Dermatological Manifestations of Systemic Diseases By Dr saad

Dermatological Manifestations of Systemic Diseases By Dr saad Al Mohizea

Skin manifestations of Diabetes mellitus: 1. - skin manifestations due to vascular abnormalities: A- wet gangrene of the foot B- Diabetic Bullae C- Diabetic dermopathy” shin spots”: D- Erysiepilas- like erythema
 -Autonomic neuropathy 3. Cutaneous infections: A- Staphylococcus aureus")
• 2. Diabetic neuropathy (peripheral) -Autonomic neuropathy 3. Cutaneous infections: A- Staphylococcus aureus B- Non- clostridial gangrene C- Candidiasis

4. Various skin disorders associated with diabetes mellitus: • A- Diabetic bullae • B- Pruritus • C- Granuloma annulare

Skin problems associated with diabetes mellitus • Necrobiosis lipoidica – Rare, insulin dependent DM – One or more tender yellowish brown patches develop slowly on the lower legs over several months – Round, oval or an irregular shape – The centre of the patch becomes shiny, pale, thinned – Prominent blood vessels (telangiectasia) – Often painless


• D- Necrobiosis lipoidica • Treatment: control of diabetes doesn’t help in disappearance of the lesions. – Intralesional steroids. – Systemic aspirin: 300 mg/day and dipyridamole 75 mg/day. – Nicotineamide – Ticlopidine as antiplatelet – pentoxyfylline. – Preilesional heparin injection - Oral cyclosporin - Photochemotherapy (PUVA)

Hyperlipidemia • Xanthomata – 4 forms : tendinous subcutaneous nodule found in fascia, ligament and extensor tendon of hand, knee and elbow – Planar : yellow, soft, macule or plaque found on the upper eyelids – Tuberous : yellow to reddish nodule at extensor surface of elbows, knees and knuckles – Eruptive : sudden, multiple reddish yellow papule extensor of extremities, buttock


PLANAR XANTHOMA

ERUPTIVE XANTHOMA

Pituitary disorders: • 1. Acromegaly – Skin is oily and wet due to hyperhidrosis with wet hands on hand shaking. – The lower lip is thickened, protruded with wide spaced teeth. – Large and furrowed tongue. – Increased skin pigmentation. – Hirsutism. 2. Hypopitutirism: “Sheehan syndrome”;

– – – – Suprarenal syndrome: Cushing syndrome: endogenous or exogenous Deposition of fat over the clavicles and back of the neck” Buffalo hump” Puffy, rounded erythematosus face with telangiectasia “Moon face” Trunkal obesity with slender wasting limbs. Striae distensae. Hirsutism, acneform rash, androgenetic alopecia. Addisonian-like pigmentation Easy bruising of the skin on simple trauma.

Striae distensae • • • Aetiology: Idiopathic pregnancy: Striae gravidarum Endocrine: cushing Iatrogenic: systemic or potent topical steroids, anabolic drugs or androgens.

• • • Hypocorticism ”Addison, s disease”: Generalized hyperpigmentation that is more prominent in light exposed areas, scars, genitalia, palmar and finger creases, and under the nails. The pigmentation characteristically affects the mucous membranes. Loss of pubic and axillary hair in females. Improvement of acne.

IV- Thyroid diseases: • Hyperthyroidism: • • red, soft, moist and hot skin. • addisonian hyperpigmentation • • • i. e. not affect the mucous membranes. Diffuse thinning of scalp hair Rapid nail growth and onycholysis. Generalised pruritus and urticaria. Palmar erythema and facial flushing. Hyperhidrosis or increased sweating.

• Pretibial myxoedema: appears as small red or skin colored coalescing Nodules • Thyroid acropatchy

Endocrinologic Diseases • Hypothyroidism Macroglossia

• Hypothyroidism: • • • Buffy face with coarse features. The skin is pale, thickened, cold, finely scaling and wrinkled. Coarse sparse hair of the scalp with loss of the lateral third of the eyebrows. Brittle and striated hair. Poor wound healing. Decreased or absent sweating.

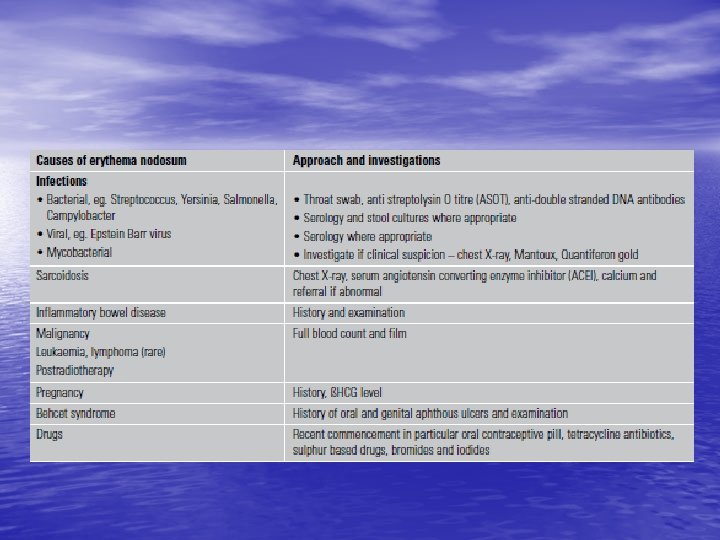
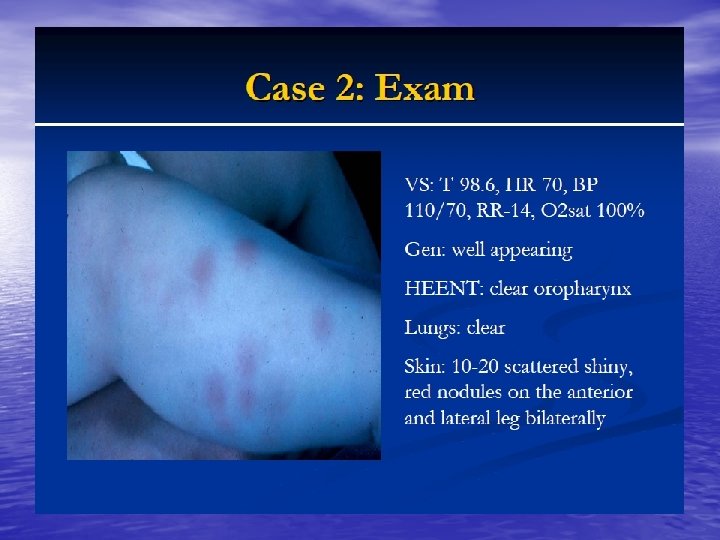
• • • Gastrointestinal tract and the skin Crohn, s disease ”regional ileitis” Perianal abscess and fisulae. Erythema nodosum Erythema multiforme Aphthous-like stomatitis and glossitis. Cutaneous vasculitis. Epidermolysis bullousa acquisita. Metastatic Crohn, s disease as numerous eroded cutaneous granulomas at sites distant from the affected intestine. Pyoderma gangrenosum.

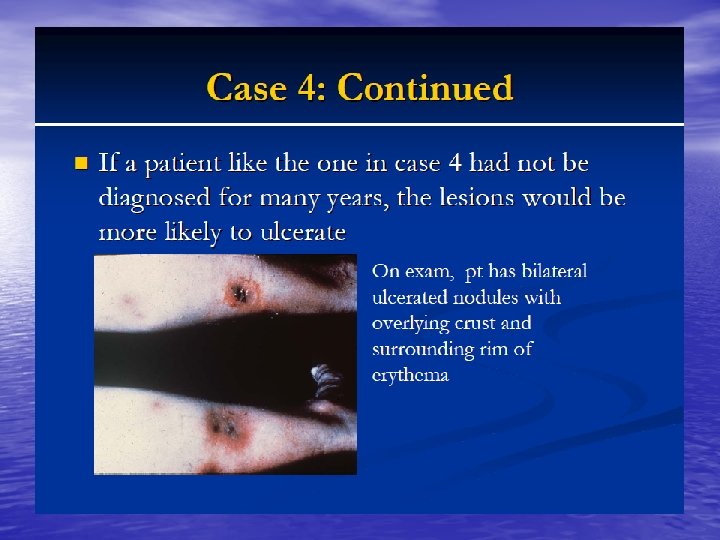
Pyoderma gangrenosum • Aetiology: • Idiopathic in 50% of the cases. • Inflammatory bowel disease • • Crohn, s disease and ulcerative colitis. Connective tissue diseases. Rheumatoid arthritis, SLE or Behc, et disease. Blood disease: Leukemia, multiple myeloma, polycythemia or monoclonal gammopathy. • Treatment: – Dealing with underlying cause. – Systemic steroids in high dose like 60 -80 mg oral prednisolone daily and then reduce gradually. • Azathioprime, Dapsone, or cyclosporine

• Ulcerative colitis: identical to • Malabsorption: specific or nonspecific features. Non- specific features: Pallor, • • • Crohn, s disease but pyoderma gangrenosum and erythema nodosum are more common in ulcerative colitis. dry skin, oedema, acquired icthyosis, Pigmentary disorders, glossitis, mouth ulcers. Specific features due to certain factor deficiency: e. g. – Follicular hyperkeratosis -------- Vit. A deficiency. Echymosis and scurvy --------- Vit. C deficiency. Acrodermatitis enteropathica ----- Zinc deficiency.

• Liver diseases: • Pruritus: generalized itching especially in the presence of biliary obstruction or jaundice. Urticaria especially in infectious hepatitis. Jaundice. Spider naevi: small telangeictatic blood vessels especially on the face and upper chest. Palmar erythema. • • • Diffuse hyperpigmentation.

Thinning of the hair and sometime loss of sexual hair in the axillae and pubic areas. Gynaecomastia. Acneform-lesions. v Porhyria cutanea tarda. v Xanthoma: collection of lipid in the dermal tissue especially in primary biliary cirrhosis.

Behcet disease • Recurrent aphthous oral • • ulcerations more than three times per a year is a must plus two of the following: Genital ulceration or other skin manifestations Erythema-nodosum like lesions, pseudofolliculitis, papulopustular lesions or acneform rash. Eye lesions: anterior or posterior uveitis • Positive pathergy test

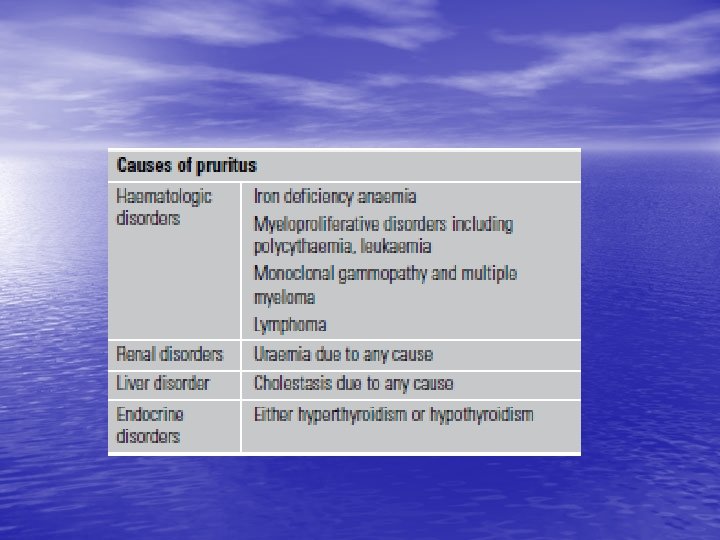
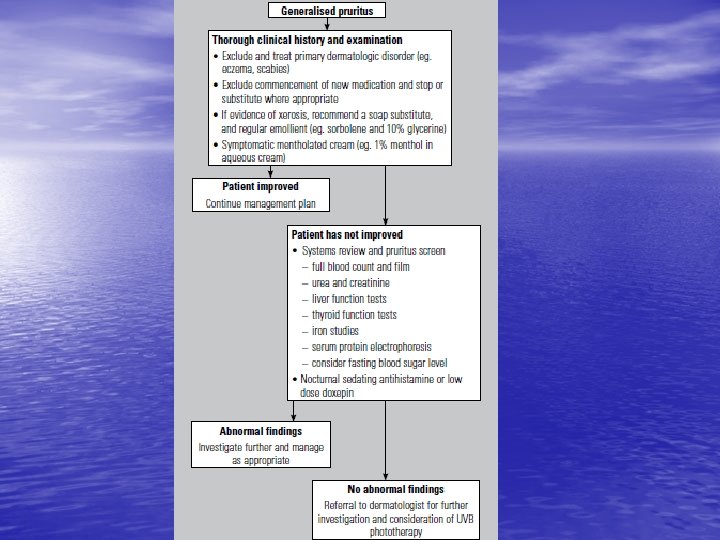
Generalised pruritus • Generalised pruritus in the absence of a rash requires investigation and exclusion of an underlying systemic disorder • it is important to distinguish these from an underlying • primary skin disease such as scabies or eczema

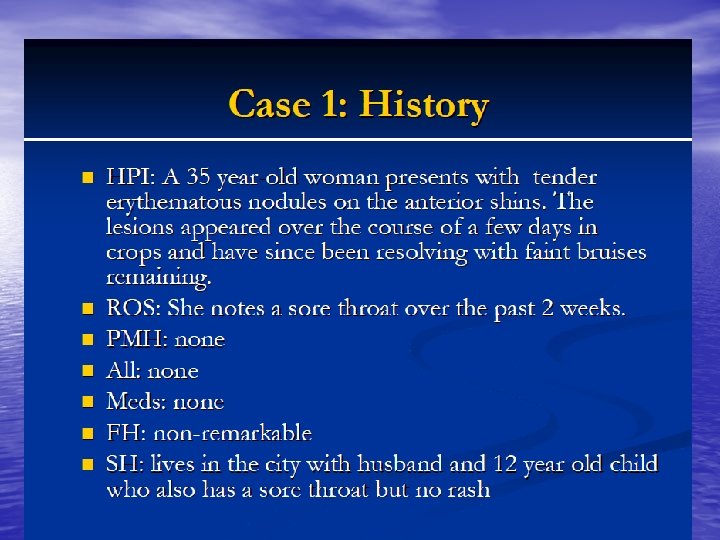
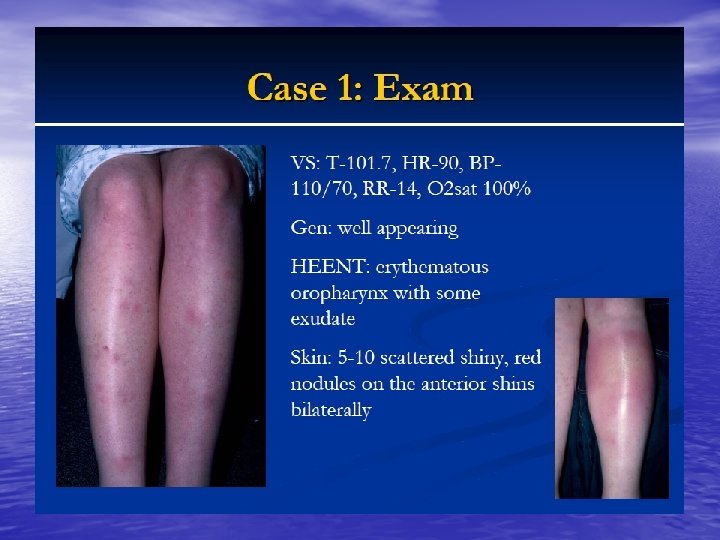
Erythema nodusom

sarcoidosis

DM

Cutaneous markers of internal malignancy • I. Genetically determined syndromes: Gardners syndrome, Howel-Evans syndrome, Torre-Muir syndrome. • II. Skin signs of exposure to carcinogen: e. g. – Nicotine staining, X -ray damage

Paraneoplastic dermatoses • 1. Acanthosis • • • nigricans 2. Dermatomyositis 3. Erythema gyratum repens 4. Erythema nodosum and erythema multiforme

• 5. Acquired icthyosis • 6. Pruritus • 7. Bullous eruptions • 8. Pyoderma gangrenosum • 9. Erythroderma • 10. Flushing of the face • 11. Urticaria

12. Acquired hypertrichosis lanuginosa

• 13. Disseminated herpes zoster • 14. Migratory superficial thrombophlebitis • 15. Hypertrophic osteoarthropathy • and Finger clubbing 16. Tripe palms • 17. The sign of Leser-Telat • 18. Necrolytic migratory erythema • IV. Direct metastases to the skin e. g. Carcinoma of the breast or lymphoma.

Sign of Leser-Trelat • Sudden appearance of multiple seborrheic keratoses • Association with internal malignancy is unproven


• 18. Necrolytic migratory erythema


Nephrogenic fibrosing dermopathy • fibrotic disease of the skin and internal organs that develops in patients with renal insufficiency after exposure to gadoliniumbased contrast agents. It is similar to, yet distinct from, scleroderma. • pain and pruritus. • Most patients are on hemodialysis or peritoneal dialysis or have had a renal transplantation.


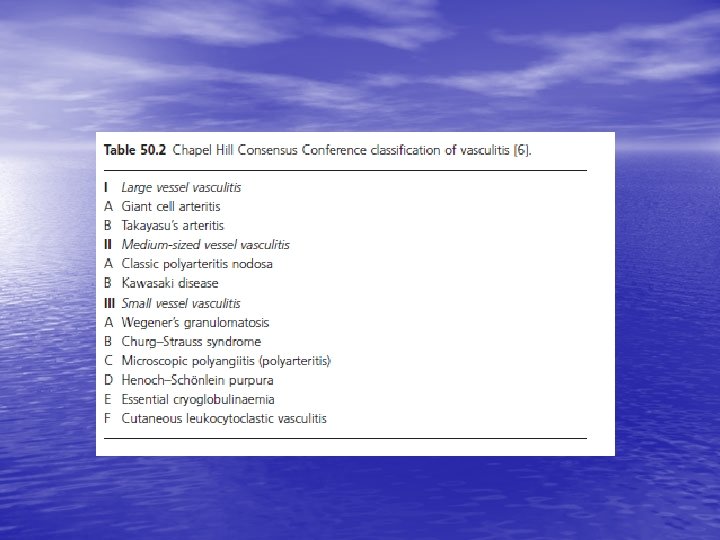
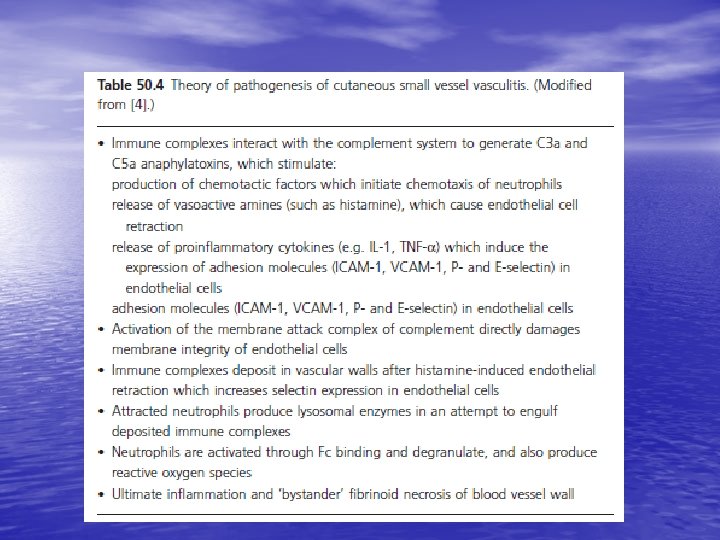

Cutaneous small vessel vasculitis • • • mainly cutaneous post-capillary venules, 50% of cases ‘idiopathic’, 15% due to infection, 15% related to inflammatory diseases (such as collagen vascular disorders), 15% due to medications 5% are associated with malignancy

Leukocytoclastic vasculitis • may be localized to the skin or may manifest in other organs. The internal organs affected most commonly include the joints, the gastrointestinal tract, and the kidneys. The prognosis is good in the absence of internal involvement.

Physical • The most common manifestation of cutaneous vasculitis is palpable purpura, but other manifestations may develop. • They may coalesce to form plaques; in some instances, they may ulcerate. • Legs is most common location • Urticarial lesions • Livedo reticularis • Nodular lesions • Ulceration

• treatment of cause. Rx • colchicine or dapsone • antihistamines • NSAIDS • severe visceral involvement may require high doses of corticosteroids with or without an immunosuppressive agent • severe or debilitating disease might also be treated with biologic agents such as rituximab or intravenous immunoglobulin

vasculitis



- Slides: 77