Dermatology Update Laura Manning Inflammatory lesions vs Tumours

 Psoriasis")






")
")

")
")


")










 Look for grey")
 Acral Melanoma (Parallel ridge pattern)")





- Slides: 38
Dermatology Update Laura Manning
Inflammatory lesions vs Tumours Multiple lesions consider inflammatory conditions Eczema Seborrhoeic dermatitis (SD) Psoriasis Lichen planus (LP) Scabies Single lesions consider tumours Actinic keratosis (AK) Solar keratosis (SK) Squamous Cell carcinoma (SCC) Basal Cell carcinoma (BCC) Malignant melanoma (MM)
Discoid Eczema
Eczema update We all know what eczema looks like Treatment failure Steroid ladder Emollients +++ Steroid phobia MILD – 1% Hydrocortisone MODERATE – Eumovate - (Clobetasone- think One is low strength) POTENT – Betnovate (min strength needed for LP or hand eczema) SUPER POTENT - Dermovate (Clobetasol- think Sol like sun is high strength) Step down Topical Corticosteroids (TCS) 7 d bd, then 7 d od 14 d bd, then 14 d od
Seborrhoeic Dermatitis
Seborrhoeic Dermatitis Cradle cap in babies Itchy flaky scalp Cocois under shower cap occlusion overnight Ketoconazole shampoo Red scaly patches in nasolabial folds Don’t treat unless bad Miconazole without TCS (Perioral dermatitis) 1 w oral itraconazole if bad (can also be used for Pitiryasis versicolor) Think HIV in uncontrolled SD
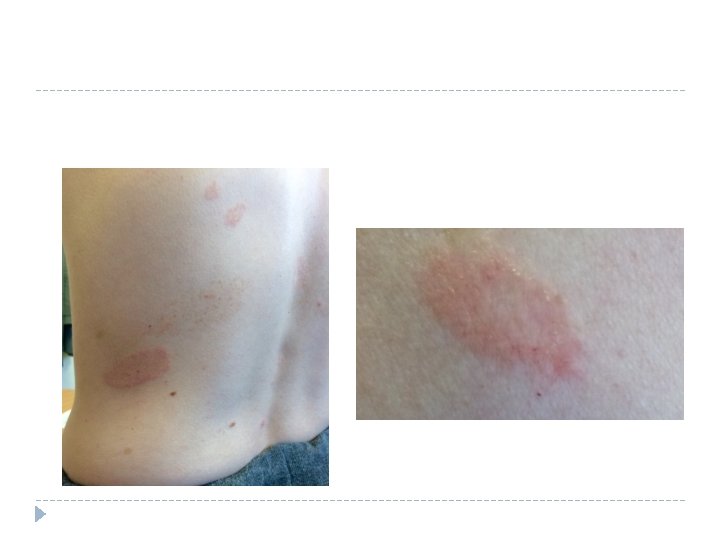
Guttate psoriasis
Psoriasis update Large plaque psoriasis treatment Emollients Dovobet gel od-bd for up to 4 weeks Step down to Dovonex ointment od-bd Cocois or Diprosalic under shower cap occlusion overnight Consider psoriatic arthritis if small joint pain/swelling Manage comorbidities: depression, obesity, CVD risks Small plaque psoriasis treatment Guttate psoriasis seen in young people after Strep throat May resolve in weeks without treatment Can try emollient and dovobet. Refer for Light Treatment if widespread
LP(Buccal Wickham’s striae seen in 50% of cases)
LP (Nail involvement in 10% of cases, usually linear ridges)
LP purple flat-topped plaques/papules
LP Koebner’s phenomenon (LP, psoriasis and vitiligo can occur in scars)
LP Close up of Wickham’s striae (fine white network of lines)
Lichen planus update Purple and itchy- think LP LP treatment Potent or Super Potent TCS Likely to need extended courses of treatment 50% clear in 9 m, 85% in 18 m Consider referral to Dermatology for oral treatment if widespread or troublesome
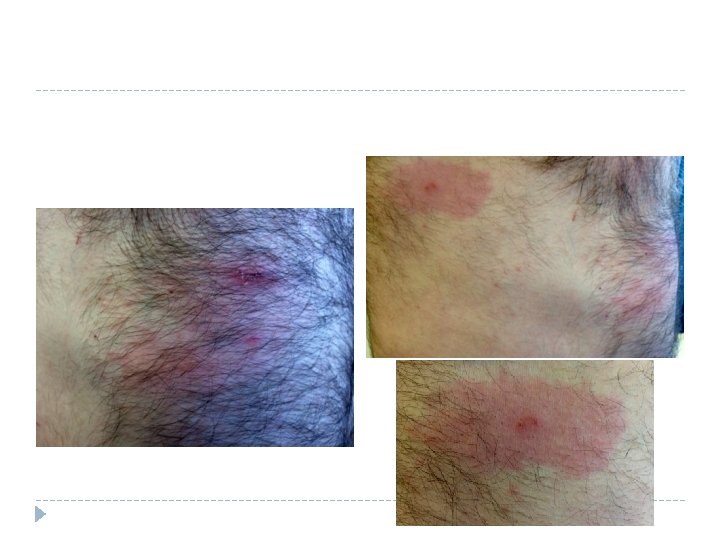
Predominant itch ΔΔ of very itchy rashes LP Dermatitis herpetiformis ( blisters on elbows, check coeliac screen) Scabies (airplane sign)
Actinic keratosis (Solar keratosis)
AK update AK is flat, sandpapery areas on sun-exposed regions Close up they have a red (strawberry) pseudonetwork If they become sore, bleed, or raised up, consider SCC Treatment of AK to avoid 10% risk of malignant conversion to SCC (always emollient and suncream) MILDEST: Solaraze – diclofenac 3% gel – for field changes, up to 12 w MODERATE: Efudix – 5% 5 fluouracil – for individual AK, bd up to 4 w STRONG: Picato – Ingenuol mebutate- for individual AK, 3 d only, expect strong local skin response, resolution within 2 w
BCC can be hard to distinguish from Sebaceous hyperplasia without dermoscopy BCC and close up (usually single) Sebaceous hyperplasia and close up (usually multiple)
Non-healing pink plaques May be treated too long as discoid eczema/psoriasis/fungal infections Bowen’s Disease (superficial SCC) Superficial BCC
Melanoma update The Ugly Duckling Close ups
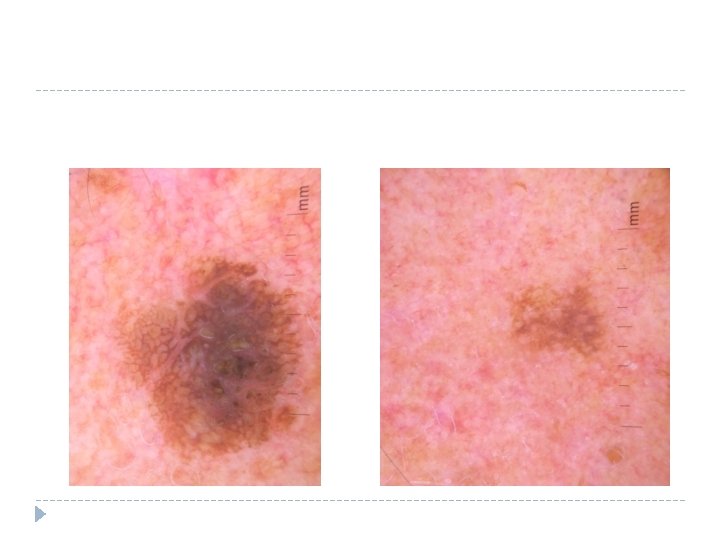
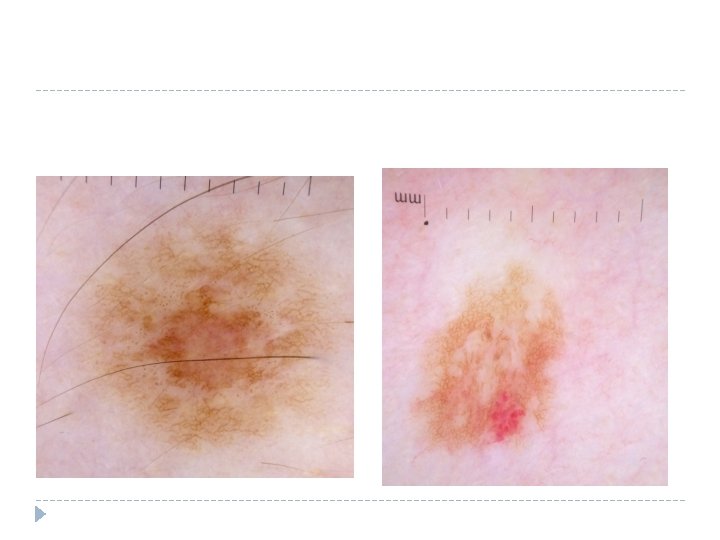
Brown and Pink – make you think! Worry about brown and pink in the same lesion Close up of superficial spreading melanoma with obvious asymmetry, border irregularity, and colour mix
Blue and Black – wish yourself back! Nodular melanoma Blue and black in the same lesion (very worrying as sign of invasion to several skin levels)
ABCDEFG clinical algorithm for melanoma A – Asymmetry B – Border irregularity C – Colour (more than 2) D – Diameter (>6 mm) E – Evolution (recent change) EFG sometimes have a different meaning to catch advanced nodular melanoma E – Elevated F – Firm G - Growth
3 Point Dermoscopy Checklist for Melanoma Asymmetry Atypical pigment network Blue white structures Presence of 2 or more suspicious for melanoma
Solitary pink nodule – think amelanotic melanoma Amelanotic nodular melanoma Don’t bring nodules back for review, worsens prognosis They can look like pyogenic granuloma which is why all of these should be sent 2 WW
Halo naevi are fine in teens NOT older adults Halo naevus Her other naevus types
Facial naevi in adults are NOT flat Lentigo maligna (facial melanoma) Look for grey Solar Lentigo or Solar Keratosis (both benign) Multiple lesions on sun-damaged skin
Acral lesions Acral Naevus (Parallel furrow pattern) Acral Melanoma (Parallel ridge pattern)
Nail lesions Nail haemorrhage Nail melanoma
Miscellaneous lesions Quiz
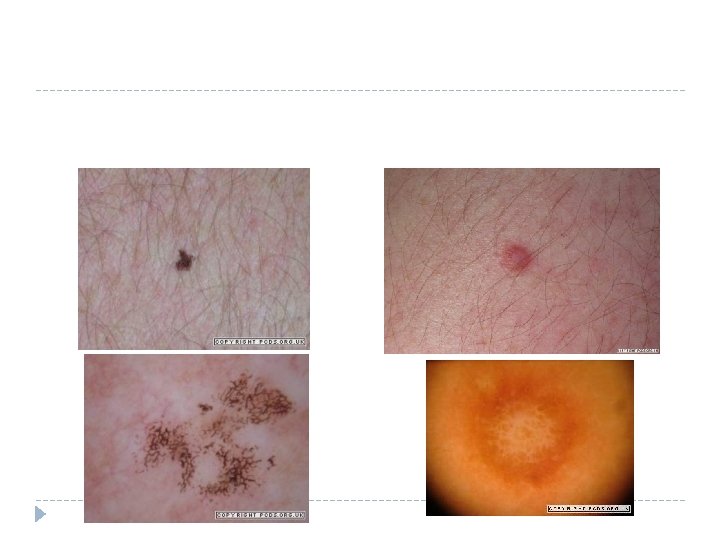
Match the benign lesion to the name/description: Dermatofibroma Broken up black network on sun-damaged skin Ink spot lentigo Dimples on pinch test Seborrhoeic keratosis Umbilicated pearly papule Molluscum Symmetrical globules or network of pigment Naevus Multiple white milia and brown comedones
Send for dermatoscope review SINGLE pink nodules or non-healing plaques FLAT Brown lesions on face, nails, palms, soles
Key learning for itchy rashes Consider LP in purple itchy rashes Treat eczema with stronger and longer steroids