Development of the Cardiovascular System Contents Establishment of

Development of the Cardiovascular System

Contents Ø Establishment of the primordial cardiovascular system Ø Development of the heart Ø Blood circulation of fetus and circulatory changes after birth Ø Congenital defects of the cardiovascular system

Establishment of the Primordial Cardiovascular System

l Yolk sac mesenchyme cells blood islands Central C Peripheral C Primitive Blood cell Endothelial C Blood C Endothelial tubule Endothelial tube meshwork

l Endothelial tube network appears in chorion and body stalk, and connect to vitelline circulation. l By the 18 -20 th days, endothelial tube network appears in intraembryonic mesenchyma to form intraembryonic endothelial tube network.

l By the end of 3 rd week, intraembryonic and extraembryonic endothelial tube networks connect to each other. l Endothelial tube networks fuse or disappear to form primordial cardiovascular system.

Primitive heart cardiac tubes 20 d 4 w End of 4 w ① cardiac tube: 2 tubes 1 tube primitive heart ② arteries ③ veins

Dorsal A 20 d 4 w ① cardiac tube ② arteries ③ veins Aortic arches Dorsal aorta End of 4 w Vitelline A Umbilical A 2 dorsal A 1 , many branches Few pairs of vitelline A 1 pair of umbilical A 6 pairs of aortic arches

Anterior cardinal V Posterior cardinal V 20 d 4 w ① cardiac tube ② arteries ③ veins Vitelline V Common cardinal V Umbilical V End of 4 w 1 pair of anterior cardinal V 1 pair of posterior cardinal V 1 pair of vitelline V 1 pair of umbilical V Common cardinal V

vitelline, umbilical and embryonic circulation.

Development of the Heart • Development of the cardiac tube • Morphogenesis of the heart • Partitioning of heart chambers

n Development of the cardiac tube l Cardiogenic area is anterior to the oropharyngeal membrane. ropharyngeal

Pericardial cavity 18~19 th day cardiaogenic plate A. A cavity appears in the cardiogenic area --pericardial cavity B. Ventral of the cavity is cardiaogenic cords --cardiaogenic plate

Pericardial cavity 20 th day cardiac tube C. cardiaogenic plate becomes hollow --cardiac tube

cardiac tube Pericardial cavity 22 nd day D. Cephalic folding: Pericardial cavity: dorsal → ventral Cardiac tube: ventral → dorsal

E. Lateral folding: 2 cardiac tubes → single cardiac tube. F. The tube remains attached to the dorsal side of the pericardial cavity by the dorsal mesocardium.

Transverse sinus Cephalic end Caudal end cardiac tube Pericardial cavity G. The dorsal mesocardium breaks down to form the transverse sinus, which connects both sides of the pericardial cavity. Cephalic end Arteries,Caudal end Veins

n Morphogenesis of the heart Artery end l l Part of the cardiac tubes merged Cardiac tube Cephalic end A Caudal end V Vein end The 21 st d

l Cardiac tubes almost merged l Three expansions bulbus cordis Bulbus cordis ventricle Ventricle Atrium atrium The 22 nd d

l The 4 th expansion, the sinus venosus appears l truncus arteriosus The truncus arteriosus bulbus cordis appears l The bulbus cordis and ventricle grow faster than atrium sinus venosus other regions, the cardiac tube starts to bend. The 23 rd d

truncus arteriosus sinus venosus l Form a ‘U’ like structure, the cardiac loop-bulboventricular loop.

l The bulboventricular loop continues to grow and bend: • Atrium shifts in dorsocranial direction and Aortic arches atrium bulges laterally on each side of bulbus. • ventricle Sinus venousus located at caudal portion of atrium The 35 th d

• Primary ventricle develop into the left ventricle. • The bulbus cordis proximal portion develops into the right ventricle. • Atrioventricular canal: atrioventricular junction remains narrow. Aortic arches atrium ventricle The 35 th d The normal heart shape was established, but partitioning has not completed.
 u")
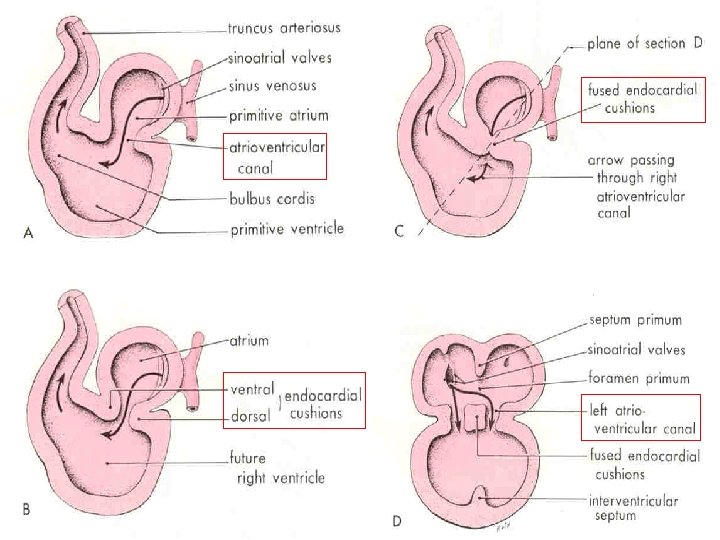
n Partitioning of Heart Chambers (from 27 th day to 37 th day) u Partitioning of atrioventricular canal u Partitioning of the primitive atrium u Partitioning of the primitive ventricle u Division of truncus arteriosus and bulbus cordis

u Partitioning of atrioventricular canal • Endocardiac cushion: • The endocardial cushions grow toward each other and fuse

• Lateral atrioventricular cushion: form atrioventricular valve. Left → bicuspid, right → tricuspid Endocardiac cushion Bicuspid Ttricuspid

u Partitioning of the primitive atrium • Septum primum: a thin sickle-shaped crest appearing from dorsocranial wall of atrium. • Foramen primum: septum primum grows toward the endocardial cushions, leaving an opening between its lower edge and the endocardial cushions Septum primum Foramen primum Endocardiac cushion End of the 4 th w

Small holes Foramen primum Early 5 th w

• Septum secundum Foramen secundum Small holes fuse to form the foramen se- Septum primum cundum, The foramen primum closed. • Septum secundum: another membrane appears on the right of the septum primum. End of the 5 th w

• Septum secundum Foramen ovale : Foramen secundum septum secundum extends downward to Septum primum cover the foramen Foramen ovale secundum, but leaving an opening. • The septum primum covers the foramen ovale, serves as a valve. Early 6 th w

• Before birth, blood can flow from right atrium toward the left atrium • After birth, two septums fuse , the foramen ovale closed complete, and atrium is separated into R and L atria.

u Partitioning of the primitive ventricle • The muscular EC Interventricular septum grows LV up from the floor RV of the ventricle. Interventricular septum The 4 th w

• Interventricular foramen the muscular interven tricular septum keeps EC growing toward endo- Interventricular foramen cardial cushions, but left an opening, called inter ventricular foramen. IV septum End of the 5 th w

• Membranous interventricular septum: Derived from right bulbar ridge, left bulbar ridge and the endocardial cushion closes the interventricular foramen , Membranous interventricular septum endocardial cushions End of the 7 th w

The interventricular septum: muscular partion + membranous portion Left ventricle Pulmonary artery Right ventricle Aorta

u Division of truncus arteriosus and bulbus cordis The 5 th w Truncal ridge Truncus arteriosus Bulbus cordis • Bulbar ridge Two spiral truncal ridges/ bulbar ridges grow from the inner walls of the truncus arteriosus and bulbus cordis.

Aorta Pulmonary artery • Aorticopulmonary septum These ridges twist around each other and fuse to form a spiral aorticopulmonary septum.

• The ridges spiral neatly down the truncus until they reach the ventricles.

• • As the same time, the division of the ventricle is completed. Aorticopulmonary septum divides truncus arteriosus and bulbus cordis into two channels: pulmonary trunk connecting to the right ventricle; aorta connecting to the left ventricle.

Blood circulation of fetus and circulatory changes after birth

Before birth Placental circulation: umbilical A. & V.

n Blood circulation of fetus

n Circulatory changes after birth a. Umbilical A: distal parts becomes into medial umbilical ligament, but proximal portions persist as superior vesical arteries. b. Umbilical V and ducts venousus: constrict and becomes into ligamen-tum teres hepatis and ligamentum venosus c. Ductus arteriosus: constrict and become ligamentum arteriosum d. Foramen ovale closed

Congenital defects of the cardiovascular system
 is a common congenital")
n Atrial septal defect l An atrial septal defect (ASD) is a common congenital heart anomaly. l The most common form of ASD is patent oval foramen. l Consequently there is a mixing of oxygenated and deoxygenated blood.

n Atrial septal defect A. Perforation of valve of ovale foramen B. Excessive resorption of the septum primum C. Inadequate development of the septum secundum. D. B+C 1. Endocardial cushion defect with septum primum defect

n Ventricular septal defect Muscular part of the ventricular septum: sparsely l Membranous part of the ventricular septum defect: commonly Unfused endocardial cushion, bulbar ridge and muscular septum or over absorption of membranous septum l

n Patent ductus arteriosus l Ductus arteriosus fails to be closed after birth. l Isolated or combined with other defects. l Blood will be shunted from the aorta to the lungs, eventually causing irreversible pulmonary hypertension.

n Persistent truncus arteriosus l Aorticopulmonary septal ridges fail to fuse and descend; l Truncus overrides both ventricles; l Accompanied by ventricular septal defect; l Resulting in cyanotic defect.

n Transposition of great vessels Aorticopulmonary septum failing to follow its spiral course and descending straight downward l Aorta originates from right ventricle, pulmonary artery from left l l Usually combined with patent ductus arteriosus

n Tetralogy of Fallot l Unequal division of the truncus and bulbus l A complex of 4 defects: Ø Pulmonary stenosis Ø Overriding aorta Ø Ventricular septal defect Ø Hypertrophy of the right ventricle

Key points l Morphogenesis of the heart l Partitioning of atrioventricular canal, autrium, ventricle, and truncus arteriosus and bulbus cordis Congenital defects of the cardiovascular system( Tetralogy of Fallot ) l

Prepare for Development of Urogenital System
- Slides: 54