DEPRESSION Depression Ill change my state with any



: -")










 Pro-Actively Limit Choices to “ 1")



")
- Slides: 20
DEPRESSION
Depression “I’ll change my state with any wretch, Thou canst from gaol or dunghill fetch. My pain’s past cure, another Hell, I may not in this torment dwell, Now desperate I hate my life, Lend me a halter or a knife. All my griefs to this are jolly, Naught so damn’d as Melancholy. ” Robert Burton, The Anatomy of Melancholy (1621) “Depression is a disorder of mood, so mysteriously painful and elusive in the way it becomes known to the self—to the mediating intellect—as to verge close to being beyond description. It thus remains nearly incomprehensible to those who have not experienced it in its extreme mood, although the gloom, “the blues” which people go through occasionally and associate with the general hassle of everyday existence are of such prevalence that they do give many individuals a HINT of the illness in its catastrophic form. ” William Styron, Darkness Visible: A Memoir of Madness (1990)
Causes of Disability in the United States, Canada, and Western Europe in 2000 Iglehart, J. K. N Engl J Med 2004; 350: 507 -514
The Birth & Growth of “Major Depression” Statistics for “Major Depressive” Disorder (DSM-IV): - moderate to severe depression: 6. 5% community prevalence rate - lifetime frequency approaches 20% - 22% of older adults report “feeling sad” most of the day/every day We live in an “age of melancholy”. “bread and butter” of psychiatry, just as “neurosis” was pre-DSM III: - 54% of psychiatric visits and treatment are for depression - 15% are for schizophrenia - 9% are for anxiety disorders - 22% are for all else combined
Diagnostic Algorithm for Major Depression Whooley, M. A. et al. N Engl J Med 2000; 343: 1942 -1950
Diagnostic Categories for Depression
The Birth & Growth of “Major Depression” Pre-DSM III term: “melancholia” – relatively rare and confined to mental asylums 1917 - 8% of psychiatrists in private/outpatient practice 1941 - 38% “ “ “ 1970 - 66% “ “ “ 1920 s-1970 s: psychiatry shifted its focus to psychopathology of daily life / everyday concerns (sex, marriage, worldly failure) Depression in U. S. dichotomized: “endogenous” or “reactive” In Europe: “endogenous-psychotic” or “neurotic-reactive”
The Birth & Growth of “Major Depression” Q: Why did this binary view of depression slowly die out in the 1970 s? - clear, distinct boundaries between the 2 categories hard to find - John Feighner at Washington University (“Feighner criteria” 1972) 3 criteria - dysphoric mood marked by symptoms of being depressed, sad, despondent, hopeless - 5 of 7 symptoms from: loss of appetite, sleep difficulty, loss of energy, agitation, loss of interest in usual activities, guilt feelings, slow thinking, or recurrent suicidal thoughts must be present disorder - must have lasted at least 1 month and not be due to another preexisting mental Feighner criteria = extraordinarily high reliability rating scores
The Birth & Growth of “Major Depression” Other major factors in demise of “reactive depression”: - psychiatric medications became diagnostic “splitters” - modern living vs. hereditary predisposition: drugs treat both the same Peter Kramer’s Listening to Prozac: A Psychiatrist Explores Antidepressant Drugs and the Remaking of the Self (1993) - changed what constituted “complete treatment” - coincided with rise of managed care/HMOs - changed treatment of “sub-threshold” cases - “baseline” change: treatment vs. enhancement -------------------------------Conflating minor depression/dysthymia with major depression leads to two troublesome outcomes: (1) social forces are not considered or taken seriously (2) limits the search for holistic treatment and prevention
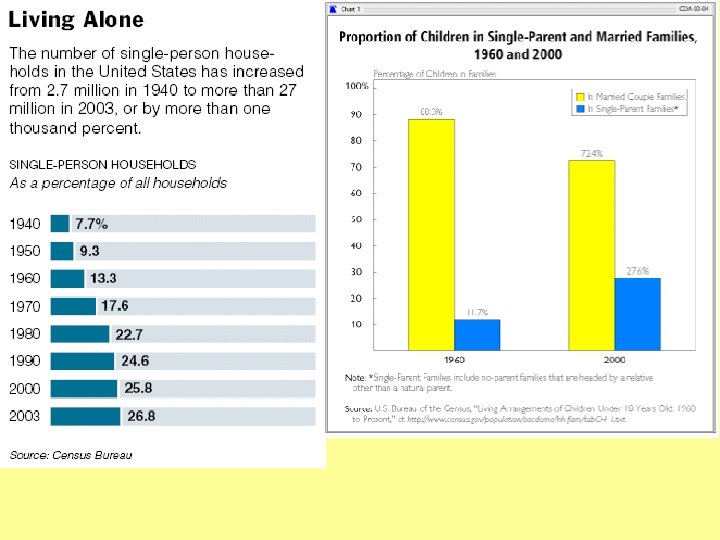
“Major Depression” and Environmental Stress
“Major Depression” and Environmental Stress
The Futile Pursuit of Happiness: Environmental Stress Gilbert, Wilson, Loewenstein, & Kahneman: “We consistently misestimate the intensity and duration of something’s utility; this is known as the ‘impact bias’. ” Our ability to predict the emotional consequences of a decision, purchase, or event is less than we think. Our mistakes of expectation can lead directly to mistakes in choosing what we think will give us pleasure. We often “miswant. ” Key role of “adaptation” to good things and “resilience” to bad things. our “psychological immune system” (a sort of emotional “thermostat”) e. g. , remember when you got your first dial-up 14, 400 baud modem?
The Tyranny of Choice • “Starter Marriages” phenomenon Census Bureau: 3 million divorced 18 -29 year-olds (1999) 253, 000 divorced 25 -29 year-olds (1962) • Atul Gawande, M. D. & cancer study - 65% of people surveyed say that if they were to get cancer, they would want to choose their own treatment; of those who do get cancer, though, only 12% actually want to choose • Steven Venti, Dartmouth economist & Employer 401 k plans The more funds employers offer their employees in 401 k plans, the less likely the employees are to invest in any of them. • “Wine Warehouse” vs. “Gas Station” experiences
Depression and the Tyranny of Choice Excessive choice is often psychologically and emotionally burdensome. Why? (1) Increases burden of information gathering to make a wise decision (2) Doing all the “cost-benefit/expected utility” calculations is exhausting (3) Increases expectations about how good the decision will be (4) People often assemble an idealistic composite of all the options foregone (5) Which increases the likelihood that they will regret the decision they make (6) And increases the chance that they will blame themselves when a decision fails to live up to expectations (more regret and second-guessing). Schwartz: Perhaps colleges/universities offer too many choices now, which might help explain double-, triple-majoring, etc. (e. g. , Spiderbytes)
Combating the “Paralysis of Choice” Helpful countermeasures: (1) Pro-Actively Limit Choices to “ 1 st order, ” “ 2 nd order, ” “ 3 rd order” (2) Counterfactual Downward (3) Make Some Decisions Nonreversible (e. g. , Harvard photography class) (4) Anticipate Adaptation (5) Learn to Love Constraints (Say “No”)
Teens and the Antidepressant Dilemma Young people's use of the antidepressants known as selective serotonin reuptake inhibitors appears to have more than doubled between 1995 -96 and 2001 -02. That's based on a database of visits associated with an SSRI prescription. While only one SSRI drug, fluoxetine, has FDA approval for use in adolescents, the data suggests that by 2002 other SSRIs had taken a larger share of these prescriptions. Journal of Adolescent Health (2005)
Teens and the Antidepressant Dilemma: “Rollback” Dilemma
Treating the Environment & Dangers of Under-Diagnosing public health imperative: prevention! environmental stressors & prevalence Maria Shin, right, and her husband moved to Great Neck from Seoul, seeking a less pressured academic life for their two teenage children
Dangers of Over- and Under-Diagnosing Hans Eysenck’s personality theory (1947)