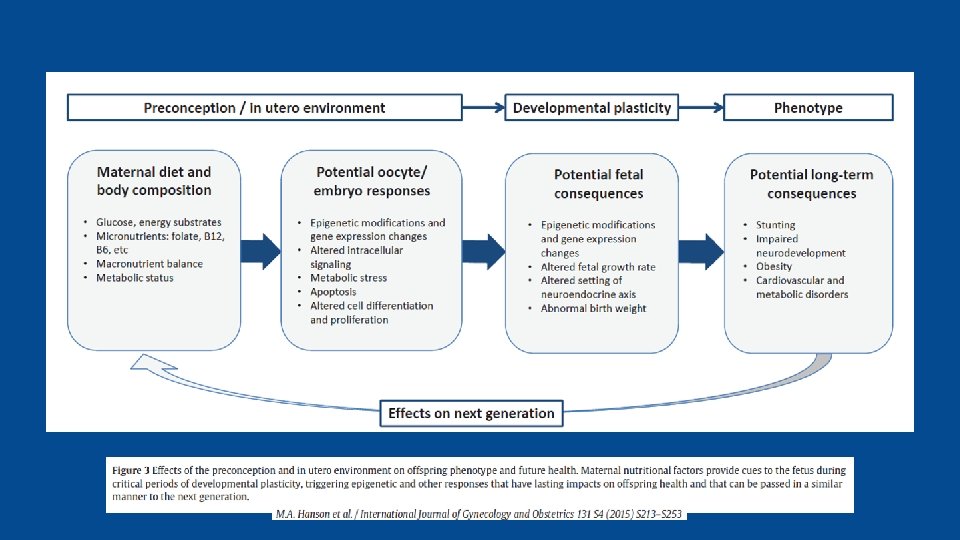
Epidemiology • Risk Factors for Diabetes • • Obesity Sedentary lifestyle Family history Genetics Ethnicity Age INTRAUTERINE ENVIRONMENT

Epidemiology • Exponential rise in numbers of pregnancies affected by diabetes mellitus • “Diabesity” • infants of mothers with diabetes (Type 1) • diabetes/prediabetes in reproductive age women • 5% to 10% of women with GDM develop Type 2 immediately after pregnancy • 35% to 60% of women with GDM develop Type 2 within the 10– 20 years • Among Hispanic women, approximately 50% develop Type 2 within 2 years


Complications and Interventions

Complications in Pregnancy

Complications in First Trimester

Complications in 1 st Trimester • Uncontrolled preexisting DM in first trimester of pregnancy = Maternal hyperglycemia • Miscarriage • Congenital anomalies • Open neural tube defects • Heart defects

Teratogens
 • Preconception counseling • Risk to fetus for")
Interventions in First Trimester (or before) • Preconception counseling • Risk to fetus for congenital malformations highest often before they know they are pregnant • Hgb. A 1 c > 8% risk of miscarriage is 26 times baseline risk • Hgb. A 1 c > 10% confers 25% risk of congenital malformation

Interventions in 1 st Trimester • Diabetes Re-Education Different rules in pregnancy • First trimester • Ultrasound to establish dates • Baseline labs and evaluations • 24 hour urine protein, preeclampsia labs, TSH, maternal echo, ophthalmology exam • Start daily low dose aspirin between 12 -16 weeks of pregnancy and continue until delivery

Complications in 2 nd and 3 rd Trimester

Complications in 2 nd and 3 rd Trimester • Uncontrolled DM in second and third trimester of pregnancy = Hyperglycemia and Hyperinsulinemia • • • Premature delivery Preeclampsia Stillbirth Macrosomia Shoulder dystocia Operative delivery Maternal or fetal trauma NICU admission Childhood obesity and diabetes mellitus

Fractured clavicle Erb’s Palsy

: 249 -254. doi: 10. 1001/archpedi. 152. 3. 249")
Arch Pediatr Adolesc Med. 1998; 152(3): 249 -254. doi: 10. 1001/archpedi. 152. 3. 249

Interventions in 2 nd and 3 rd Trimester • Strict blood glucose control • Fasting < 95 mg/dl (I prefer <90 mg/dl) • Pre-prandial <100 mg/dl • Post-prandial <120 mg/dl • Bedtime <100 mg/dl • Close follow-up • Nutritional Counseling and Diabetes Self-Management Education • Serial ultrasounds for anatomic survey and then for growth q 4 weeks • Antenatal testing • Delivery timing

Antepartum Testing • Ultrasounds • For dating • To assess for congenital malformations • Growth assessment • Fetal echocardiogram • Non-Stress Tests – begun generally between 32 -34 weeks, but individualized based on underlying risk

Delivery Timing • Balance the risk of IUFD with risks of preterm birth • Poorly controlled – delivery between 37 -39 weeks • Evidence of compromise/elevated risk profile – consider delivery before 39 weeks • Well-controlled, A 1’s may go to EDC • Expectant management beyond is not recommended

PREGNANCY = TEACHABLE MOMENT

Questions?
- Slides: 31