Dermoscopy of acral pigmented lesions Kat Nightingale Associate
















- Slides: 22
Dermoscopy of acral pigmented lesions Kat Nightingale Associate Specialist Bristol Royal Infirmary
Acral melanoma • • ALM – 2 -3% of all melanomas 1. 8 per million person years 36% of melanomas in black skin <1% of melanomas in white skin 5 year survival 80. 3% 10 year survival 67. 5% Feet >hands
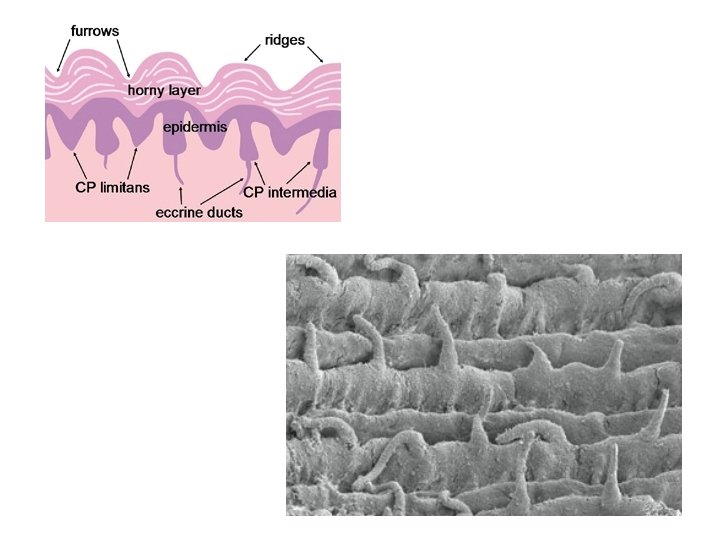
Acral skin structure • • • Thick compact cornified layer Dermatoglyphics – ridges and furrows Absent hair follicles Well developed eccrine ducts 2 types Rete ridges - Crista profunda limitans - furrow Crista profunda intermedia – ridge • Melanocytes distributed mainly in the CPL
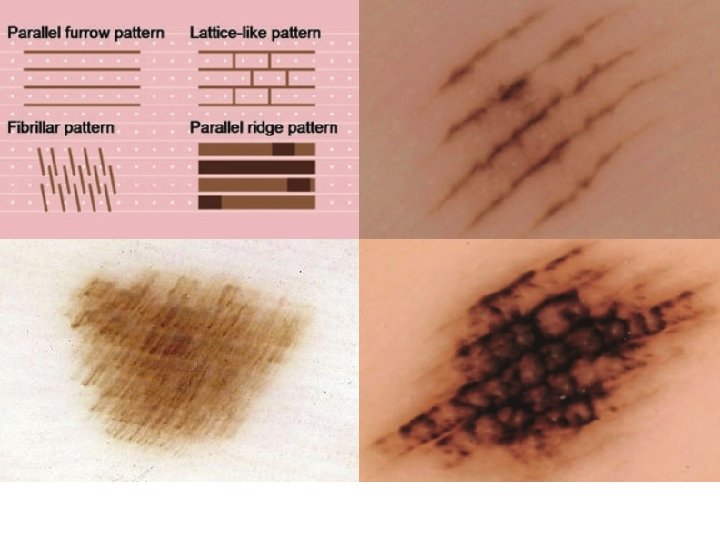
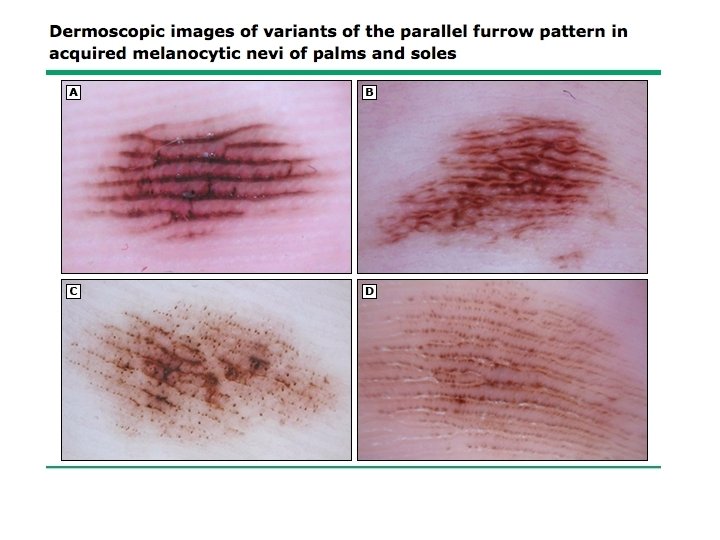
Acral dermoscopy patterns – acquired • • Parallel furrow- 40 -50% Lattice – 15% arch area Fibrillar – 10 -20% Pressure bearing areas Parallel ridge - melanoma Globular Acral reticular Homogenous Transition
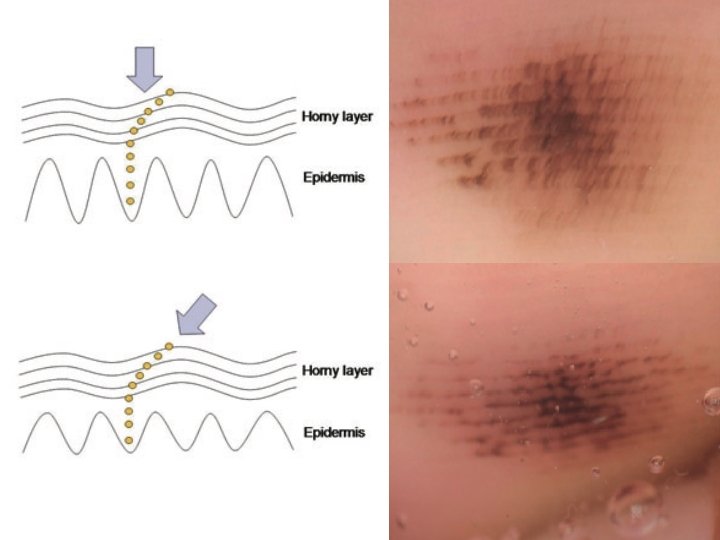
Ink Furrow test
Lattice pattern – 15% Peripheral palms and soles Where typical parallel pattern lost
Benign homogenous, globular, atypical and reticular acral dermoscopy patterns
Transition zone patterns
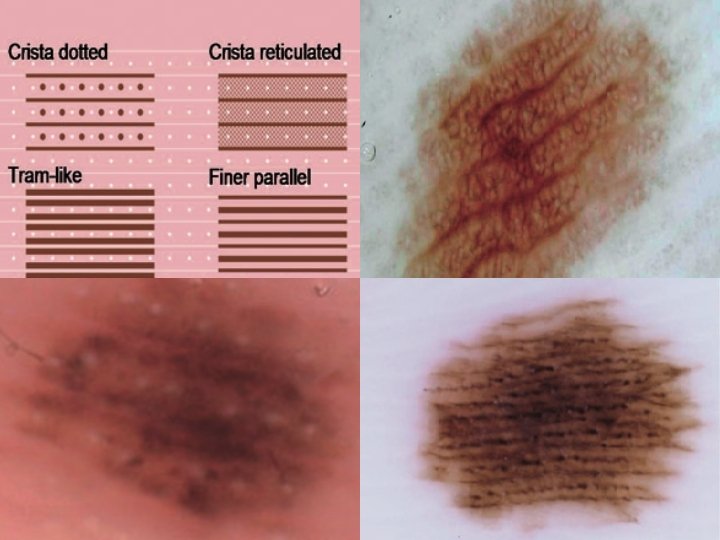
Acral dermsocopy patterns - congenital • • Parallel furrow Crista dotted Peas-in-a-pod – combination of above Crista reticulated
From: Dermoscopic Characteristics of Congenital Melanocytic Nevi Affecting Acral Volar Skin Arch Dermatol. 2011; 147(7): 809 -813. doi: 10. 1001/archdermatol. 2011. 150
Acral melanoma patterns • Parallel ridge- 89% sensitive 99% specific (Significance of dermoscopic patterns in detecting malignant melanoma on acral volar skin: results of a multicenter study in Japan. Saida T, Miyazaki A, Oguchi S, Ishihara Y, Yamazaki Y, Murase S, Yoshikawa S, Tsuchida T, Kawabata Y, Tamaki K Arch Dermatol. 2004 Oct; 140(10): 1233 -8. ) • Multicomponent - irregular diffuse pigmentation, abrupt edges, serrated pattern, peripheral irregular dots and globules, and/or blue-white veil. • Advanced- changes similar to non-acral skin
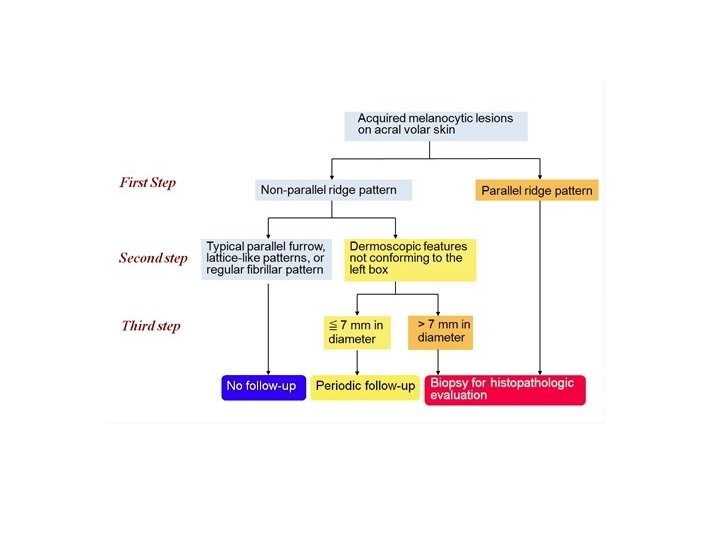
The 3 -step dermoscopic algorithm • Step 1 – The lesion is examined for the presence of the parallel ridge pattern. If the parallel ridge pattern is found in any part of the lesion, the lesion should be biopsied regardless of the size. If the lesion does not show the parallel ridge pattern, proceed to Step 2. • ●Step 2 – The lesion is examined for the presence of one or an orderly combination of the typical benign dermoscopic patterns (ie, typical parallel furrow pattern, typical lattice-like pattern, regular fibrillar pattern). If the lesion shows one or a combination of two or three typical benign patterns, further dermoscopic follow-up is not needed. If the lesion shows equivocal dermoscopic features (ie, absence of any typical/regular patterns) proceed to Step 3. • ●Step 3 – The maximum diameter of lesions that do not show typical benign patterns is measured. Lesions >7 mm should be excised or biopsied for histopathologic evaluation. Lesions ≤ 7 mm should be monitored clinically and dermoscopically at three- to six-month intervals.
References • Saida T, Miyazaki A, Oguchi S, Ishihara Y, Yamazaki Y, Murase S, Yoshikawa S, Tsuchida T, Kawabata Y, Tamaki K: Significance of dermoscopic patterns in detecting malignant melanoma on acral volar skin: results of a multicenter study in Japan. Arch Dermatol 2004, 140: 1233 -1238. • Altamura D, Altobelli E, Micantonio T, Piccolo D, Fargnoli MC, Peris K: Dermoscopic patterns of acral melanocytic nevi and melanomas in a white population in central Italy. Arch Dermatol 2006, 142: 1123 -1128. Malvehy J, Puig S: Dermoscopic patterns of benign volar melanocytic lesions in patients with atypical mole syndrome. Arch Dermatol 2004, 140: 538 -544. Miyazaki A, Saida T, Koga H, Oguchi S, Suzuki T, Tsuchida T: Anatomical And histopathological correlates of the dermoscopic patterns seen in melanocytic nevi on the sole: a retrospective study. J Am Acad Dermatol 2005, 53: 230206. • •