Determinants of Cardiac Output and Principles of Oxygen


























- Slides: 27
Determinants of Cardiac Output and Principles of Oxygen Delivery Scott V Perryman, MD PGY-III
• Principle of Continuity: • • Conservation of mass in a closed hydraulic system Blood is an incompressible fluid Vascular system is a closed hydraulic loop Vol ejected from left heart = vol received in R heart
Preload • Preload: load imposed on a muscle before the onset of contraction • Muscle stretches to new length • Stretch in cardiac muscle determined by end diastolic volume
Preload
Preload • At bedside, use EDP as surrogate for ventricular preload – i. e. assume EDV = EDP
Preload • How can we measure EDP? Pulmonary Capillary Wedge Pressure
PCWP • How does wedge pressure work? – A balloon catheter is advanced into PA – Balloon at the tip is inflated – Creates static column of blood between catheter tip and left atrium – Thus, pressure at tip = pressure in LA
PCWP • Only valid in Zone 3 of lung where: – Pc > P A • • Catheter tip should be above left atrium Not usually a problem since most flow in Zone 3 Can check with lateral x-ray Will get high respiratory variation if in Zone 1 or 2
Preload • Ventricular function is mostly determined by the diastolic volume • Relationship between EDV/EDP and stroke volume illustrated by ventricular function curves
Ventricular Compliance • Cardiac muscle stretch determined by EDV • Also determined by the wall compliance. • EDP may overestimate the actual EDV or true preload
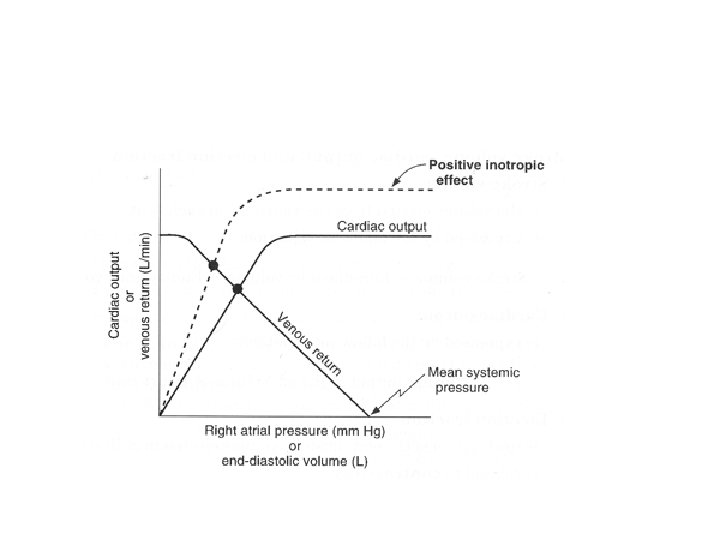
Cardiac Output and EDV
Effect of Heart Rate • With increased heart rate, we get increased C. O…. to a point. • Increased HR also decreases filling time
Contractility • The ability of the cardiac muscle to contract (i. e. the contractile state) • Reflected in ventricular function curves
Afterload • Afterload: Load imposed on a muscle at the onset of contraction • Wall tension in ventricles during systole • Determined by several forces – Pleural Pressure – Vascular compliance – Vascular resistance
Pleural Pressure • Pleural pressures are transmitted across the outer surface of the heart – Negative pressure increases wall tension. Increases afterload – Positive pressure Decreases wall tension. Decreases afterload
Impedence • Impedence = total force opposing flow • Made up of compliance and resistance • Compliance measurement is impractical in the ICU • Rely on resistance
Vascular Resistance • Equations stem from Ohm’s law: V=IR Voltage represented by change in pressure Intensity is the cardiac output • SVR = (MABP – CVP)/CO • PVR = (MPAP – LAP)/CO
Oxygen Transport • Whole blood oxygen content based on: • hemoglobin content and, • dissolved O 2 Described by the equation: Ca. O 2 = (1. 34 x Hb x Sa. O 2) + (0. 003 x Pa. O 2)
Oxygen Content • Assuming 15 g/100 ml Hb concentration • O 2 sat of 99% Hb O 2 = 1. 34 x 15 x 0. 99 = 19. 9 ml/d. L For a Pa. O 2 of 100 Dissolved O 2 = 0. 003 x 100 = 0. 3 ml/d. L
Oxygen Content • Thus, most of blood O 2 content is contained in the Hb • PO 2 is only important if there is an accompanying change in O 2 sat. • Therefore O 2 sat more reliable than PO 2 for assessment of arterial oxygenation
Oxygen Delivery • O 2 delivery = DO 2 = CO x Ca. O 2 • Usually = 520 -570 ml/min/m 2
Oxygen Uptake • A function of: – Cardiac output – Difference in oxygen content b/w arterial and venous blood VO 2 = CO x 1. 34 x Hb (Sa. O 2 – Sv. O 2) 10
Oxygen Extraction Ratio • VO 2/DO 2 x 100 • Ratio of oxygen uptake to delivery • Usually 20 -30% • Uptake is kept constant by increasing extraction when delivery drops.
Critical Oxygen Delivery • Maximal extraction ~ 0. 5 -0. 6 • Once this is reached a decrease in delivery = decrease in uptake • Known as ‘critical oxygen delivery’ • O 2 uptake and aerobic energy production is now supply dependent = dysoxia
Tissue Oxygenation • In order for tissues to engage in aerobic metabolism they need oxygen. • Allows conversion of glucose to ATP • Get 36 moles ATP per mole glucose
Tissue Oxygenation • If not enough oxygen, have anaerobic metabolism • Get 2 moles ATP per mole glucose and production of lactate • Can follow VO 2 or lactate levels