Demystifying Growing pain Abhisek Naskar Senior resident Dept

Demystifying Growing pain Abhisek Naskar Senior resident Dept. of Paediatrics Diamondharbour Govt. Medical College& Hospital

Introduction �Described first in French literature in 1823 �Marchel Duchamp termed it as Maladies de la Croissance (pain of growth)

Epidemiology �Most common cause of recurrent musculoskeletal pain in children. �Prevalence : 3 -37% �M: F = 1: 1 �Age group = 4 -14 years

Diagnostic criteria Naish & Apley criteria �Intermittent lower limb pain for 3 months. �Not specifically located in joints. �Sufficient severity to interrupt sleep

Diagnostic criteria �Peterson criteria Characteristic s of pain Inclusion criteria Exclusion criteria Frequency & Duration Intermittent pain once/ twice per week, rarely daily Pain free in between episodes Each lasting for 30 mins to 2 hours Pain, that is persisting or increasing in severity with time Site Calf muscles, ant thigh muscles, a) Pain involving joints shins and popliteal fossa b) Pain in only one Affects both limb Time Evening & Nights Daytime / Nocturnal pain persist till next morning O/E Normal Signs of inflammation

Differential Diagnosis Condition Diseases Injury related Inflammation of Soft-tissue or bone due to sports injuries or accidental injuries or battered child syndrome, Osgood-Schlatter disease, Chondromalacia Patella Infection related Osteomyelitis, Septic arthritis, Cellultis and soft tissue abscess tumors Benign: Osteoid osteoma, Unicameral cyst, Fibrous dysplasia, Aneurismal bone cyst, Gaint cell tumor, Histiocytosis X and Osteochondroma, Malignant: Osteosarcoma, Ewing’s sarcoma,

Differential Diagnosis Condition Disease Developmenta l & congenital others Slipped capital femoral epiphysis, Hypermobile joints, Limb deformities such as genu valgum, flat foot, Discoid lateral meniscus, Patellar subluxation Legg-Calve-Perthes disease, Osteochondritis dissecans, Sickle cell crisis, Amplified musculoskeletal pain syndromes, Restless leg syndrome, Juvenile idiopathic arthritis

Red flag signs �Involvement of joints �Systemic involvement �Persisting pain or day time pain that can be localized �limping

Etiopathogenesis Anatomical /Mechanical � Growing pain often associated with hypermobilty � Association with orthopedic defects like flat foot, knock knee, bad stance[1] � Mechanical instability has been suggested as a cause[2] � Shoe inserts reduces growth pain. [3] 1. Hawksley JC. The nature of growing pains and their relation to rheumatism in children and adolescents. BMJ. 1939; 1: 155 -7. 2. Pavone V, Lionetti E, Gargano V, Evola F, Costarella L, Sessa G. Growing Pains: A study of 30 cases and a review of literature. J Pediatr Orthop. 2011; 31: 606 -9. 3. Evans AM. Relationship between growing pain and foot posture in children: single case experimental design in clinical practice. J Am Pediatr Med Assoc. 2003; 93: 111 -7.

Etiopathogenesis Fatigue � Often reported on days of increased activity. � Represents relative local overuse syndrome[1] � Bone strength in children with growth pain is significantly low than population norm[2] 1. Lowe RM, Hashkes PJ. Growing pains: a noninflammatory pain syndrome of early childhood. Nat Clin Pract Rheumatol. 2008; 4: 542 -9. 2. Friedland O, Hashkes PJ, Jaber L, Cohen A, Eliakim A, Wolach B, Uziel Y: Decreased bone strength in children with growing pains as measured by quantitative ultrasound. J Rheumatol 2005, 32: 1354 -1357.

Etiopathogenesis Lower pain threshold � Growing pain may represents non inflammatory pain amplification syndrome � Children with growth pain have low pain threshold than population norm[1] � Persistence of symptoms associated with low pain threshold[2] 1. Haskesh PJ, Friedland O, Jaber L, Cohen A, Wolach B, Uziel Y. Decreased pain threshold in children with growing pains. J Rheumatol. 2004; 31: 610 -3. 2. Pathirana S, Champion D, Jaaniste T, Yee A, Chapman C. Somatosensory test responses in children with growing pains. J

Etiopathogenesis Psychosocial �‘PHYSICAL GROWTH IS NOT PAINFUL, BUT EMOTIONAL GROWTH CAN HURT LIKE HELL’ -John Apley � Painful experiences during the parents' childhood are a precipitating factor for development of a pain syndrome among their children[1] 1. Oster J, Neilsen A. Growing pains: clinical investigation of a school population. Acta Pediatr Scand. 1972; 61: 329 - 34.

Etiopathogenesis Blood perfusion changes � The sudden onset and severity of GP as well as the transience of the attacks support a hypothesis that GP has a vascular perfusion component, similar to migraines. � Higher prevalence of GP was found among children with migraine headaches [1] 1. Aromaa M, Sillanpaa M, Rautava P, Helenius H: Pain experience of children with headache and their families: a controlled study. Pediatrics 2000, 106: 270 -275.

Growing pain: A Misnomer? ? ? !!!!! �Peak age of growth pain corresponds to relatively slower growth period. �Pain mainly occurs over diaphyses rather than epiphyses.

Management �Clinical diagnosis. �Self limiting �In shoe inserts & triplane wedges found effective. �Muscle stretching exercises.

Muscle stretching exercises STANDING HAMSTRING STRETCH QUADRICEPS STRETCH

Muscle stretching exercises QUADRICEPS ISOMETRIC HEEL STRETCHING

Vitamin D and Growing pain Ben Mc. Naughten et al. Is vitamin D useful in the treatment ofgrowing pains? Arch Dis Child 2017; 0: 1– 3. doi: 10. 1136/archdischild-2017 -313796

BENIGN JOINT HYPERMOBILITY SYNDROME
 is the occurrence of musculoskeletal symptoms in hypermobile")
Definition �Benign joint hypermobility syndrome (BJHS) is the occurrence of musculoskeletal symptoms in hypermobile individuals in the absence of systemic rheumatologic disease

Epidemiology �Prevalence : 4 -13% �Female > Male �Diminishes with age �African, Asian, Middle eastern descent mostly affected

EDS with hypermobilty Hypermobilit y syndromes Hypermobility

Pathology Muscle Loose joints Strain on muscle ligaments tendon Tearing and spasm Pain around joints

Pathogenesis � Strong genetic component with AD pattern � 10 relatives identified in 50% cases. � Abnormality of collagen / ratio of collagen subtypes. � Tenascin X( interacts with type 1 collagen and enhances fibril formation) mutation causes hypermobility in experimental animals. [1] � Mutations in the fibrillin gene have also been identified in families with BJHS[2] 1. Minamitani T, Ikuta T, Saito Y et al. Modulation of collagen fibrillogenesis by Tenascin x and type VI collagen. Exp Cell Res. 2004; 298: 305 -15 2. Magnusson SP. Viscoelastic properties and flexibility of the human muscle– tendon unit in benign joint hypermobility syndrome. J Rheumatol. 2001; 28: 2720– 2725.

Clinical features 1. Pain around the joints �Any joint can be involved with strain of soft tissues around joints causing pain. �Chronic neck strain �Low back pain �Piriformis syndrome: stained piriformis muscle pinching sciatic nerve mimicks nerve root compression by prolasped disc.

2. Neuropathic pain �Associated with disc prolapse �Often psychological 3. Tendonitis �Tennis elbow/Golfer’s elbow 4. Chondromalacia �Wearing of articular cartilage around knee joint.

5. Costochondritis 6. TM joint loosening

Extra articular manifestation Autonomic instabilty Joint hyper mobility Stretchy blood vessels Always on the go & Ignorance of fatigue Chronic fatigue syndrome Over production of adrenaline • Orthostatic intolerance • Neurally mediated hypotension • Postural orthostatic tachycardia syndrome

CVS �Mitral valve prolapse �Cold hand feet �Increased chance of varicose vein, migraine, hemorrhoids GI �Gastro esophageal reflux �IBS �Delayed gastric emptying

Neurobehavioral �Anxiety and overreaction �Poor sleep quality Genitourinary �Uterine prolapse �Cystocele / Rectocele �Vaginismus �Interstitial cystitis

DIAGNOSIS

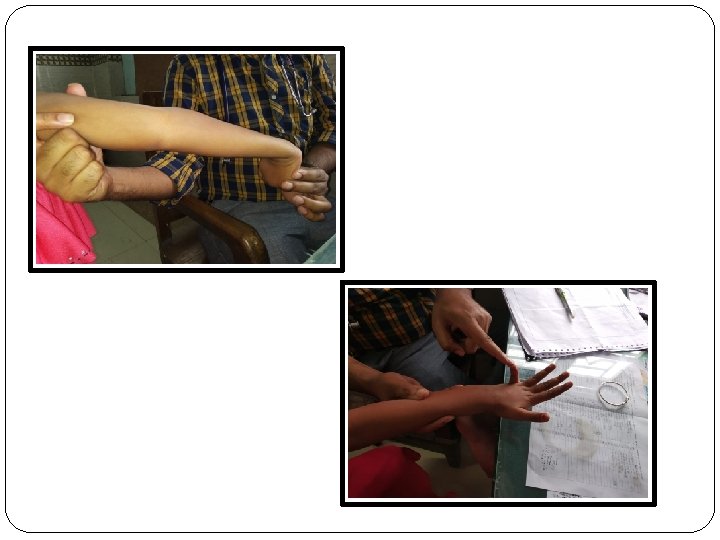
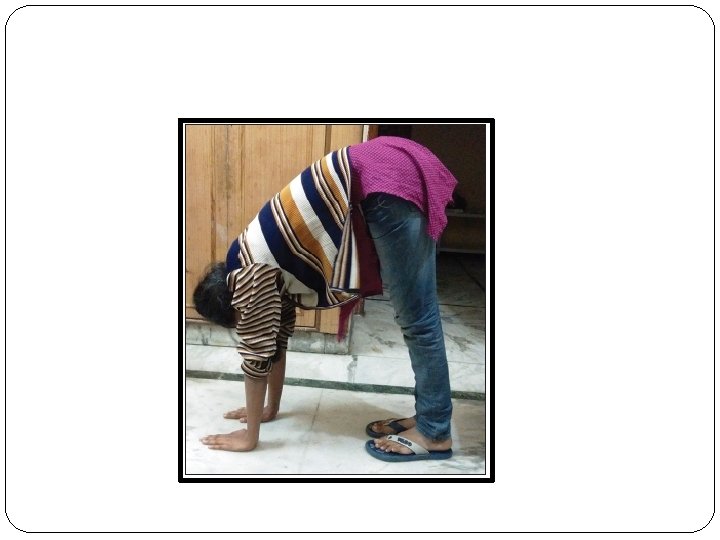
Questions physician should ask to detect joint hypermobility � Can you now (or could you ever) place your hands flat on the floor without bending your knees? � Can you now (or could you ever) bend your thumb to touch your forearm? � As a child, did you amuse your friends by contorting your body into strange shapes or could you do the splits? � As a child or teenager, did your shoulder or kneecap dislocate on more than one occasion? � Do you consider yourself double-jointed? Hakim AJ, Cherkas LF, Grahame R, Spector TD, Mac. Gregor AJ. The genetic epidemiology of joint hypermobility: A population study of female twins. Arthritis Rheum. 2004; 50: 2640– 2644.

Beighton score Assessment site Left Hyperextension of elbow >100 1 Hyperextension of 5 th MCP 1 Hyperextension of knee joint>100 1 Thumb touching forearm 1 Maximum possible score Hand touching floor with full palms with Knee extended Hypermobility if score Right 1 1 9 ≥ 4 1


Brighton criteria & interpretetion

Neuromusculoskeletal sign and potential sequalae of joint hypermobility

Differential diagnosis Ehlers Danlos syndrome �AD �Skin hyperelasticity and fragility �Papyraceous scar Marfan syndrome �AD �Tall, Thin (Marfanoid habitus) �Cardiac and ocular features JRA �Inflammatory involvement of joints

Management �For acute symptoms – analgesics for pain control �For moderate or severe pain, rest and abstaining from aggravating activities may improve �Physical therapy and joint protection may help

Long Term Management �Modification of activities �Stretching technique to isolate tight muscles �Strength training �Supportive splints along with appropriate footwear �Osteopathic Manipulative Treatment – no more than 3 times per week

Prognosis �Non progressive �Benign!!!!! – sequalae may have potential effects on quality of life

Take home message �Growing pain is the most common cause of chronic musculoskeletal pain in children. �Vitamin D should be supplemented if there is deficiency/insufficiency �Joint hypermobility is the most common finding in chronic musculoskeletal pain in children.

THANK YOU

When the historyand physical examination for a child with lower extremity pain fit the classic description of growing pains, explanation and reassurance from a health care provider are generally all that is needed. For children with an atypical history or with concerning physical examination findings, clinicians should pursue additional evaluation.
- Slides: 46