Determining the Surgical Risk Stratification in Aortic Stenosis


 � Euro. SCORE")


 LES 50. 87 (33.")

 255— 260")
 255— 260")



 Surgical AVR LES Predicted Observed Leontyev 33")
 Adult Cardiac Surgery Database � Started in 1986 in")














- Slides: 34
Determining the Surgical Risk Stratification in Aortic Stenosis: STS, Euro. SCORE, and “Frailty” Assessments Michael Mack, M. D. Dallas, TX February 21, 2010
DISCLOSURES Michael J. Mack, MD Consulting Fees –Edwards Lifesciences LLC, MAQUET Gmb. H & Co. KG, Medtronic Cardio. Vascular, Inc. I intend to reference unlabeled/ unapproved uses of drugs or devices in my presentation. I intend to reference Percutaneous Heart valves.
Aortic Valve Surgery Predictive Risk Algorithms � STS Euro. SCORE (additive) � Euro. SCORE (logistic) Ambler (UK) Northern New England New York State Providence Health System
Do any of these algorithms accurately predict risk in patients undergoing TAVI ?
LES Mean LES 30 day/ Hosp Mortality <10 10 -20 7. 3% 13. 7% 7. 5% 12. 6% > 20 33% 12. 5%
>90 th Percentile STS 13. 3% (8. 38 -46. 8) LES 50. 87 (33. 47 -93. 32) Observed 18. 75% 15. 63% O/E Ratio 1. 41 0. 31 N= 638
All LES 10 -20 LES >20 n 652 130 52 Observed Mortality 2. 5% 4. 6% 3. 9% LES 8. 46% 13. 9% 28. 5% STS 4. 4% 6. 5% 10. 1%
European Journal of Cardio-thoracic Surgery 37 (2010) 255— 260
European Journal of Cardio-thoracic Surgery 37 (2010) 255— 260
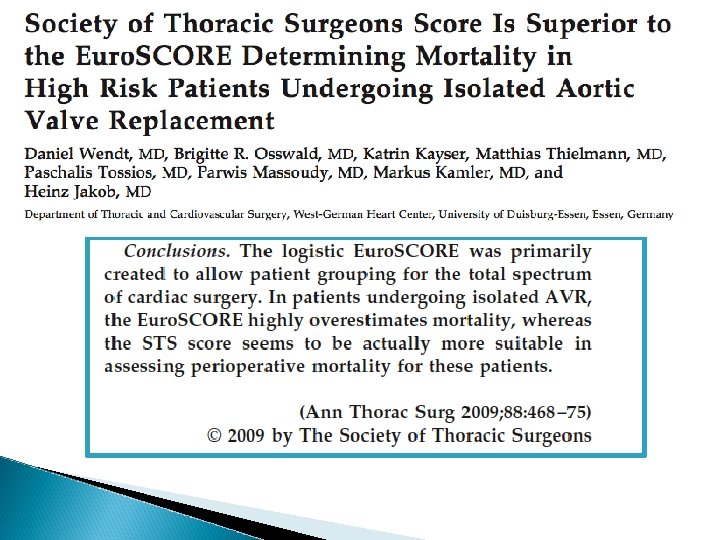
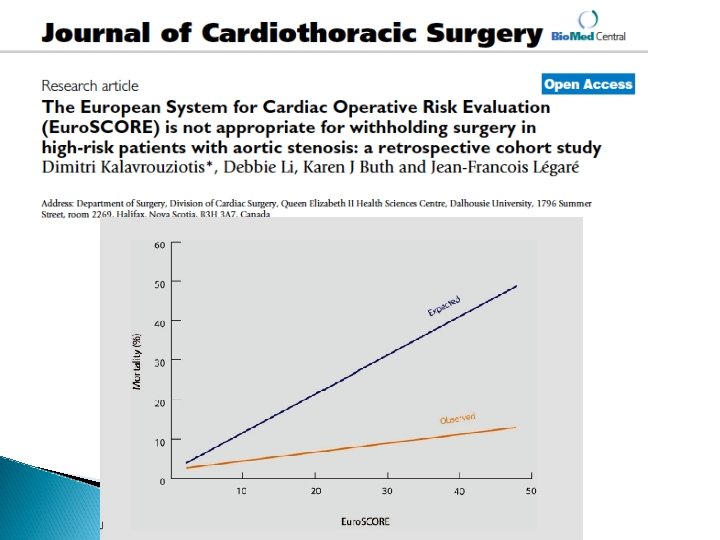
Conclusions: Euro. SCORE appears to be an invalid model in absolute and relative risk prediction for isolated AVR
“Hence, why is the logistic Euro. SCORE, which by all accounts gives the highest values and is the furthest away from observed rates, used almost exclusively by the groups performing PAVI, when it has been conclusively proven to be inaccurate, unreliable and difficult to validate for all groups of patients? ” Manuel Antunes
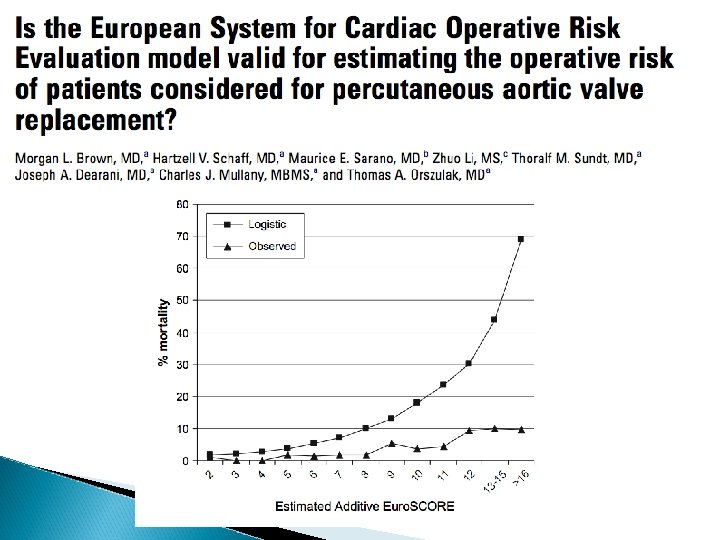
Logistic Euroscore in Surgical AVR n LES Predicted Observed Di. Giammarco 379 9. 4% 5. 2% German Society 6, 305 7. 3% 3. 9% Kalavrouziotis 1, 421 7. 3% 3. 2% LES over predicts AVR mortality by 1. 5 -2 X
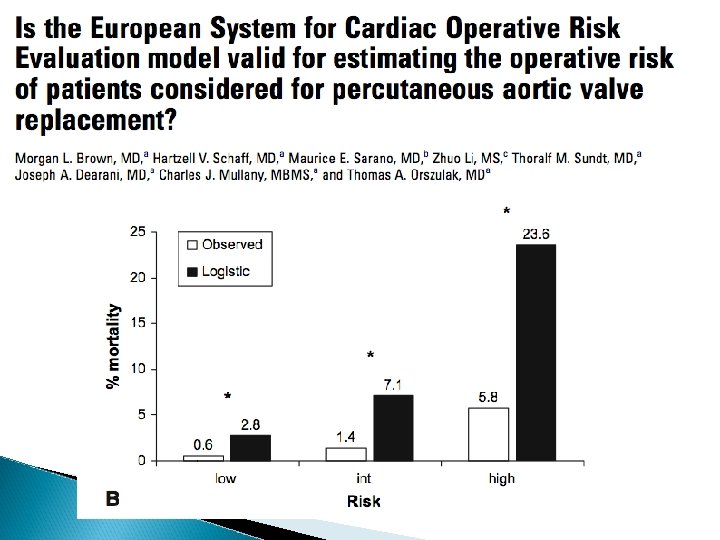
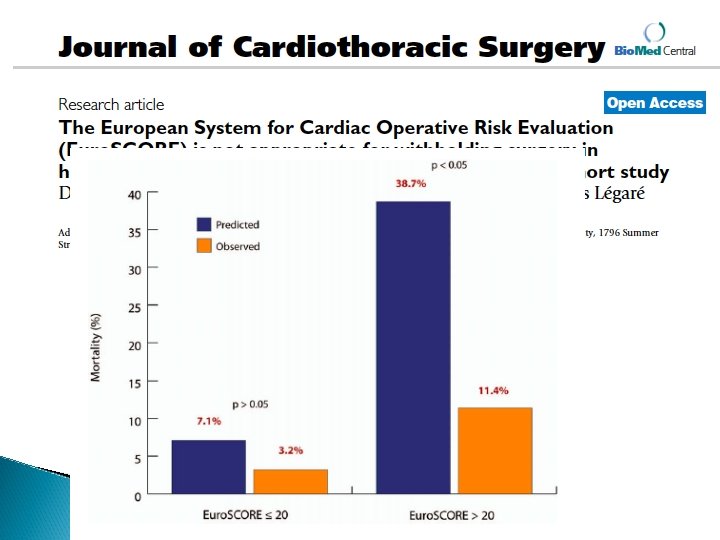
Logistic Euroscore in High Risk (LES >20) Surgical AVR LES Predicted Observed Leontyev 33 12. 5 Brown 23. 6 5. 8 Dewey 50. 8 15. 6 Wendt 28. 5 3. 9 Kalavrouziotis 38. 7% 11. 4% LES over predicts mortality in high risk AVR by 3 -7 X
Society of Thoracic Surgeons (STS) Adult Cardiac Surgery Database � Started in 1986 in response to HCFA (CMS) public reporting of non risk adjusted outcomes of cardiac surgery � Outcomes from 1, 000 centers � 90% of all cardiac surgery providers in U. S. � 3. 6 million procedures � Warehoused and managed by DCRI
Society of Thoracic Surgeons Adult Cardiac Surgery Database � NQF endorsed � Audited � Predicts Mortality and 8 other endpoints � Data shared with 5 major payors � Public reporting in 2010 � Linkage to SS Death Masterfile and CMS � Harmonization with ACC Database
STS Aortic Valve Risk Algorithm � Valves only- 2002 -2006 � N= 67, 292 Aortic Valve Operations � 60% Development Sample/40% Validation � 24 covariates for mortality � C-index 0. 799 for mortality
Euro. SCORE Risk Algorithm � Developed in Europe � All cardiac operations � Additive ◦ 14, 871 patients in 128 centers in 8 countries between Sept and November 1995 � Logistic-LES � 14, 799 patients in 1995 - published 2003
Risk Algorithms Population Analyzed Place Number Operations Type of Operations Covariates for Aortic Valve Mortality LES 1995 STS 2002 -2006 Europe (8 countries) 14, 799 US All cardiac Aortic Valve only 24 12 67, 292
Risk Factors Not Included in Algorithms �Data not collected or too few patients with variables to validate ◦ ◦ ◦ Liver disease Porcelain aorta Frailty Radiation Dementia/Parkinson’s
LES OBSERVED STS
What Does This Mean? LES- the TAVI is better than expected STS- the TAVI is worse than predicted Neither apply since these are different patients (inoperable) and the algorithms aren’t accurate at the extreme risk LES STS OBSERVED
2 Females > 85 years, STS>10 One operable, one NOT !
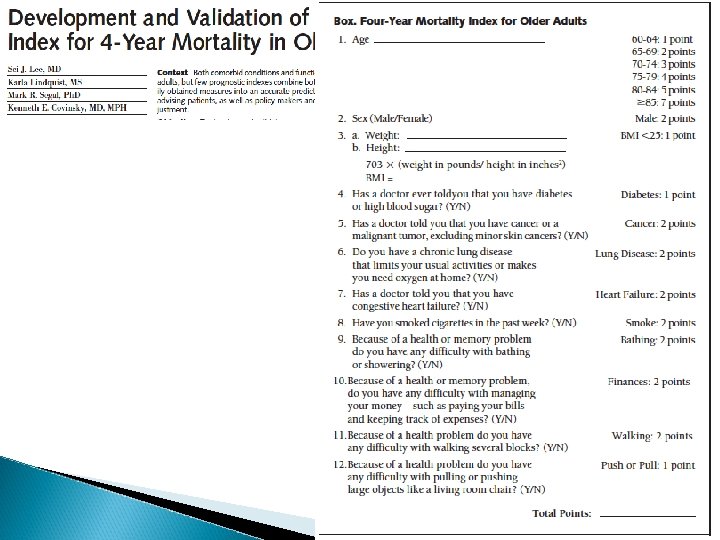
Age Gender Co-Morbidities ◦ ◦ ◦ Diabetes Lung Disease CHF Active Tobacco Use BMI Functional Ability ◦ ◦ Bathing Walking Managing Finances Pushing Large Objects
Score 4 Year Mortality 0 -5 <4% 6 -9 15% 10 -13 42% >14 64%
Summary Both STS and LES are fairly accurate for predictive value in low risk patients STS is more accurate especially in high risk: ◦ ◦ ◦ Larger database- 67 K vs. 14 K More specific – AVR only vs. all cardiac More variables collected- 24 vs. 12 More current- by 10 years US population LES should not be used for predicting risk ◦ If used needs to be with a “recalibration coefficient” of 0. 3 -0. 5
Logistic Euroscore should no longer be used for predicting risk or evaluating outcomes in TAVI patients! � The evidence of inaccuracy in high risk AVR patients is overwhelming � It gives a false sense that outcomes of TAVI are better than they are � There is no valid excuse not to use STS risk algorithm ◦ Most accurate ◦ Online user friendly ◦ Free
Response to RFA-HS-10 -005 ARRA-AHRQ Recovery Act 2009 Limited Competition PROSPECT Studies Building New Clinical Infrastructure for Comparative Effectiveness Research February 16, 2010 � National Disease-based Registry of Valvular Heart Disease � Linkage of: ◦ ◦ STS Adult Cardiac Database ACCF NCDR Database Social Security Death Masterfile Medicare Parts A and B Claims Database � Direct Comparison of Clinical Outcomes of: ◦ Medical Therapy ◦ TAVI ◦ Surgery
The FDA GOT THIS ONE RIGHT 6 YEARS AGO