Detrusor Sphincter Dyssynergia A Case Study in Integrated

 • Bladder Sphincter Dyssynergia • Voiding dysfunction • symptoms related")











. Percutaneous tibial nerve stimulation (PTNS) efficacy in the treatment")








- Slides: 24
Detrusor Sphincter Dyssynergia: A Case Study in Integrated Care and Management Anthony G Bailes AOMA Graduate School of Integrative Medicine
Detrusor Sphincter Dyssynergia (DSD) • Bladder Sphincter Dyssynergia • Voiding dysfunction • symptoms related to both the storage and emptying phases of the micturition cycle • Storage dysfunction • Emptying dysfunction
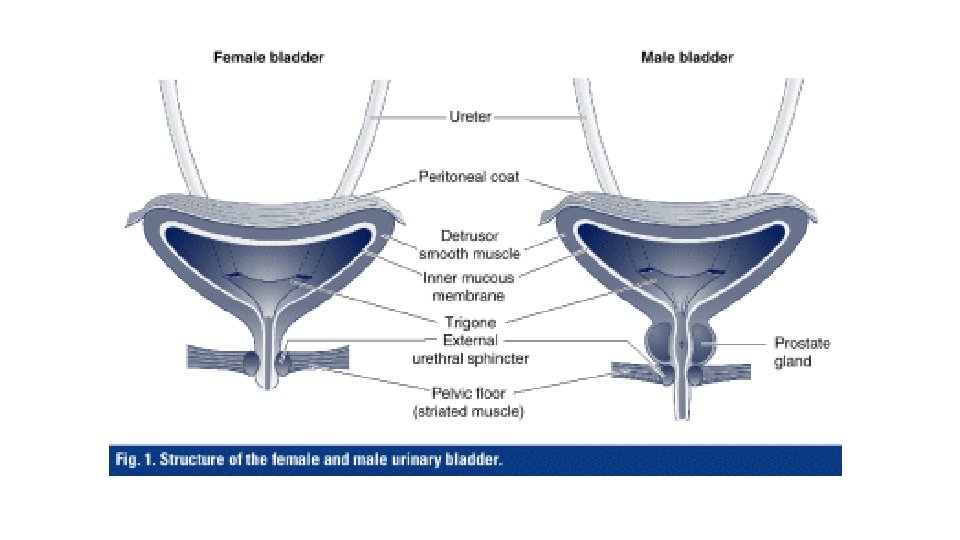
DSD Detrusor muscle • The detrusor muscle remains relaxed to allow the bladder to store urine • Contracts during urination to release urine External sphincter muscle of urethra • Efferent muscle • Receives innervation form the pudendal nerve
Voiding Dysfunction Storage Dysfunction • Frequency • Urge incontinence • Dysuria • Pain Emptying Dysfunction • Hesitancy • Straining • Difficulty initiating • Diminished stream • Incomplete voiding • Urinary retention
Patient Information Social History Demographic Information • 60 years old • Female • Caucasian • Lives alone • Unmarried • No tobacco • No ETOH • No recreational drugs • Limited social interaction • No spiritual/religious affiliation
Medications/Supplements Dietary Habits • Insulin • Aspirin prn • Magnesium glycinate 300 mg QD • Multivitamins • Gluten free • Low sugar • Includes animal proteins Allergies • Sulfas • Floroquinolone (Cipro) Exercise • Walking to tolerance • Physical therapy
Medical Hx • Contracted Hep C in 1982 form surgical blood transfusion • Was not diagnosed until 2008 • Treated with Copegus (ribavirin) and Alinia (nitazoxanide) • Treated for 1 yr w/resolution of sustained virologic response • Diagnosed Type I Diabetes in 2009 • Thought to be a result of undiagnosed/untreated Hep C • Managed w/insulin
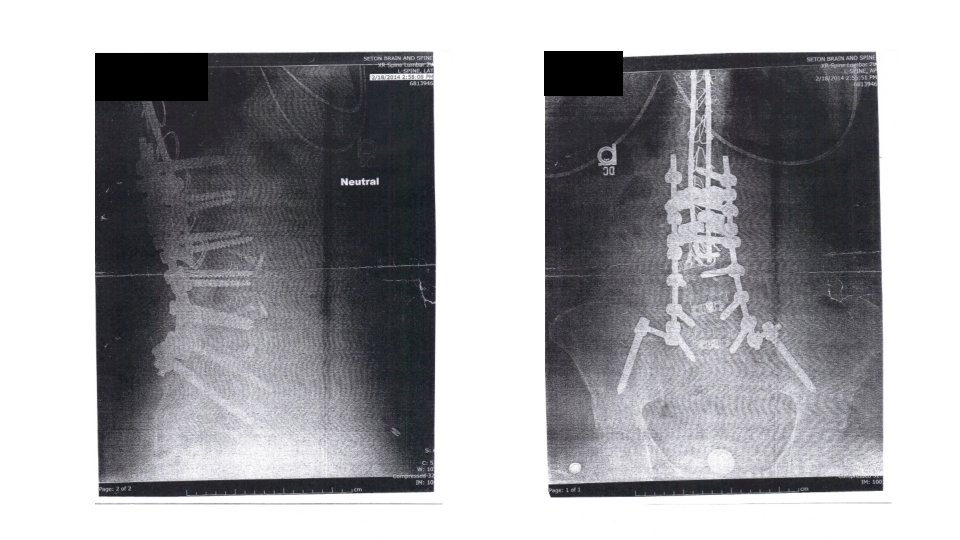
Surgical Hx • 1982: T 8 to S 1 fusion to correct scoliosis • February 2014: T 8 to S 1 fusion to correct long standing complications from 1982 surgery • December 2013, presented in ER with complaints of severe pain • Internal hemorrhaging, spontaneous cerebrospinal fluid leak, and atrial fibrillation • Resulted in 10 hospitalization • During corrective surgery, the pudendal and hypogastric afferent nerves around the bladder were damaged, resulting in DSD
May 5, 2014 – Initial office visit • Vitals within normal ranges • CC: urinary difficulty with dribbling, urgency, and retention • Urgency up to 20 times daily, difficulty initiating urination, interrupted urine flow, and inability to void completely • Recurrent urinary tract infections UTIs • Self-cath three times daily • Secondary complaint: Depression • Tegretol 200 mg BID and Prozac 20 mg QD • Self-discontinued Prozac and Tegretol after 1 month, citing the “inability to function” • Tertiary Complaint: R sided sciatic pattern pain rating 8/10 • Confirmed with seated straight leg raise
• DDX: Qi blockage in Bladder Channel and Organ • TX: Unblock channel and organ Qi • Points: SP 6, 9; Ren 2, 3, 4; ST 36; Yintang, Kidney Gate; BL 23, 27, 28, 39, 52; (R) GB 30, 42; (R) BL 60, 61, 63; (Bilateral) Ashi around PSIS (4 needles) and Ashi lateral hip (1 needle); All points with strong manual manipulation. • Herbs: (patent – unspecified) Shao Yao Gan Cao Tang; 2 pills TID
Follow Up Visits • June 3, 2014 • June 16, 2014 • August 5, 2014 • No significant changes other than reduction in sciatic pain to manageable levels. Initial tx resulted in full bladder evacuation for 1 day, but returned to old pattern. During this period, patient had multiple UTIs and was dx w/Kidney infection. • Antibiotics resolved infection and patient began prophylactic Hiprex (methenamine hippurate) to manage UTIs • No remarkable changes to DSD
August 12, 2014 • DSD symptoms still persisting • Outside research found study on pudendal nerve stimulation for DSD and voiding disorders • Percutaneous Tibial Nerve Stimulation (PTNS) protocol • 12 treatments and reevaluate
• Points: BL 14, 15, 18, 23, 28, 40, 65; PTNS Protocol • Herbs: (patents) Plum Flower Ba Zheng San – 8 pills TID; Plum Flower Jia Wei Xiao Yao San – 8 pills TID • Notes: Patient was instructed to take herbs concurrently with antibiotics. • **PTNS Protocol: Electro acupuncture at SP 5 to SP 6 bilaterally. Stimulated with continuous wave at 20 Hz for 30 minutes (Agrò, E. (2013). Percutaneous tibial nerve stimulation (PTNS) efficacy in the treatment of lower urinary tract dysfunctions: A systematic review. BMC Urology, 13, 61 -61. )
PTNS Protocol Agrò, E. (2013). Percutaneous tibial nerve stimulation (PTNS) efficacy in the treatment of lower urinary tract dysfunctions: A systematic review. BMC Urology, 13, 61 -61. • 2013 Italy • PTNS was found to be effective in 37 -100% of patients with overactive bladder syndrome (OAB) • 41 -100% of patients with non-obstructive urinary retention (NOUR) • 100% of patients with chronic pelvic pain/painful bladder syndrome (CPP/PBS), dysfunctional voiding and patients with neurogenic pathologies • No major complications have been reported
PTNS Protocol • Stimulating the tibial nerve by means of a 34 gauge needle electrode • 4– 5 cm cephalad to the medial malleolus • Continuous wave at frequency of 20 Hz • Stimulation sessions last for 30 minutes • Once a week for 10– 12 weeks • Mechanism of action still remains unclear
August 14, 2014 • Patient reports more complete evacuation after last treatment. • Easier to initiate urination. • Patient reports increased energy, improved bowel movements, and increased appetite. • Patient reports numbness in vaginal wall.
• Points: BL 14, 18, 23, 24, 25, 26, 40, 65; Four Gates; KD 7; Jiaji L 2 through S 1; PTNS Protocol • Herbs: (patents) Plum Flower Ba Zheng San – 8 pills 5 X a day; Plum Flower Zhi Bai Di Huang Wan – 8 pills TID
August 19, 2014 • Patient reports she has been evacuating bladder 100%, verified by urologist with imaging. • Urologist dismissed patient and has taken her off self-catheterization. • No UTI for first time in 7 months. • Numbness in R lower leg, R anterior upper leg, pelvic floor, and vaginal wall. • Although mood has improved, patient is still worried that results are only temporary and is feeling “emotional”.
• Points: BL 13, 24, 25, 26, 40; GB 41; Four Gates; Jiaji L 4 through S 4; (R) PTNS Protocol • Herbs: Continue current Plum Flower Ba Zheng San – 8 pills TID; Plum Flower Jia Wei Xiao Yao San – 8 pills TID
• August 21, 2014 – dx with Interstitial Cystitis • August 28, 2014 • September 1, 2014 – IC controlled with dietary changes • September 4, 2014 • September 9, 2014 – IC resolved, but new dx of UTI. Antibiotics prescribed • September 15, 2014 • September 23, 2014 – IC resolved • September 29, 2014 • October 7, 2014 – UTI cleared
October 21, 2014 • No UTIs since early September • Bladder function maintaining normal with complete evacuation • Emotions stabilized • Patient wishes to consider support for increasing libido and addressing mild vaginal dryness • No other complaints • Patient will schedule follow up treatments as needed
Thank You ? ? ? ’s