Dental Caries By Syed MukhtarUnNisar Andrabi Introduction Dental

Dental Caries By: Syed Mukhtar-Un-Nisar Andrabi

Introduction � Dental caries is an infectious microbiologic disease of teeth which involves the destruction of the mineralized tissues and dissolution of the calcified matrix. � Caries has affected humans since prehistoric times, the prevalence of this disease has greatly increased in modern times on a worldwide basis, an increase strongly associated with dietary change. � This trend peaked and began to decline in many countries in the late 1970 s and early 1980 s, and the decline was most notable in certain segments of the population of the United States, western Europe, New Zealand, and Australia. “

Introduction �On a worldwide basis the prevalence of caries is declining in developed countries, it is increasing in less developed countries, and is epidemic in countries with emerging economies. “

� Carious lesions only occur under a mass of bacteria capable of producing a sufficiently acidic environment to demineralise tooth structure. � A gelatinous mass of bacteria adhering to the tooth surface is termed dental plaque. � The plaque bacteria metabolize refined carbohydrates for energy and produce organic acids as a by-product which cause a carious lesion by dissolution of the tooth's crystalline structure.

Evidence for the role of bacteria in the genesis of caries � Teeth free from bacterial infection, either in germfree animals or unerupted teeth in humans, do not develop caries. � Antibiotics are effective in reducing caries in animals and humans. � Oral bacteria can demineralize enamel in vitro and produce lesions similar to naturally occurring caries. � Specific bacteria can be isolated and identified from plaque over various carious lesions.

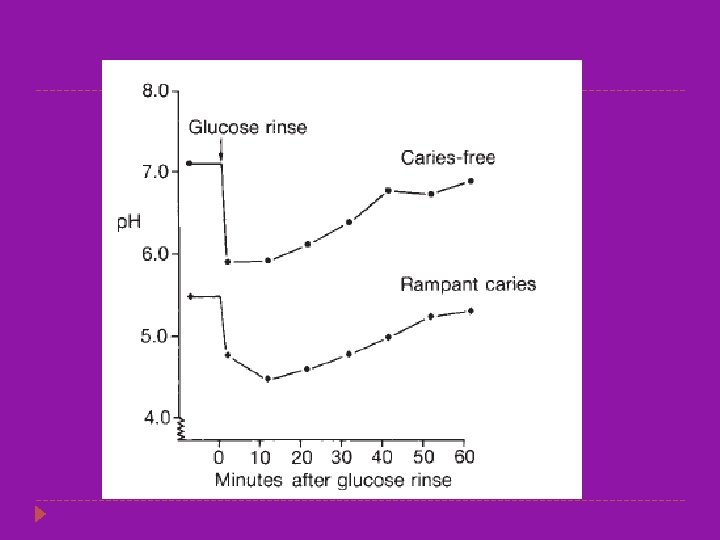
The carious process and the carious lesion � The carious process is the metabolic activity in the plaque biofilm. � Caries is a dynamic process with ongoing demineralization and remineralization � The cumulative result of these de- and remineralization processes may be a net loss of mineral and a carious lesion can be seen. � The de-and remineralization processes can be modified particularly by regular disturbance of the biofilm with a toothbrush and fluoride toothpaste.

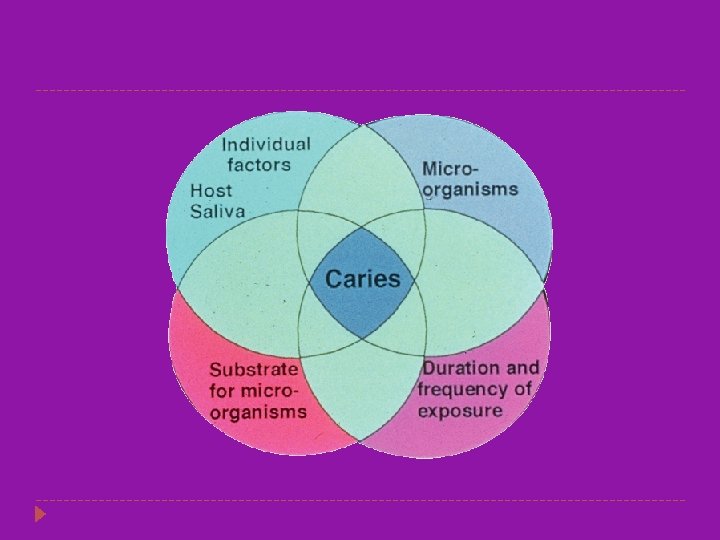
The carious process and the carious lesion � For caries to develop, three factors must occur at the same time: �A susceptible tooth �Diet rich in fermentable carbohydrates �Specific bacteria (regardless of other factors, caries cannot occur without bacteria)

Caries Etiology � There are two specific groups of bacteria found in the mouth that are responsible for dental caries: � Mutans streptococci (S. mutans, S. salivarius, S. sanguis, S. mitior, S. millieri) � Lactobacilli � They are found in relatively large numbers in the dental plaque. � The presence of lactobacilli in the mouth indicates a high sugar intake. � A. naeslundi, A. viscosus are responsible for development of root caries.

Caries Etiology � MS are present as a pandemic infection in humans; that is, MS are found in everyone regardless of race, ethnic background, or geographic origin. � Normally MS exist in the mouth as an insignificantly small component of the oral flora. � In patients with multiple active carious lesions, MS have become a dominant member of the plaque flora.

Plaque retention and susceptible sites � Enamel pits and fissures on occlusal surfaces of molar and premolar teeth � Proximal enamel smooth surfaces just cervical to the contact area � Enamel at the cervical margin of the tooth at the gingival margin � The margins of restorations, particularly where there is a wide gap between the restoration and the tooth or those where the restoration overhangs the margin of the cavity

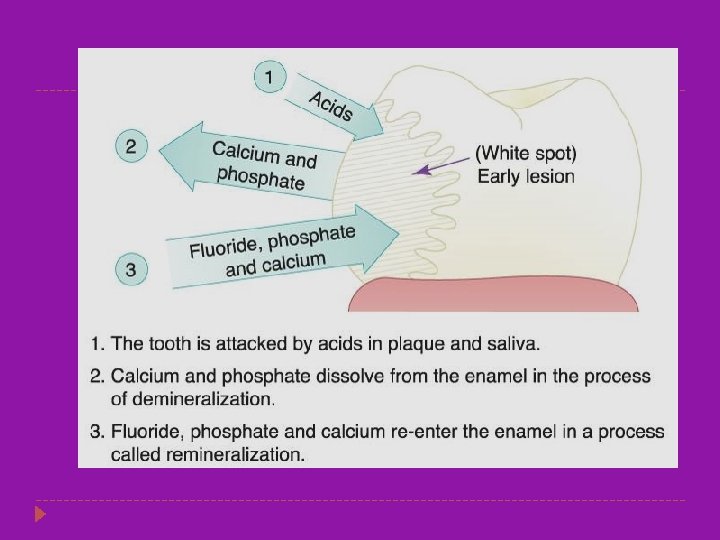
Stages of Caries Development � It usually takes a period of time, from months to years, for a carious lesion to develop. � It is an ongoing process, characterized by alternating periods of demineralization and remineralization. � Demineralization is the dissolving of the calcium and phosphate from the hydroxyapatite crystals. � Remineralization is the calcium and phosphate being redeposited in previously demineralized areas. � It is possible to have the processes of demineralization and remineralization occur without any loss of tooth structure.

Stages of Caries Development-cont’d � Incipient lesion develops in the earliest stages when caries begins to demineralize the enamel. � Overt, or frank, lesion is characterized by cavitation (the development of a cavity or hole in the tooth). � Rampant: The time between the onset of the incipient lesion and the development of the cavity is rapid and there are multiple lesions throughout the mouth.

Areas for Development of Caries �Pit and fissure caries occurs primarily on the occlusal surfaces and buccal and lingual grooves of posterior teeth, as well as in lingual pits of the maxillary incisors. �Smooth surface caries occurs on intact enamel other than pits and fissures. �Root surface caries occurs on any surface of the root. �Secondary, or recurrent, caries occurs on the tooth surrounding a restoration.

�In younger age groups pit and fissure caries is more common than approximal caries and buccal and lingual caries; �Posterior approximal caries is more common than anterior approximal caries. �In older patients root surfaces exposed by gingival recession may be the predominant site for caries to occur.

Pit and Fissure Caries � Highest prevalance of all caries bacteria rapidly colonize the pits and fissures of the newly erupted teeth � These early colonizers form a “bacterial plug” that remains in the site for long time , perhaps even the life of the tooth � Type & nature of the organisms prevalent in the oral cavity determine the type of organisms colonizing the pit & fissure � Numerous gram positive cocci, especially dominated by s. sanguis are found in the newly erupted teeth.

�The appearance of S. mutans in pits and fissures is usually followed by caries 6 to 24 months later. �Sealing of pits and fissures just after tooth eruption may be the most important event in their resistance to caries. � Shape, morphological variation and depth of pit and fissures contributes to their high susceptibility to caries. �Caries expand as it penetrates in to the enamel.
: Based on the alphabetical description of shape– 4 types")
Morphology Of Fissures NANGO (1960): Based on the alphabetical description of shape– 4 types V&U type: self cleansing and somewhat caries resistant U type: narrow slit like opening with a larger base as it extend towards DEJ. Caries susceptible; also have a number of different branches K type: also very susceptible to caries
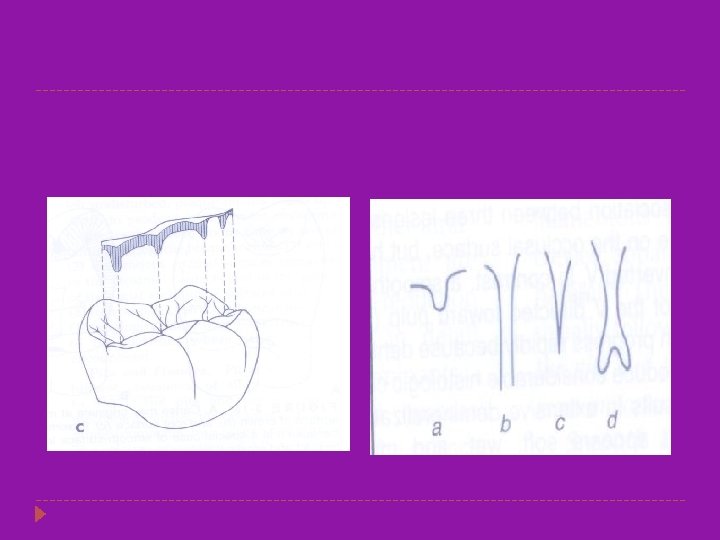

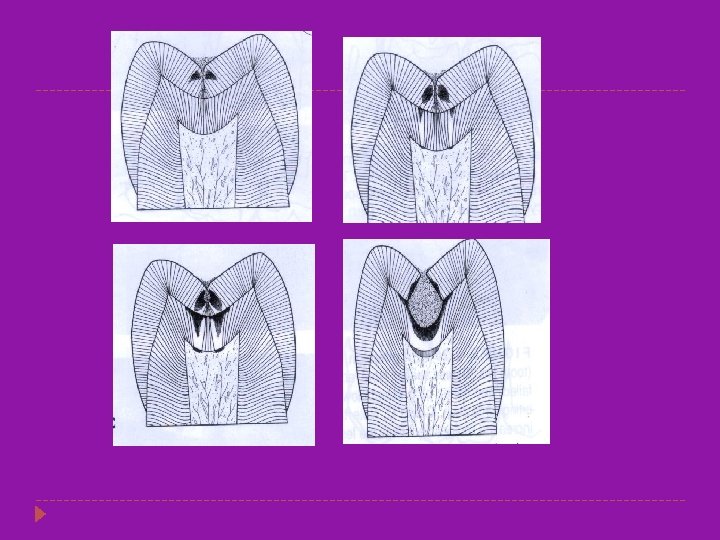
�Entry site may appear much smaller than actual lesion, making clinical diagnosis difficult. �Carious lesion of pits and fissures develop from attack on their walls. �In cross section, the gross appearance of pit and fissure lesion is inverted V with a narrow entrance and a progressively wider area of involvement closer to the DEJ.

Smooth surface caries � Less favorable site for plaque attachment, usually attaches on the smooth surface that are near the gingiva or are under proximal contact. � In very young patients the gingival papilla completely fills the interproximal space under a proximal contact and is termed as col. Also crevicular spaces in them are less favorable habitats for s. mutans. � Consequently proximal caries is less lightly to develop where this favorable soft tissue architecture exists.

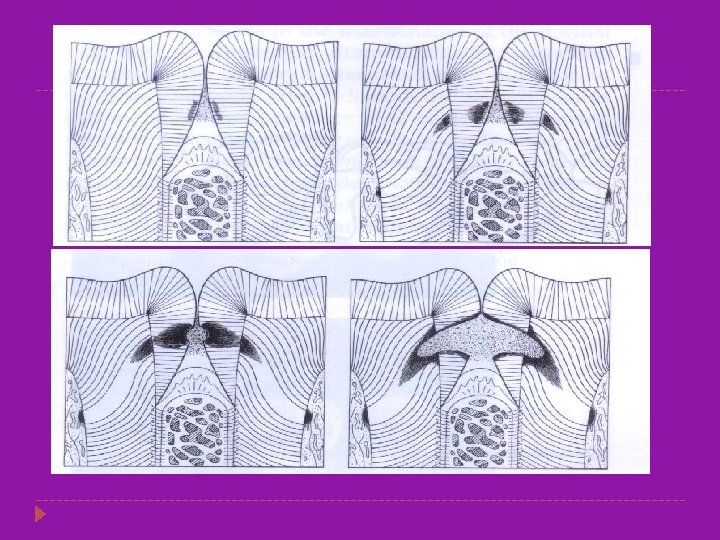
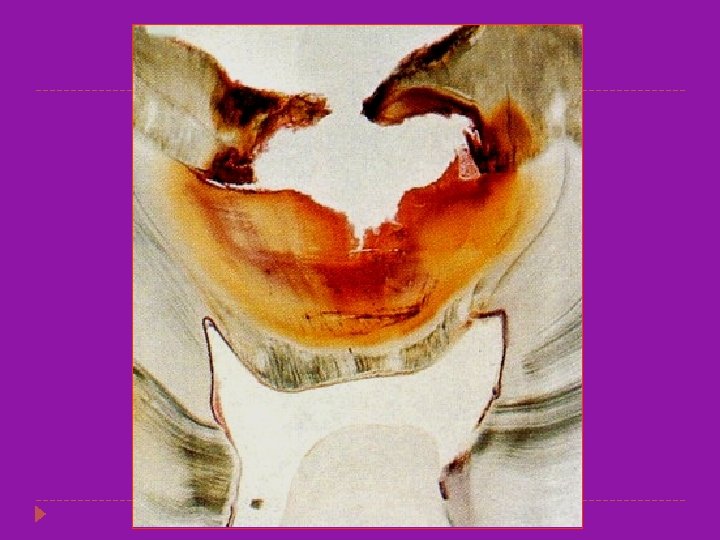
�The proximal surfaces are particularly susceptible to caries due to extra shelter provided to resident plaque owing to the proximal contact area immediately occlusal to plaque. �Lesion have a broad area of origin and a conical, or pointed extension towards DEJ. �V shape with apex directed towards DEJ. �After caries penetrate the DEJ softening of dentin spread rapidly and pulpally
 is seen to occur")
Linear enamel caries � Linear enamel caries ( odontoclasia ) is seen to occur in the region of the neonatal line of the maxillary anterior teeth. � The line, which represent a metabolic defect such as hypocalcemia or trauma of birth, may predispose to caries, leading to gross destruction of the labial surface of the teeth. � Morphological aspects of this type of caries are atypical and results in gross destruction of the labial surfaces incisor teeth

Root Surface Caries � � The proximal root surface, particularly near the cervical line, often is unaffected by the action of hygiene procedures, such as flossing, because it may have concave anatomic surface contours (fluting) and occasional roughness at the termination of the enamel. These conditions, when coupled with exposure to the oral environment (as a result of gingival recession), favor the formation of mature, caries-producing plaque and proximal root-surface caries. Root-surface caries is more common in older patients. Caries originating on the root is alarming because 1. it has a comparatively rapid progression 2. it is often asymptomatic 3. it is closer to the pulp 4, it is more difficult to restore

� The root surface is softer than the enamel and readily allows plaque formation in the absence of good oral hygiene. � The cementum covering the root surface is extremely thin and provides little resistance to caries attack. � Root caries lesions have less well-defined margins, tend to be U-shaped in cross sections, and progress more rapidly because of the lack of protection from and enamel covering.

HISTOPATHOLOGY OF CARIES

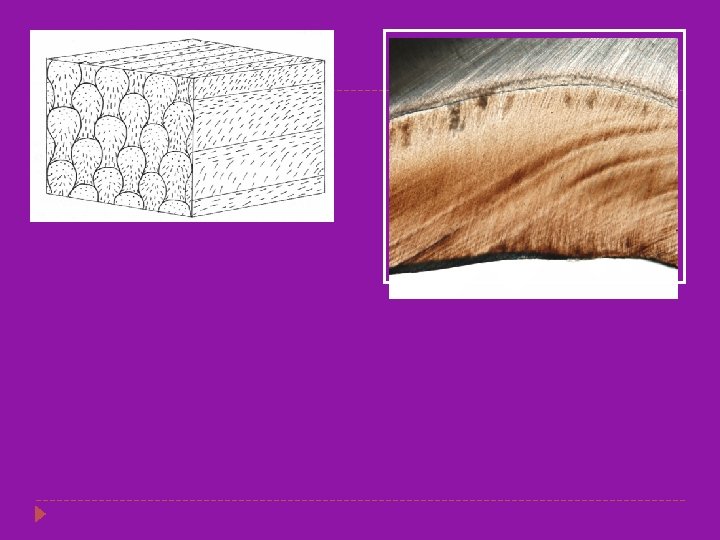
Histology of Enamel � Enamel is composed of very tightly packed hydroxyapatite crystallites, organized into long columnar rods (prisms). � The rods are key-shaped in cross-section with each rod starting at the DEJ and extends as a wavy, continuous column to the surface of the crown. � The mineralization process is apparently somewhat discontinuous and is characterized by alternating phases of high and low activity. � Periods of low activity create "rest“ lines within the rods. Several rest lines in adjacent rods form-“striae of Retzius”.

Histology of Enamel � The striae and the inherent spaces in prism boundaries provide sufficient porosity to allow movement of water and small ions, such as hydrogen ions. � Thus enamel acts as a “molecular sieve” by allowing free movement of small molecules and blocking the passage of larger molecules and ions. � The striae form horizontal lines of greater permeability in the enamel, they probably contribute to the lateral spread of smooth surface lesions.

Tufts and Enamel Lamella � � � Enamel spindles are short spindle-like structures that are the ends of dentinal tubules that are trapped in enamel. Enamel tufts are hypocalcified enamel rods that resemble tufts of grass. Enamel lamellae, hypocalcified enamel rods, are of two types, false and true. � False enamel lamellae are cracks in enamel and frequently extend into the dentin. � True enamel lamellae are hypocalcified enamel rods that are poorly calcified or uncalcified due to developmental disturbances affecting the ameloblasts. Enamel Spindle Enamel Tuft Histological slide prepared and provided by the Department of Biomedical Sciences, University of Maryland, Dental School.

Tufts and Enamel Lamella

Enamel Lamellae False Enamel Lamella True Enamel Lamella

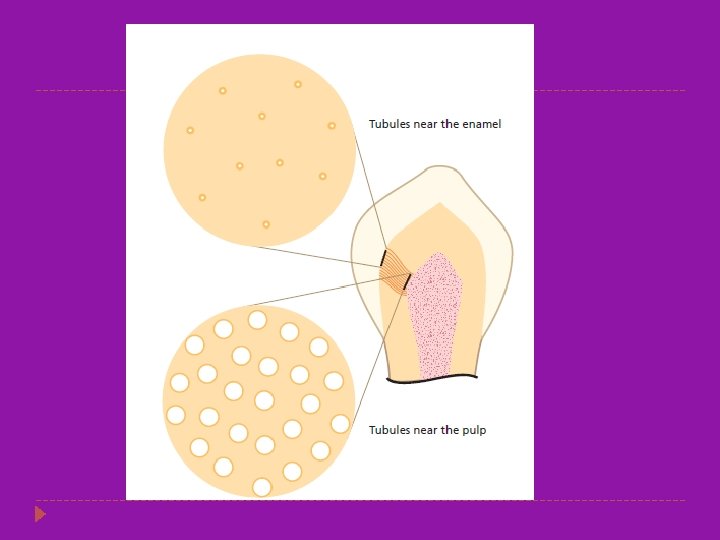
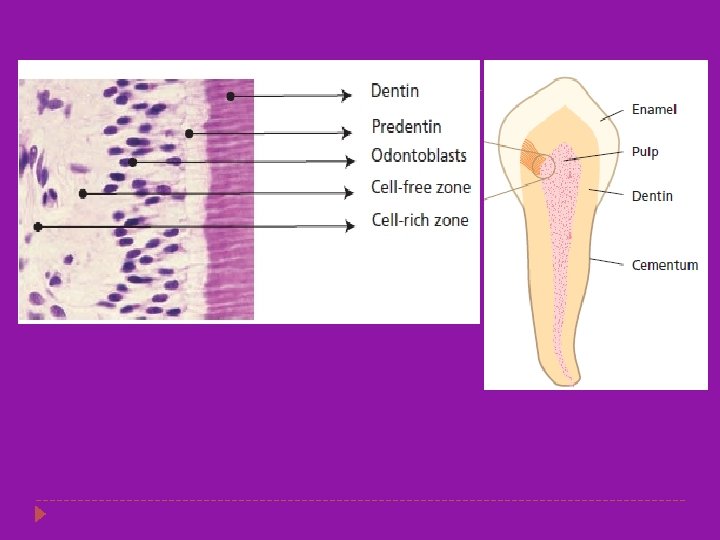
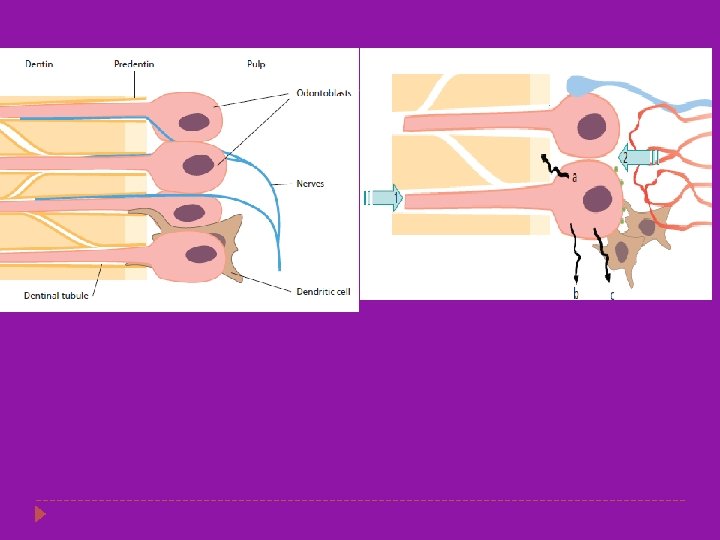
Histology of Dentin � Dentin is an intrinsically hydrated tissue, penetrated by a maze of 1 to 2. 5 um diameter fluid-filled dentin tubules. � Dentinal tubules enclose cellular extensions from the odontoblasts and therefore are in direct communication with the pulp. � Each odontoblast is a pulp cell that is associated with a tubule extending to the external periphery of the dentin � Average tubule diameter ranges from 0. 63 um at the periphery to 2. 37 um near the pulp � The dentin and the pulp are morphologically and embryologically a single unit.

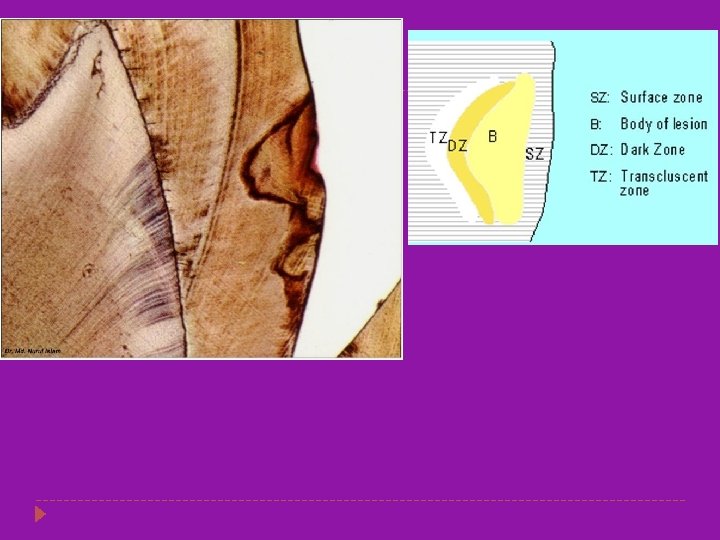
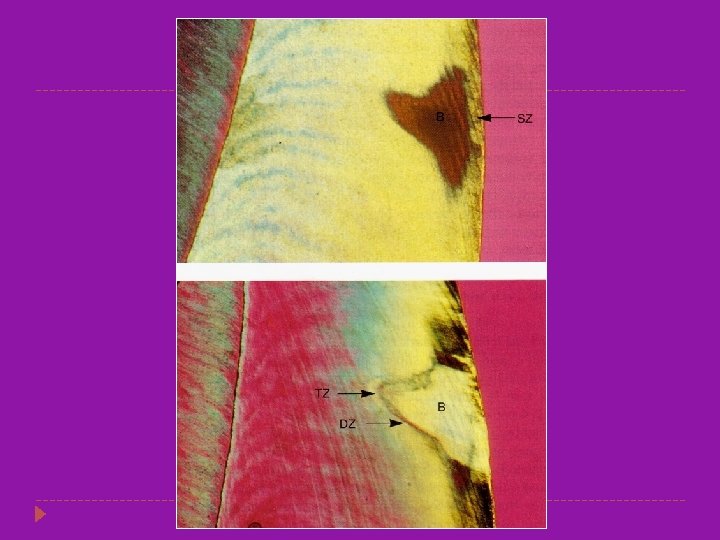
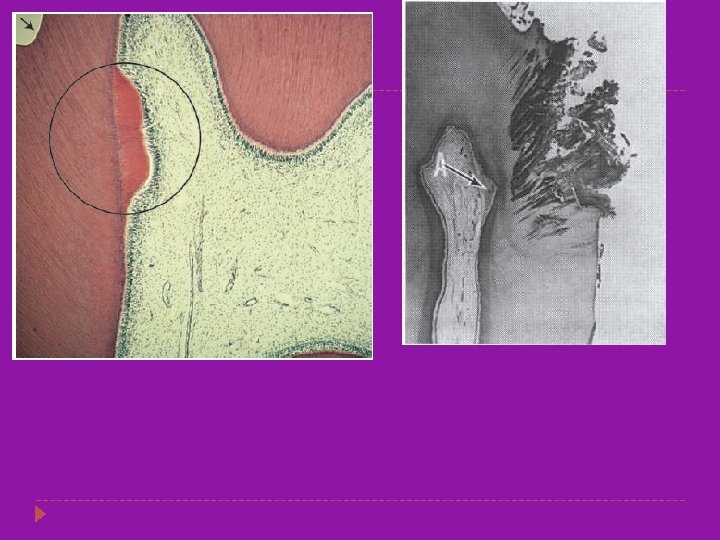
ENAMEL CARIES � � The early lesion is a white spot which appears on the surface of the enamel the extension of caries is cone shaped with the base towards the outer enamel surface and the apex towards the DEJ. Caries spreads in zones which are as follows. Translucent zone Dark zone Body of the lesion Surface zone

Translucent Zone �Zone of Intial demineralization � More porous than the normal enamel. � The pore volume of the translucent zone of enamel caries is 1%, 10 times greater than normal enamel. � These pores are larger than the normal enamel. � Chemical analysis show that there is a fall in the magnesium and carbonate content as compared to the normal enamel

Dark zone � This zone contains 2 -4% by volume pores � Some pores are large and some are smaller than the translucent zone suggesting that some remineralization has occurred. � In rapidly advancing lesion the dark zone narrow. � In this zone previously liberated salts are redeposited

Body of the Lesion � This zone has pore volume of 5 -25% � It is the largest portion of the incipient lesion while in a demineralizing phase. � There is more of an effort for the remineralization but by the further attack there is further dissolution of the mineral � Thus this is the zone of maximum demineralization. � (TEM) and (SEM) demonstrate the presence of bacteria invading between the enamel rods (prisms) in the body zone.

Surface zone � This is about 40 micrometer thick � This part is relatively normal because in this area there is maximum remineraization from the inorganic components of both the plaque and saliva.

CARIES OF DENTIN �Caries advances more rapidly in dentin than in enamel because dentin provides much less resistance to acid attack because of less mineralized content. � Dentin contains much less mineral and possesses microscopic tubules that provide a pathway for the ingress of acids and egress of mineral. � The dentinoenamel junction has the least resistance to caries attack and allows rapid lateral spreading. � Caries produces a variety of responses in dentin, including pain, demineralization, and remineralization.

CARIES OF DENTIN � Three levels of dentinal reaction to caries can be recognized: (1) reaction to a long-term, low-level acid demineralization associated with a slowly advancing lesion; (2) reaction to a moderate-intensity attack; and (3) reaction to severe, rapidly advancing caries characterized by very high acid levels. The dentin can react defensively (by repair) to low- and moderate intensity caries attacks as long as the pulp remains vital and has an adequate blood circulation. .
")
Zones of Dentinal Caries � Caries advancement in dentin proceeds through three changes: (1) weak organic acids demineralize the dentin; (2) the organic material of the dentin, particularly collagen, degenerates and dissolves; and (3) the loss of structural integrity is followed by invasion of bacteria. Five different zones have been described in carious dentin
")
(work of Dr. T. Fusayama. Copyright Ishiyaku Euro. America, Inc. Tokyo, 1993. )
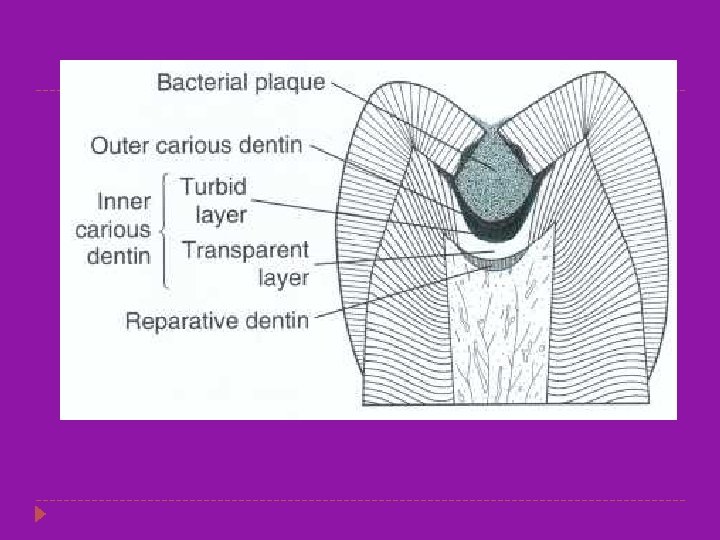

Zones of Dentinal Caries Zone 4: Turbid Dentin. Zone 1: Normal Dentin � Zone of bacterial invasion- widened and � It is the deepest area which has tubules distorted dentinal tubules filled with bacteria. with odontoblastic processes that are smooth, and no crystals are in the lumens. � Little mineral present, collagen irreversibly denatured. Zone 2: Subtransparent Dentin. � Stained by caries detection dyes. � a zone of demineralization of the intertubular dentin. Zone 5: Infected Dentin. � Damage to odontoblast is evident but no � Outermost zone with no recognizable bacteria in the lesion. structure to the dentin. � Amenable to remineralization, not stained � Collagen and mineral seem to be absent. by caries detection dyes. � Great nos. of bacteria are dispersed in this Zone 3: Transparent Dentin zone. � Zone of further demineralization � Softened dentin, large crystals in tubular lumens but no bacteria. � Collagen cross-linking intact and thus not stained by caries detection dyes. � Amenable to remineralization.

MANAGEMENT OF CARIES

MANAGEMENT OF CARIES � Management of dental caries and its consequences remains the dominant activity of dentists. � ***Current strategy for caries management is based on “CAMBRA” caries management by risk assessment. Objectives of caries management: � Diagnosis (especially identifying those people at high risk for caries), � Preventive measures, and � Treatment modalities.

For caries to occur, three factors must be present simultaneously and in the correct manner. These are: (1) cariogenic bacteria, (2) a susceptible tooth surface, and (3) available nutrients to support bacterial growth. Caries is an infectious disease caused by cariogenic plaque formation on the tooth that causes demineralization of the tooth (enamel demineralization occurs at p. H of 5. 5 or less)
")
MS are the primary causative agents of initial coronal caries because they: � (1) adhere to enamel; � (2) produce and tolerate acid; � (3) thrivein a sucrose-rich environment; and � (4) produce bacteriocins, substances that kill off competing organisms

Carious Process 1. Ion transfer continuously occurs at the plaque/enamel interface. 2. The initial decalcification occurs subsurface and it may be 1 to 2 years before loss of the tooth's surface integrity (cavitation). 3. After enamel cavitation has occurred, the lactobacillus organism then becomes the primary agent for further destruction of the dentin. 4. As plaque is exposed to nutrients (primarily sucrose), the plaque metabolism produces acids and demineralization continues. 5. If the nutrient or the plaque itself is removed, ions from saliva (sodium, potassium, calcium or flouride) cause remineralization to occur
 Bacterial Clearance, (continuous bathing) �(2) Buffering Actions, (urea, bicarbonate)")
Protective Mechanisms Of Saliva �(1) Bacterial Clearance, (continuous bathing) �(2) Buffering Actions, (urea, bicarbonate) �(3) Antimicrobial Actions (lactoferrin, lactoperoxidase, Type A secretory immunoglobins) �(4) Remineralization (calcium, phosphate, �potassium, and sometimes fluoride ions)

CARIES DIAGNOSIS � The primary objectives of caries diagnosis are to identify: those lesions that require surgical (restorative) treatment, �those that require nonsurgical treatment, and �those persons who are at high risk for developing carious lesions. �

Methods Of Caries Diagnosis � Conventional methods: � Visual examination � Explorer & mouth mirror � Radiograghs � Alternative methods : � Digital radiogragphy � DIAGNOdent � QLF(quantitative light induce fluorescence) Electronic carries monitor � Fibreoptic transillumination

Laser Caries Detector � The laser caries detector is used to diagnose caries and reveal bacterial activity under the enamel surface. � Carious tooth structure is less dense and gives off a higher reading than non- carious tooth structure.

Fig. 13 -10 Visual and radiographic appearance of seemingly intact molar

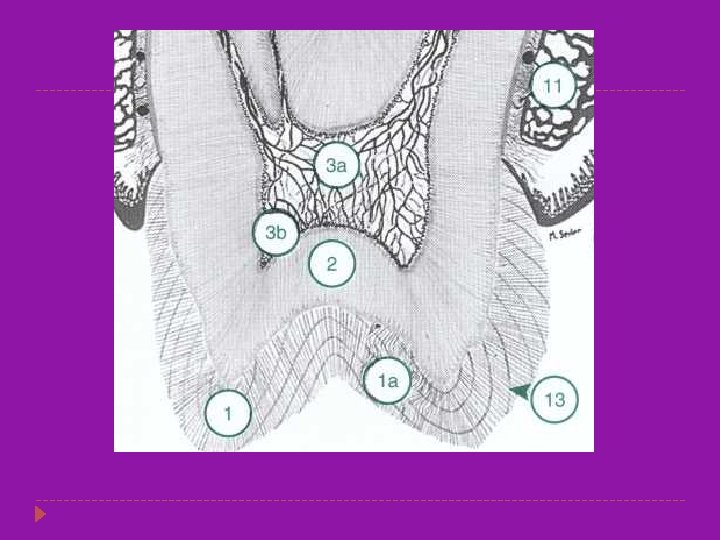
Fig. 13 -11 Cross section of molar showing decay

Primary Goals Of An Effective Diagnosis And Treatment Program � Early detection of incipient caries � Limitation of caries activity before significant tooth destruction has occurred � Identification of high-risk patients

ASSESSMENT TOOLS � Patient History � Clinical Examination � Nutritional Analyses � Salivary Analyses � Radiographic Assessment. **The minimal depth of a detectable lesion on a radiograph is about 500 µm. **Approximately 60% of teeth with radiographic proximal lesions in the outer half of dentin are likely to be noncavitated
 prior caries activity,")
Factors Contributing To An Increased Risk Of Caries Development: � (1) prior caries activity, � (2) frequent sucrose intake, � (3) minimal exposure to fluoride, � (4) young or old age, � (5) decrease in salivary functioning, � (6) high numbers of cariogenic bacteria, and � (7) presence of existing carious lesions.

Clinical Examination Findings Associated With Increased Caries Risk

Medical History Factors Associated With Increased Caries Risk

CARIES DIAGNOSIS FOR PITS AND FISSURES � Factors considered for pit-and-fissure caries diagnosis are: � (1) softening at the base of the pit or fissure; � (2) opacity surrounding the pit or fissure, indicating undermining or demineralization of the enamel; and � (3) softened enamel that may be flaked away by the explorer. **injudicious use of the explorer may actually cause a cavitation
: � No radiolucency below occlusal")
CARIES DIAGNOSIS FOR PITS AND FISSURES � Noncavitated (caries-free): � No radiolucency below occlusal enamel � Deep grooves may be present � Superficial staining may be present in grooves � Mechanical binding of explorer may occur � Cavitated (diseased): � Chalkiness of enamel on walls and base of pit or fissure � Softening at the base of a pit or fissure � Brown-gray discoloration under enamel adjacent to pit or fissure � Radiolucency below occlusal enamel

CARIES DIAGNOSIS FOR SMOOTH SURFACES � Bitewing radiographs are the most typical method for evaluation of the proximal smooth surfaces for evidence of demineralization because these areas usually are not readily assessed visually or tactilely. � An early lesion is detectable radiographically as a localized decrease in the density of the enamel immediately below the proximal contact, resulting in a radiolucent area on the radiograph. � Bitewing radiographs must be combined with clinical examination---many radiolucent lesions may be non-cavitated and can be remineralized.

CARIES DIAGNOSIS FOR SMOOTH SURFACES � Noncavitated: Surface intact; use of an explorer to judge surface must be done with caution because excessive force can cause penetration of intact surface over demineralized enamel � Opacity of proximal enamel may be present � Radiolucency may be present � Marginal ridge is not discolored � Opaque area may be seen in enamel by translumination � � Cavitated: Surface broken, detectable visually or tactilely; temporary mechanical separation of the teeth may aid diagnosis � Marginal ridge may be discolored � Opaque area in dentin on translumination � Radiolucency is present. �

Developmental stages of enamel carious lesion correlated with radiographic and clinical examination. (Darling Al: Brit Dent J 107: 287, 1959)
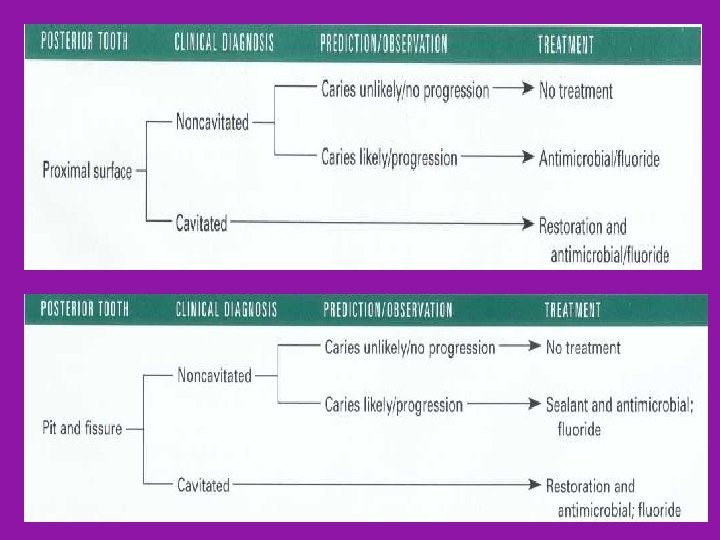

New Caries Treatment Based on the Medical Model
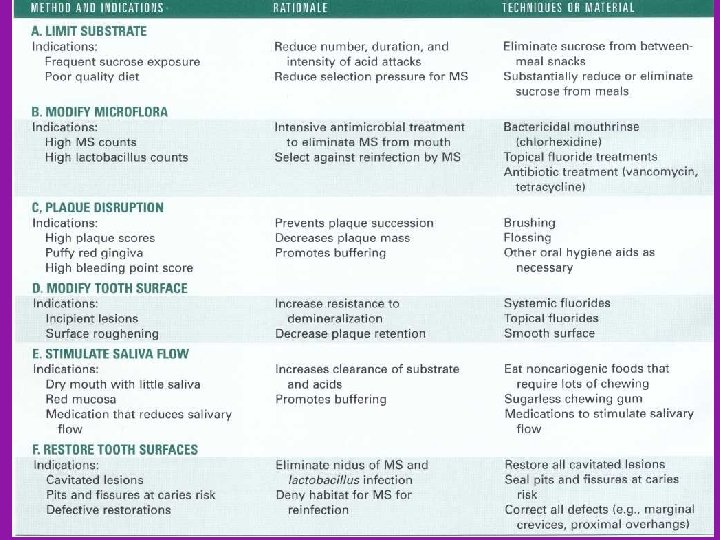

PREVENTION OF DENTAL CARIES

Prevention of dental caries Limit Tooth Demineralization Limit Microbial Growth Oral hygiene Dietry modifications Antimicrobial agents Immunizations Saliva function Xylitol gums Increase Resistance Of Tooth To Deminerelization Fluorides (systemic &topical) Pit and fissure sealants Preventive resin restoration Air abrasion

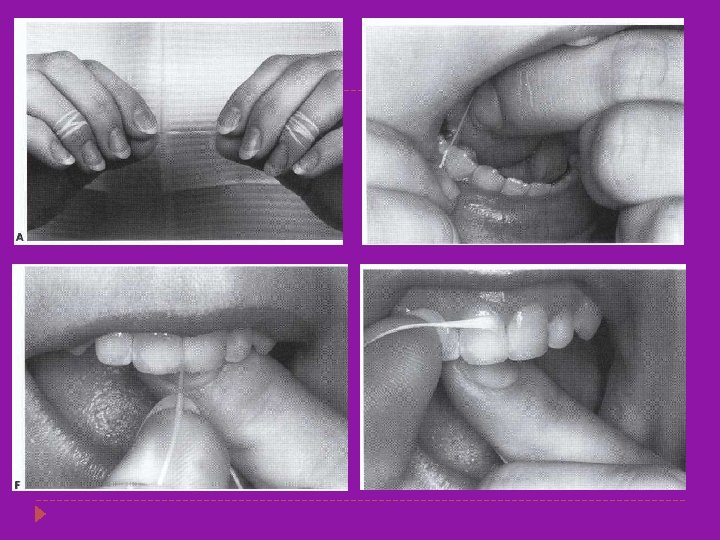
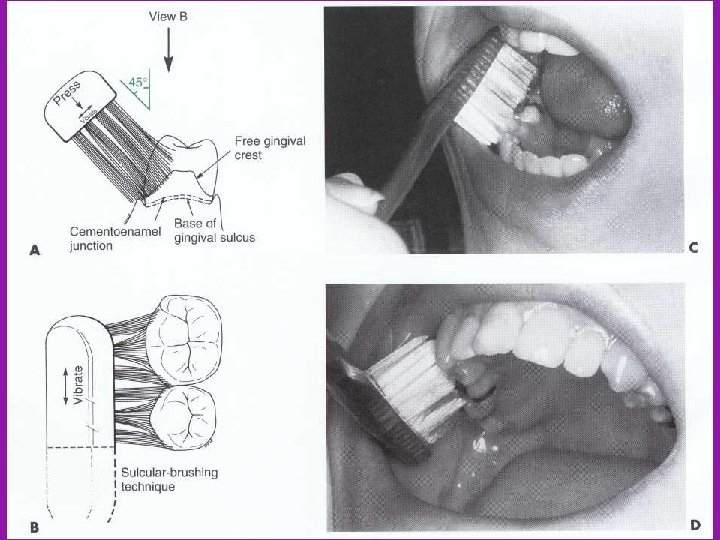
Oral hygiene � Daily removal of plaque by tooth brushing, flossing &rinsing � Floss: purpose to remove plaque from proximal tooth surfaces � Mechanical plaque removal changes the species composition of plaque &denies habitat to potential pathogens

Dietary Modifications � Identify source of sucrose in diet and reduce the frequency of uptake � Caries activity stimulated more by frequency rather than quantity � Sugar free foods or snacks may be advocated Substitution of alchohol based sugar

Salivary functions � Saliva is a natural defence against caries � Protective properties of saliva are: � Bacterial clearance � Buffer properties � Antibacterial properties � Xerostomia increases caries susceptibility � Salivary stimulants ( gums, paraffin or salivary substitute)to patient with impaired salivary functions.

� Xylitol gums : � Natural five carbon sugar � Acts directly on bacteria � Gets substituted for fructose in bacterial metabolism cycle � Environmental shift favouring nonpathogenic bacteria � Immunization: � Caries vaccine primarily based on Ig. A immunoglobulin Certain limitations: � potential side effects � concerns of possible reaction with cardiac tissues � cost

Pit and fissure sealants � Specifically designed for caries prevention in pit and fissure areas bcoz fluorides more effective in prevention of smooth surface caries � Three important preventive effects: � Mechanical filling of pits and fissures with acid resistant resin � Filled pits no longer habitat for MS and other oral bacteria � Render pits easy to clean Pit and fissure sealants

Indications for Use of Sealants

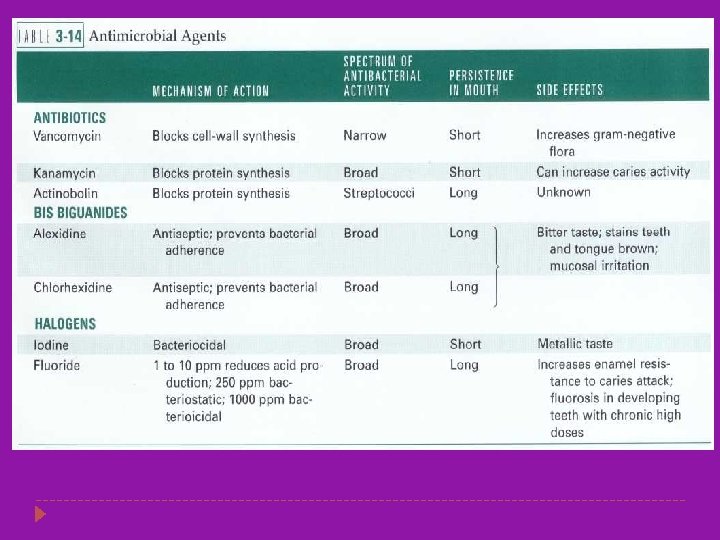
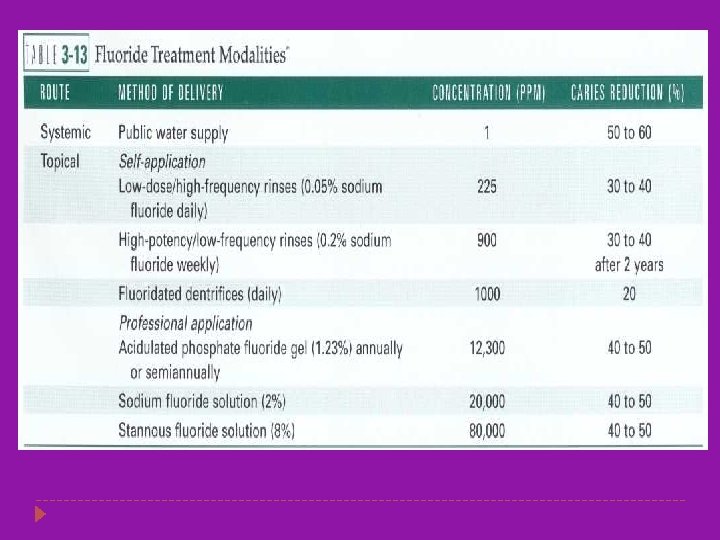
Fluoride Exposure � Flouride in trace amount increase the resistance of tooth to demineralization � Exerts anticaries effects by three mechanism: � Enhances precipitation of fluorapatite , less soluble & more acid resistant � Inhibits enzymatic glycosyltransferase prevents glucose from forming extracellular polysacchridre- reduces bacterial adhesion In high concentration � Directly toxic to oral microorganisms

Thank you
- Slides: 94