Dermatology for Phototherapists Skin conditions that can be

Dermatology for Phototherapists

Skin conditions that can be treated with phototherapy � Psoriasis � Eczema � Polymorphic � Vitiligo � Pruritis Light Eruption (PLE)

Psoriasis � Affects 2 -4% of the population � Male and female equally � Peaks around age of 15 -25 and 50 -60 but can occur at any age � It is not infectious � It does not scar but can change pigment either paler or darker skin that fades in a few months. � May be inherited in about 1/3 or patients.

Changes in skin with psoriasis � Inflammatory condition � Inflammatory process ultimately triggers the epidermis to develop much more rapidly than normal. � Normally skin cells take 3 -4 weeks to mature but in psoriasis they take 3 -4 days and the immature cells shed very easily.

Chronic plaque psoriasis � The most common type of psoriasis � Plaques are red or pink with silver white scales � Often symmetrical pattern � Common areas are knees, elbows, trunk, lower back and sacrum but can be anywhere.

Guttate Psoriasis � Small plaques scattered over trunk and limbs. � Often affects young adults � Acute and frequently associated with a streptococcal throat infection � Responds well to phototherapy

Nail Psoriasis � Half of all psoriasis patients have nail psoriasis. � Characterised by pitting, discolouration, separation of the nail from the nail bed and thickening of the nails. � Strong predictor for psoriatic arthritis.

Scalp psoriasis � � � Often the first area to be affected Can extend to the forehead, neck and ears Pink/red plaques of skin can have fine scale or thickened hard scale and widespread erythema. Hair loss can occur but usually will re-grow when condition of scalp improves. Scalp can be very itchy and feel tight. If ears are affected , deafness and ear infections can occur.

Flexural psoriasis � � � Affects skin folds and genital areas. Painful and embarrassing, sometimes the patient will hide these areas. Shiny, smooth skin, less scales. Painful fissures can appear. Flexural psoriasis can be difficult to treat with phototherapy therefore a topical treatment would also be required.

Palmoplanter psoriasis � � � Palms of hands and soles of feet Skin can become very thick and develop painful fissures Debilitating Topical treatments containing salicylic acid or urea, topical steroids and regular emollients can be used Phototherapy can be very effective In some cases systemic therapy is required

Palmoplanter pustulosis � � � Similar to palmoplanter psoriasis Skin becomes very thickened, itchy and painful. Deep fissures form and pustules(small pus filled spots) develop them become brown in colour. The pustules are sterile. Up to 24% of patients can have psoriasis elsewhere on their body. Up to 95% of patients with this condition smoke or are ex smokers. May improve with PUVA, sometimes in conjunction with an oral retinoid.

Generalised Pustular Psoriasis � � � Rare and can be serious Plaques of psoriasis have tiny sterile pustules Can flare rapidly and very unstable form of psoriasis Patient may feel very ill and skin may become erythrodermic requiring hospital admission Phototherapy would not be suitable

Erythrodermic psoriasis � � � Skin becomes very red and covers at least 75% of the body. Symptoms may include: fever, shivering, intense itch, tachycardia, exhaustion, headache, nausea, lack of appetite, muscle weakness, skin and joint pain, extreme oedema. Flu like symptoms. Often requires hospital admission. May require IV fluids (essential loss increases to 3 -4 litres a day). May become hypothermic due to excessive heat loss through skin. Even if the patient’s temperature is elevated they may still need to be incubated. Room should be 30 -32 degrees. Phototherapy would not be suitable.
 � � � 10 -30% of patients with psoriasis will")
Psoriatic Arthritis (Ps. A) � � � 10 -30% of patients with psoriasis will develop Psoriatic Arthritis. 80% of patients with Ps. A have nail changes compared to 20% of psoriasis patients with no Ps. A. Joints affected most commonly are hands, feet, neck, spine and elbows although any joint can be affected. Joints may flare when psoriasis flares and improve when skin improves. Early diagnosis is important for treatment to commence before joint damage occurs.

Psoriasis Care Pathway � � � On first presentation the GP should assess severity, co-morbidities, vascular risk, psychosocial health and provide patient information. If patient shows signs of Ps. A then a rheumatology referral should be made. (simple Ps. A assessment tool) see PEST tool and CASPAR criteria. Topical therapy prescribed to be reassessed after 4 -6 weeks. If responds then for annual GP review. If no response then DLQI and if less than 5 for second topical therapy. If DLQI >5 then for dermatology referral. Reassess second topical therapy after 4 -6 weeks then if no response try a third topical therapy as long as DLQI no more than 5. If patient has guttate psoriasis consider early referral for phototherapy

Topical therapy for use in Primary Care � � � Emollient and soap substitute Vitamin D analogue +- moderate potency topical steroid Coal Tar preparations Dithronal cream as short contact therapy Topical retinoid Dermatology pathways App has guidelines for all forms of psoriasis

Psoriasis treatments for use in secondary care � Topical therapy should be fully explored by the time a psoriasis patient is referred to secondary care. � Phototherapy if no response to topical therapy. � Systemic therapy-ciclosporin, methotrexate, acitretin, fumaric acid esters, hydroxycarbamide � Biologic therapy

Annual review � � Psoriasis is generally lifelong but can vary in severity over time. Psoriasis patients are at increased risk of developing; Ps. A, cardiovascular disease (including diabetes, obesity, hyperlipidaemia, hypertension) anxiety, depression and are more likely to smoke and drink excess alcohol, Crohn’s disease. Annual review should include: DLQI, depression screening, vascular risk screening (BMI, BP, bloods including glucose and lipids), topical therapy review, Ps. A screening Annual review can be done by GP

How does phototherapy work for psoriasis? � In psoriasis, there is an increase in T helper cells (required for an immune response) 1 and 17 and related cytokines (inflammatory mediators) which leads to the increased skin cell production that forms psoriasis plaques

How does phototherapy work cntd � UVB treatment improves the stability of the T cells and reduces the amount of circulating cytokine. � UV therapy also increases cell death in keratinocytes and T cells in the epidermis and the dermis. � This leads to a decrease in skin scaling and inflammation.

What treatments can be used with phototherapy. � There are no set guidelines regarding the use of emollients before phototherapy. � Yellow soft paraffin and salicylic acid should be avoided on the day leading up to treatment. � Medicated topical treatments should be withheld on day of treatment until after treatment unless advised by clinician. � Consistency is important if emollients are applied near to treatment time.

What treatments can be used with phototherapy cntd. � � The patient should have emollients prescribed, preferably an ointment and a cream that the patient prefers. Samples are easily ordered in. Medicated topical treatments that can be used in combination with phototherapy are commonly; topical steroids, coal tars, vitamin D analogue, dithranol and calcineurin inhibitors. The patient should be advised if they have erythema post treatment to avoid using coal tar, protopic or salicylic acid. Systemic treatments that can be used with phototherapy include acitretin, methotrexate, apremilast and fumeric acid esters.

Psoriasis treatment plan

Psoriasis references Dermnet NZ Images- these images have not been altered in any way. http: //creativecommons. org. nz/the-noncommercial-licences/ Scottish Intercollegiate Guidelines Network. 2010 Diagnosis and management of psoriasis and psoriatic arthritis in adults; A national clinical guideline. NHS Quality Improvement Scotland, Edinburgh. Psoriasis and Psoriatic Arthritis Association. 2018 About Psoriatic Arthritis [www. papaa. org/resources/about-psoriatic-arthritis] British Association of Dermatology October 2018 ‘Psoriasis- an overview’. [http: //www. bad. org. uk/shared/get-file. ashx? id=178&itemtype=document] Sobelewski. P, Walecka I, Dopytalska K‘Nail Involvement in Psoriatic Arthritis’ Reumatologia V 55 (3) 2017 p 131 -135 Psoriasis Association November 2017 ‘Psoriasis and treatments’ [https: //www. psoriasis association. org. uk/psoriasis-and-treatments/] Penzer-Hick, R. 2017 Phototherapy for People with Psoriasis, Dermatological Nursing, Vol 16 (2) pp 30 -33. Garibaldinos, T. And Stephen, K. 2011 Phototherapy for dermatological conditions, Dermatological Nursing, Vol 10 (4) pp 30 -37.

Eczema Atopic. Eczema Varicose Eczema Contact Eczema Asteatotic Eczema Seborrhoeic Eczema Pompholyx Eczema Discoid Eczema

Atopic Eczema � Can occur at any age but most commonly in children � 20% of children 8% of adults � Atopy is a group of conditions including eczema, asthma, hayfever and rhinitis. � Anyone with Atopic eczema is at higher risk of having one or more of the other atopic conditions � There is often a family history of atopy.

Atopic Eczema cntd � Filaggrin is a protein in the epidermis that is essential for the skin barrier � 50% of people with atopic eczema have at least one mutated filaggrin gene. This can lead to dry skin and a breakdown of the skin barrier � Reduced presence of fats and oils in the epidermis that make a protective barrier in the skin, water escapes from the skin and irritants and bacteria can get in

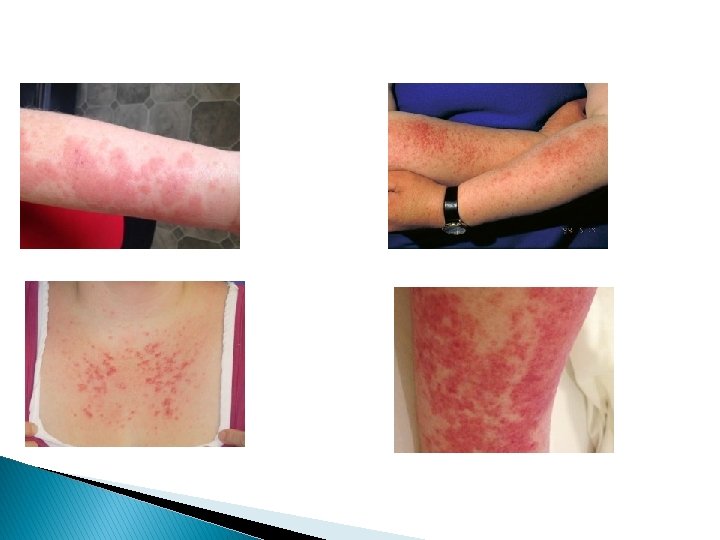
Atopic eczema cntd � Dry, red, itchy and painful skin � If skin in infected it can be weepy, blistered or crusted � Itch can be extreme causing sleep disturbance and emotional distress. � Scratching the skin will cause excoriations, this sometimes happens during sleep � Long term scratching will thicken the skin causing lichenification

Images of atopic eczema

Infection in atopic eczema � � � Eczematous skin is very prone to infection particularly with Staphylococcus bacteria and herpes simplex (cold sore) virus 25% of population have staph present on skin or in nose causing no problems 90% of AE sufferers have Staph present on skin or in nose and broken skin barrier leads to frequent infection. This can be treated with antibiotics

Contact eczema � Does not have the same genetic factors as Atopic Eczema � Mainly present at site of contact with irritant or allergen � 9% of population � Commonly work related � 2 forms- irritant and contact

Irritant contact dermatitis � Caused by contact with everyday things such as soaps, cleaning products, white spirit, solvents, cement, glue, raw food, plants, hair dye

Allergic Contact Eczema � Following contact with a substance, an allergy may develop. � Skin can become dry, painful, red, itchy, weeping and fissured. � Often caused by preservatives, perfumes, nickel, plants, and rubber (latex)

Seborrhoeic Eczema � � � � � Dry, red, flaky , greasy skin Can be itchy May be yellow, crusted flakes of skin Appears around sebaceous glands on upper back, nose, scalp, eyebrows Dandruff is mild seborrhoeic eczema of the scalp May be triggered by stress, illness, hormone changes, soaps, cold weather, medication, tiredness, some diseases Not infectious, not related to diet Infant form is cradle cap or nappy rash Yeast infection, treat with antifungal cream or shampoo and may require mild topical corticosteroid for inflammation

Discoid eczema � � � Disk shaped inflamed round patches of skin Starts as a small group of red spots that cluster together and are very itchy Can be moist and look infected May be a number of patches and usually worse on trunk, arms and legs After time the centre of the circles can have normal skin May also have atopic eczema

Pompholyx Eczema � � � Intensely itchy, watery blisters On sides of fingers, palms of hands and/or soles of feet Starts with a burning, itchy sensation then small blisters that enlarge Can become infected and very painful Stress, heat, sweating can be a factor May be linked with contact eczema and 50% may also have atopic eczema
 � � Most common in women Linked to poor circulation,")
Varicose eczema (stasis eczema) � � Most common in women Linked to poor circulation, varicose veins, phlebitis, cellulitis, leg ulcers, family history, multiple pregnancies, employed in a standing job Increased blood pressure in lower legs, fluid escapes into surrounding tissue causing oedema. Red/brown spots appear on skin that are very itchy, hot could become small blisters Develops into eczema and skin may change colour

Asteatotic Eczema � � � Very dry skin, appears like crazy paving First appears on the shins, then arms, thighs and lower back. Can be Itchy and painful Almost always over 60 years Contributing factors- reduced humidity, hot baths, abrasive cleansing, rough towel drying, underactive thyroid, malnutrition, severe weight loss, certain medications Some patients may have genetic link to icthyosis

How does phototherapy improve eczema � Exact mechanism is unclear � Immunological alteration with T cells � UV interacts with Staphylococci � Increased thickness of epidermal barrier � Of all forms of eczema, phototherapy is most effective for atopic eczema � Hand TL 01 and PUVA can be used for hand dermatitis and UVA 1 for complex cases

Severity of eczema � Clear- normal skin � Mild- areas of dry skin, infrequent itching (with or without redness) � Moderate- areas of dry skin, frequent itching with or without localised thickening or excoriation) � Severe- Widespread areas of dry skin, incessant itching, redness, with or wothout excoriation, skin thickening, bleeding, oozing, cracking, alteration of pigmentation

Other treatments for Atopic Eczema � SIGN Guidelines; management of atopic eczema in primary care � Dermatology Pathways app � Primary Care Dermatology Society for education and diagnostic help http: //www. pcds. org. uk/

Summary of guidelines � All eczema patients should have appropriate emollients prescribed which should be reviewed regularly � Education on application of creams and emollients should be given � Emollients. . . restore barrier function, reduce itch, enhance steroid effect, steroid sparing action
 � Mild, moderate, potent, very potent � Once a day unless")
Topical corticosteroids (TCS) � Mild, moderate, potent, very potent � Once a day unless no response then twice a day for short term � in remission- can be used twice weekly to prevent relapse in chronic conditions � Strength of TCS should match the severity of the eczema � Delicate areas such as face and flexures should be treated with mild or moderate CTS � Topical Tacrolimus (Calcinuerin inhibitors) for age 2 and over, short term, mod- severe cases not controlled by CTS

Severe eczema � Urgent consultation required if patient has: � possible eczema herpeticum (stop treatment and take viral swabs if possible) � Erythrodermic eczema >90% of surface area � Systemically unwell

Systemic therapy for eczema � Phototherapy, � Methotrexate � Azathioprine usually UVB � Mycophenolate � Ciclosporin � Oral mofetil CTS � Biologics- Dupilumab

Eczema treatment plan

Eczema References British Association of Dermatologists, 2017 Atopic eczema , Available at; http: //www. bad. org. uk/shared/gefile. ashx? id=69&itemtype=document Accessed 5 th December 2018 British Association of Dermatologists, 2017 Contact Dermatitis, Available at: http: //www. bad. org. uk/Resource. Listing. aspx? sitesectionid=159&itemid=421 Accessed 5 th December 2018. British Association of Dermatologists, 2016 Discoid Eczema; Available at : http: //www. bad. org. uk/Resource. Listing. aspx? sitesectionid=159&itemid=454 Accessed 6 th December 2018 British Association of Dermatologists, 2018 Seborrhoeic Dermatitis, Available at: http: //www. bad. org. uk/Resource. Listing. aspx? sitesectionid=159&itemid=381 Accessed 6 th December 2018 British Association of Dermatologists, 2016 Venous Eczema: Available at: http: //www. bad. org. uk/Resource. Listing. aspx? sitesectionid=159&itemid=436 Accessed 6 th December 2018 Dermnet NZ Images- these images have not been altered in any way. http: //creativecommons. org. nz/the-noncommercial-licences/ Accessed 6 th December 2018. National Eczema Society, 2018 About Eczema Available at: www. nationaleczema. org, Accessed 6 th December 2018. Scottish Intercollegiate Guidelines Network, 2011 Management of Atopic Eczema in Primary Care: A national clinical guideline. Sign, Edinburgh.
, is a benign, non-life-threatening skin condition")
Polymorphic Light eruption � Polymorphic light eruption (PLE), is a benign, non-life-threatening skin condition that occurs in response to exposure to sunlight and artificial UV light. � Due to its many clinical appearances, it is named polymorphic or polymorphous and the terms are used interchangeably. � PLE is also defined as an idiopathic primary photodermatosis, in which the photosensitiser is unknown.

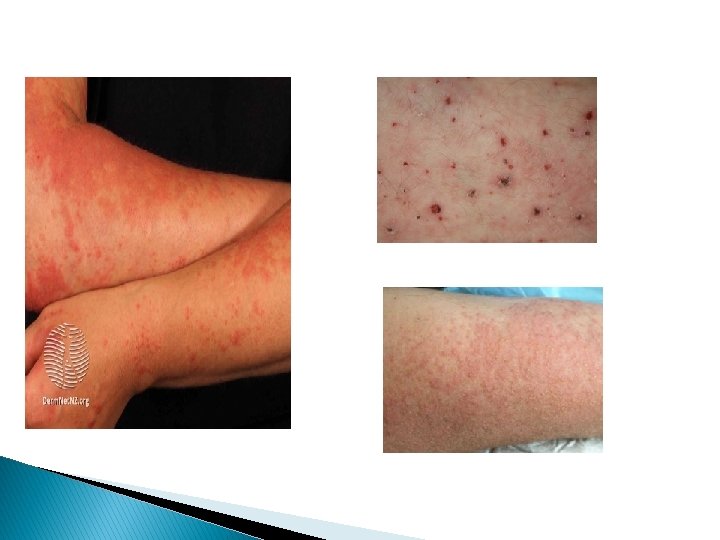
3 main types of PLE � Papular type consists of small erythematous, sometimes urticarial papules on patchy erythematous skin, this is the most common type. � Plaque type consists of sharply defined, infiltrated erythematous plaques, more common on the face � Papular-vesicular type is a combination of papules and vesicles, sometimes bullae

Epidemiology � FHx of PLE: although no candidate genes have been characterised for PLE, a positive family history can be found in up to 50% of the cases. � the prevalence in the general population is 10 to 15% and may even be as high as 40% � PLE is more common in young adults and has a female preponderance with a ratio of 2: 1 femaleto-male. � Most common between the spring and autumn months in the northern hemisphere and at higher altitudes

Clinical presentaion � Typically, the first episode develops in the spring following the first exposure to intense sun, further episodes occur several hours to days following subsequent sun exposure � PLE appears on areas of the skin newly exposed to sunlight such as the visible part of the neckline, backs of hands, arms and legs, and feet, but less commonly the face. It may occur in other parts of the body in some people treated for inflammatory skin diseases with phototherapy. It may be associated with severe itch and burning

� Symmetrical appearance

� Smooth red-topped small papules which merge into plaques, small fluid-filled blisters and less commonly target-shaped lesions may be visible.

� Plaque type

� Appearance varies from person to person but usually reoccurs in same pattern � Occurs annually � Usually symmetrical � Fever, fatigue and headache have been associated with PLE however this is rare

UV Light � � UV irradiation, both from natural sunlight and from artificial UV light sources, is the trigger for PLE. It is provoked by UVA or UVB rays, meaning it can be triggered even by sunlight through glass. UV-A is a major constituent of sunlight, can pass through glass, is relatively resistant to sunscreen and can cause light eruption without sunburn. Artificial UV light sources from tanning units and phototherapy treatment units can also trigger PLE. About three-quarters of sufferers acquire PLE after UV-A exposure only, one-tenth after UV-B exposure only, and the rest after a combination of UV-A and UV-B exposure. [People vary in the amount of sun exposure needed to trigger the rash.

Cause Exact aetiology is unknown but thought to be a delayed hypersensitivity reaction to a compound in the skin that is altered by UV. This impairs T cell function and alters the production of cytokines reducing the normal imunosuppression associated with UV light. � Several factors may be associated with this such as oestrogen, vitamin D, antimicrobials, genetic influence and oxidative stress.

Phototherapy Various regimens of phototherapy have been employed to induce skin desensitisation. Although UVB and UVA have been used with varying degrees of success, they also bear the risk of inducing or aggravating PLE skin lesions. � Annual treatment course to desensitise the skin usually given in winter/ spring � Exposed sites only should be treated � Treatment course of UVB is 3 x weekly or daily for 15 treatments � UVA is 2 x weekly for 5 weeks � The necessity for intense, repeated UV exposures, with the goal of achieving prophylactic protection from clinical symptoms of PLE, might arise in some patients. This increases the long-term risk for skin cancers and photoageing. �

Other treatment � Avoidance of sun exposure � Covering up with densely woven clothing, applying a broad-spectrum, water-resistant semi-opaque sun protection factor (SPF) 50+ before sun exposure and then every two hours thereafter confers some protection. � The application of topical corticosteroids may lessen the redness and itch, and for preventing predictable holiday flare-ups, short courses of oral corticosteroids are sometimes considered.

� Current guidelines suggest that PUVA should be considered if UVB has failed, and it is preferable over systemic treatments such as immunosuppressive therapies or oral steroids.

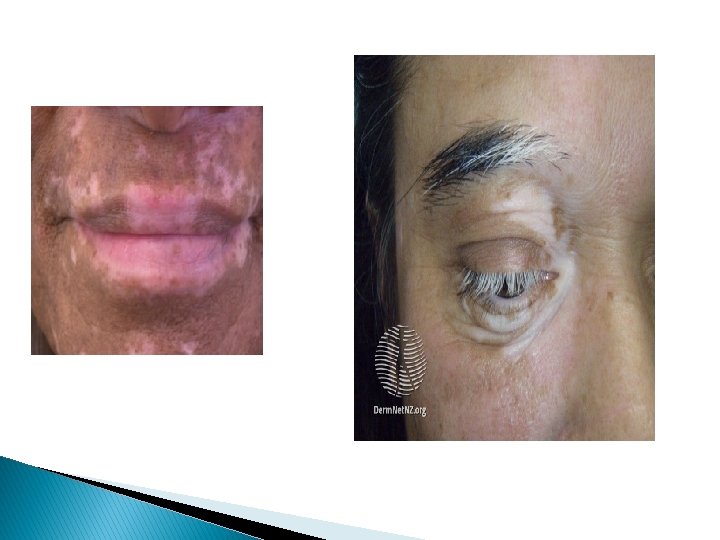
Vitiligo � Vitiligo is an acquired depigmenting disorder of the skin, in which pigment cells (melanocytes) are lost. It presents with welldefined milky-white patches of skin � Vitiligo can affect any part of the body. Complete loss of pigment can affect a single patch of skin, or it may affect multiple patches. � Two types: non segmental (most common) and segmental (dermatomal distribution)

Epidemiology � Vitiligo affects 0. 5– 2% of the population � Occurs in all races however it may be more common in India than elsewhere, with reports of up to 8. 8% of the population affected. � In 50% of sufferers, pigment loss begins before the age of 20, and in about 80% it begins before the age of 30 years. � In 20%, other family members also have vitiligo � Males and females are equally affected

Clinical presentation � Common sites are exposed areas (face, neck, eyelids, nostrils, fingertips and toes), body folds (armpits, groin), nipples, navel, lips and genitalia. � Vitiligo also favours sites of injury (cuts, scrapes), acne, burns � Loss of colour may also affect the hair on the scalp, eyebrows, eyelashes and body. � The retina at the back of the eye may also be affected. However, the colour of the iris does not change.

� The colour of the edge of the white patch can vary. � It is usually the colour of unaffected skin, but sometimes it is hyperpigmented or hypopigmented. � The term trichrome vitiligo is used to describe three shades of skin colour. Very rarely, there are four shades of pigment (white, pale brown, dark brown and normal skin). � Occasionally, each patch of vitiligo has an inflamed red border

� � � The severity of vitiligo differs with each person. There is no way to predict how much pigment an individual will lose or how fast it will be lost. Pigment has occasionally been reported to be lost from the entire skin surface. Extension of vitiligo can occur over a few months, then it stabilises and some spontaneous repigmentation may occur. Brown spots arise from the hair follicles, and the overall size of the white patch may reduce. Cycles of pigment loss followed by periods of stability may continue indefinitely. Light skinned people usually notice the pigment loss during the summer as the contrast between the affected skin and suntanned skin becomes more distinct. Tanning of normal skin makes vitiligo patches appear more obvious. Vitiligo appears more obvious in patients with naturally dark skin.



Cause � Vitiligo is due to the loss or destruction of melanocytes, which are the cells that produce melanin. Melanin determines the colour of skin, hair, and eyes. If melanocytes cannot form melanin or if their number decreases, skin colour becomes progressively lighter. � Vitiligo is thought to be a systemic autoimmune disorder, although this has been disputed for segmental vitiligo where it is thought neurochemical mediators released from nerve endings in the epidermis become toxic to melanocytes � Genetic and environmental factors are thought to be important. � New-onset vitiligo also sometimes follows emotional stress.

Phototherapy � Whole-body or localised broadband or narrowband UVB � Oral, topical, or bathwater phototherapy (PUVA) � Phototherapy is thought to work in vitiligo by two mechanisms: - Immune suppression—preventing the destruction of the melanocytes - Stimulation of cytokines (growth factors) to stimulate repigmentation of the skin

UV treatment � � � Phototherapy is unsuitable for very fair skinned people. The treatment intensity aims for the vitiligo skin to be a light "carnation" pink. If repigmentation is observed, treatment is continued until repigmentation is complete or for a maximum of 1– 2 years. The aim is to cause the treated skin to appear very slightly pink the following day and it is important to avoid burning (red, blistered, peeling, itchy or painful skin), as this could cause the vitiligo to get worse. A meta-analysis included 35 unique studies reporting outcome after phototherapy for generalised vitiligo. A marked or clinically useful response was achieved in 36% after 12 months of NBUVB and in 62% after 12 months of PUVA. Face and neck responded better than the trunk, which responded better than extremities. It was not very effective on hands and feet.

Other treatment � � • Minimise skin injury: wear protective clothing as skin damage may lead to a new patch of vitiligo. Cosmetic camouflage can disguise vitiligo, options include make-up, dyes and stains, dihydroxyacetone-containing fake tan Micropigmentation or tattooing for stable vitiligo. Sun protection - white skin can only burn on exposure to ultraviolet radiation (UVR); it cannot tan and sunburn cause vitiligo to spread Topical corticosteroids can be used for vitiligo on trunk and limbs for up to 3 months. Potent steroids should be avoided on thin-skinned areas of the face (especially eyelids), neck, armpits and groin.

� Calcineurin inhibitors (elidel cream and protopic ointment reduce inflammatory response, can be used for vitiligo affecting eyelids, face, neck, armpits and groin. � Surgery to graft melanocytes � Topical hydroquinone – chemical causing repigmentation if 50% involvement

Guidelines � NICE clinical knowledge summary 2016 � Guidelines for the management of vitiligo: the European dermatology forum consensus 2012 � BAD guidelines for diagnosis and management of vitiligo 2008

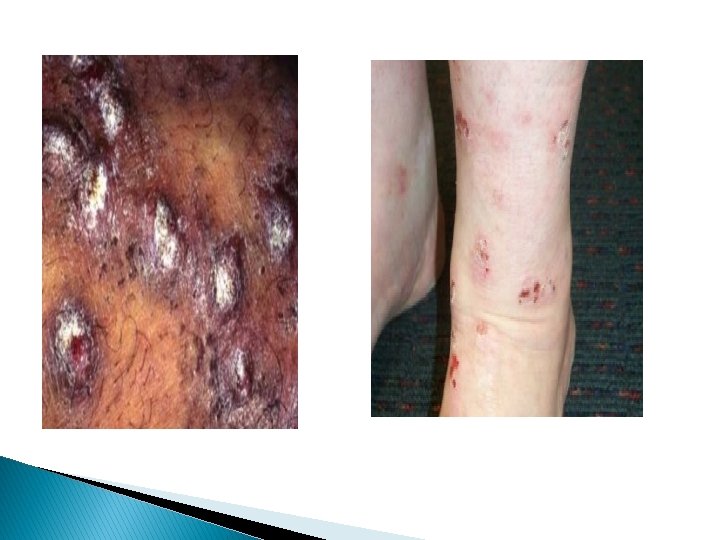
Prurigo � Condition characterised by very itchy lesions � Lesions can be primary or secondary � Primary lesions are dome shaped papules � Secondary lesions are excoriated, scaly or pigmented � Cause is unknown but can be disease related eg atopic eczema, pemphigoid, HIV, diabetes � Two main types – prurigo simplex and nodular prurigo

Prurigo Simplex � Symmetrical � Small domed papules � Mostly outer aspects of limbs and buttocks although may occur anywhere


Nodular prurigo � Hard nodules � Often increased pigmentation � May be ulcerated or crusted � Very resistant to treatment � 80% have personal or family history of atopy

Treatment � Emollients and topical anti itch creams � Topical corticosteroids � Antihistamines � Habit reversal techniques � Phototherapy
- Slides: 82