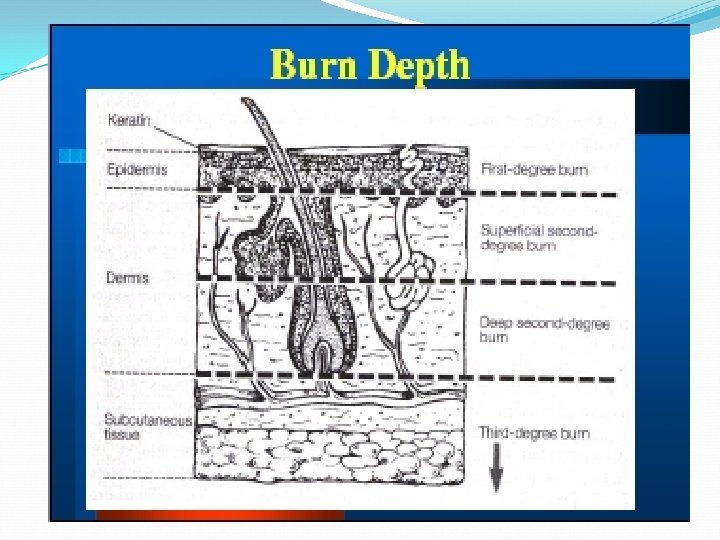
Depth of burn Partial thickness burn involves epiderm






Depth of burn Partial thickness burn involves epiderm Deep partial thickness involves derm Full thickness involves all of ski
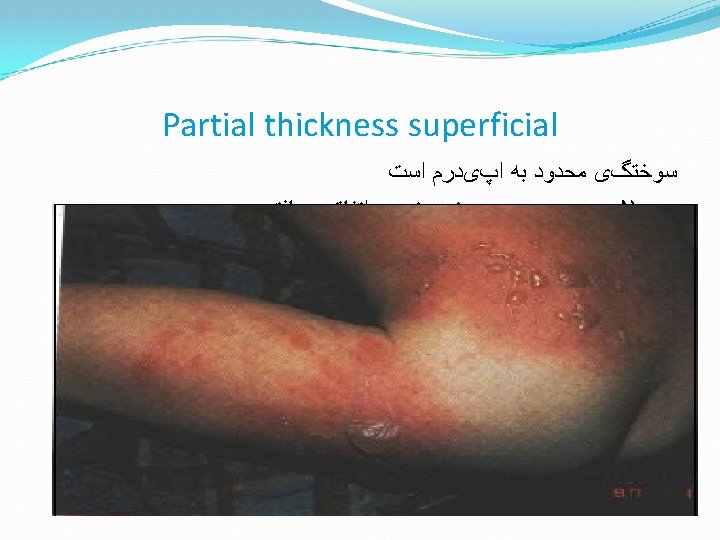

Partial thickness burns Sunburn is a very superficial burn. Expect blistering and peeling in a few days. Maintain hydration orally. Heals in 3 -6 days- generally no scaring Topical creams provide relief. No need for antibiotics • • •


Mixed partial and full thickness Central yellow area might be full thickness. Outer edges are probably partial thickness. Initial management is the same. Later will need skin grafts for the full thickness areas.

Deeper partial thickness Blisters are typical of partial thickness burns. Don’t be in a hurry to break the blisters. Heals in 14 -21 days Blisters provide biologic dressing and comfort. Once blisters break, red raw surface will be very painful. � � �
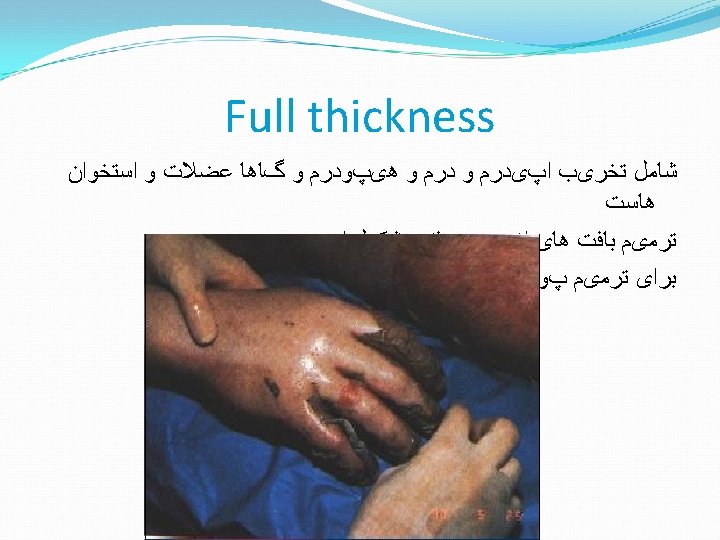

Full thickness burn Yellow, “leathery” appearance; or charred Often have no sensation (nerve endings destroyed) Outer edges might be partial thickness. Initial management same as partial thickness. Later will need skin grafts. � � �




Estimate the size of the burn The patient’s own palm is about 1% of his body surface � area. “Rule of Nines” �

Rule of 9 s ABA
.")
Burn size in small children The head accounts for about 18% (instead of 9%). The legs account for about 13% (instead of 18%).

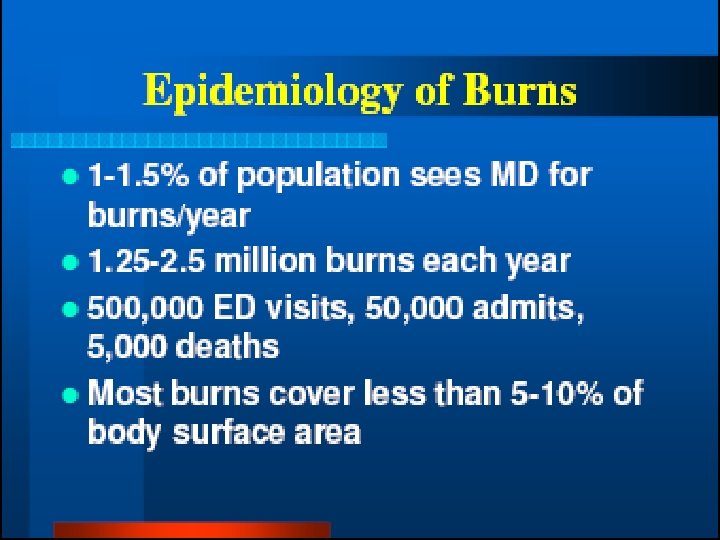
severity grading system American Burn Association burn injury

Minor burn 15 percent TBSA or less in adultsv 10 percent TBSA or less in children and older adults v 2 percent TBSA or less full-thickness burn in children v or adults without cosmetic or functional risk to eyes, ear, face, hands, feet, or perineum

The two commonly used methods of assessing TBSA: in adults are the Lund-Browder chart and "Rule of Nines, “ whereas in children, the Lund-Browder chart v is the recommended method because it takes into account the relative percentage of body surface area affected by growth.

Moderate burn 15 to 25 percent TBSA in adults with less than 10 percent v full-thickness burn 10 to 20 percent TBSA partial-thickness burn in children v under 10 and adults over 40 years of age with less than 10 percent full-thickness burn 10 percent TBSA or less full-thickness burn in children or v adults without cosmetic or functional risk to eyes, ears, face, hands, feet, or perineum

Major burn 25 percent TBSA or greater v 20 percent TBSA or greater in children under 10 and adults over 40 years v of age 10 percent TBSA or greater full-thickness burn v All burns involving eyes, ears, face, hands, feet, or perineum that are v likely to result in cosmetic or functional impairment All high-voltage electrical burns v All burn injury complicated by major trauma or inhalation injury v All poor-risk patients with burn injury v





Care of small burns What can YOU do?

Care of small burns Clean entire limb with v soap and water (also under nails). Apply antibiotic cream v (no PO or IV antibiotic). Dress limb in position of function, and v elevate it. No hurry to remove blisters unless infection occurs. v Give pain meds as needed (PO, IM, or IV) v v Rinse daily in clean water; in shower is very practical. v Gently wipe off with clean gauze. v

Blisters break on their own Upper arm burn day 1 day 2 Burn “looks worse” the next day because of blisters breaking and oozing

Blisters In the pre-hospital setting, there is no hurry to v remove blisters. Leaving the blister intact initially is less painful v and requires fewer dressing changes. The blister will either break on its own, or v the fluid will be resorbed.

American Burn Assoc says send these to a burn center Partial thickness burns >10% BSA • Burns involving the face, hands, feet, genitalia, • perineum, or major joints full thickness/3 degree burn • Electrical, Chemical, and Inhalation burns • In combat, all but the most superficial burn should be evacuated •

Airway? “Flash” burns may refer to v that suddenly flare up, then die down quickly. Patients may have burnt facial v hair and carbon on lips. Patients with this kind of facial v burn will probably NOT need an artificial airway. Give humidified oxygen while v under close observation.


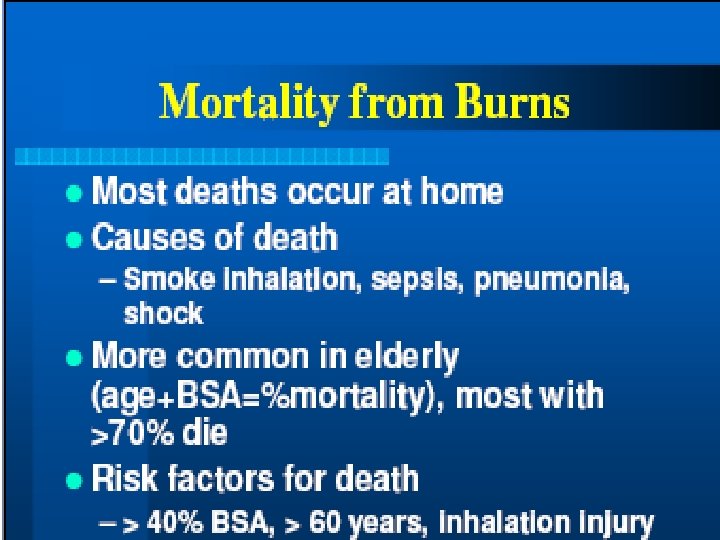
Causes of death in burn patients Circulation: “failure of resuscitation” Cardiovascular collapse, or acute MIv Acute renal failurev Other end organ failurev Missed non-thermal injuryv

Escharotomy - indications Circulation to distal limb is in danger v due to swelling. Progressive loss of sensation / motion in hand / foot. Progressive loss of pulses in the distal extremity by palpation or doppler. In circumferential chest burn, patient v might not be able to expand his chest enough to ventilate, and might need escharotomy of the skin of the chest.

Neuro status The burn itself does not alter the level of consciousness. v If patient is not alert, think of other causes: v hypovolemia v carbon monoxide v head injury v Don’t allow swollen eyelids to prevent you from v examining the pupils. Test sensation and motion in burned extremities. v

Circulation Record vital signs. Check distal pulses and nail beds. v Keep him warm! Loss of skin impairs ability to retain heat and fluids. Being cold will cause vasoconstriction. Monitor urine output (in larger burns, insert v Foley catheter for hourly urine output). 30/50 cc/hr Monitor at least HCT and urine specific gravity. v When available, monitor electrolytes. v
 Depression")
Edema Formation Amount of edema can be v immense (even without facial burns) Depression of mental status can v worsen problem Edema peaks at 12 to 24 hoursv Pediatric patients even more v concerning

Upper arm burn 121 Blisters show probable partial thickness burn. v Area without blister might be deeper partial v thickness.

Arm burn 4 days

Arm burn 7 days – note the exudate

After debridement

Debride blister using simple instruments

Causes of death in burn patients Airway v Facial edema, and/or airway edema Breathingv Toxic inhalation (CO, +/- CN) Respiratory failure due to smoke injury or ARDS

Special types of burn Circumferential burnn Burn requiring escharotomyn Electrical burnn Chemical burnn

Burns of special areas of the body Face n Mouthn Neckn Hands and feetn Genitalian

Genitalia Shower daily, rinse off old cream, apply new cream. v Insert Foley catheter if unable to urinate due to swelling. v

Circumferential burn Limb is burned all the way around. v Soft tissues under the skin always swell with v burns (due to capillary leak of fluids in first day or so). There is a loss of skin expansion due to the loss v of turgor/elasticity in burned tissue Pressure inside limb gradually increases. v Eventually, pressure inside limb exceeds arterial v pressure. This requires escharotomy to relieve the pressure. v

Hands and feet Fingers might develop contractures if active measures are not taken to prevent them.

Hands and feet Allow use of the hands in dressings by v day. Splint in functional position by night. v Keep elevated to reduce swelling. v

Face Be VERY concerned for the airway!! Eyelids, lips and ears often swell alarmingly. In fact, they look even worse the next day. But they will start to improve daily after that. Cleanse eyes with warm water or saline. Apply antibiotic ointment or liquid tears until lids are no longer swollen shut. Bacitracin cream/ointment will serve


Phosphorus Particles of phosphorus v must be removed from under the skin. Pick them off with v forceps. Must apply wet dressing v to prevent re-igniting.

Electrical burn Outer skin might not appear v too bad. But heat was conducted v along the bone. Causes the most damage. v Burns from inside out. v Usually requires fasciotomy v

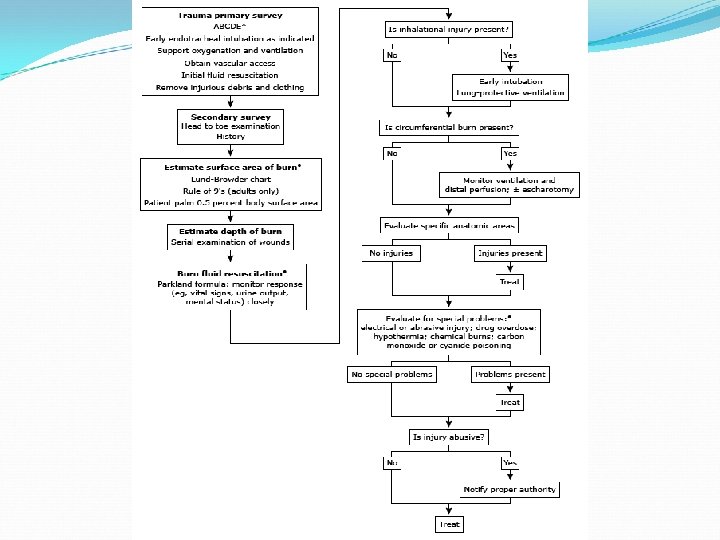
QUESTIONS? SUMMARY Describe how to estimate the body surface area of burn. Describe how to calculate initial fluid requirements in a patient with a large burn. Describe intial management of a patient with a large burn. Discuss indications and complications of escharotomy. � �

- Slides: 72