Delirium How Emergency Physicians Can Make a Big

Delirium How Emergency Physicians Can Make a Big Difference Alan Bates, MD, Ph. D, FRCPC Consultant Psychiatrist St. Paul’s Hospital and the BC Cancer Agency Clinical Assistant Professor Department of Psychiatry University of British Columbia

In 1959… § Engel and Romano § “…while most physicians have a strong bias toward an organic etiology of mental disturbances, … they seem to have little interest in … the one mental disorder presently known to be based on derangement of cerebral metabolism. ” § “… deficiencies in the education of many physicians ill equip them to recognize any but the most flagrant examples of delirium…”

In 1959… § Engel and Romano continued § “Only … a management problem on a medical or surgical service is likely to result in a psychiatric consultation. ” § “[The psychiatrist] … seeing the patient in the home territory of the “organic” specialists … is less likely or able to pursue an understanding of the underlying physiologic derangements, which are generally conceived to be the proper domain of the internist. ”

In 1959… § Engel and Romano continued § “Unhappily, the unfortunate patient’s malfunctioning brain rests in limbo, an object of attention and interest neither to the medical man nor to the psychiatrist. ” § “Not only does the presence of delirium often complicate and render more difficult the treatment of a serious illness, but also it carries the serious possibility of permanent irreversible brain damage. ”

In 1959… § Engel and Romano continued § “With increasing life expectancy … we are now beginning to see an increasing incidence of so-called senile and arteriosclerotic dementias. ” § “The physician who is greatly concerned to protect the functional integrity of the heart, liver, and kidneys … has not yet learned to have similar regard for the functional integrity of the brain. ”

From Cresswell III et al. Organic Age Functional < 12 or > 40 years old 12 – 40 years old Sudden Gradual Consciousness Decreased Normal Hallucinations Visual Auditory Course Fluctuates Continuous Orientation Disoriented Scattered thoughts Abnormal No Yes Onset Vitals Psych Hx

DSM-5 Criteria § Disturbance in attention and awareness § Develops over short time, change from baseline, fluctuates in severity over course of a day § An additional cognitive disturbance (e. g. memory, orientation, language, visuospatial, perception) § Not another neurocognitive disorder, not coma § Direct consequence of another medical condition

Meagher et al. , 2007 § 100 palliative care patients § Attention – 97% (e. g. distractibility, digit span) § Sleep-wake cycle – 97% (? cause of fluctuation, early) § § § § Long-term memory – 89% Short-term memory – 88% Orientation – 76% (misses ¼) Visuospatial ability – 87% Motor agitation – 62% (early) Motor retardation – 62% (early) Language – 57% Perceptual – 50% (motor agitation = retardation)
 §")
Incidence § Hospitalized elderly patients – 25% (van Blanken et al. , 2005) § ICU – 70% at some point (Mc. Nicoll et al. , 2003) § 30% of critically ill children (Smith et al. , 2013) § Post-operative delirium in patients over 60 after cardiac surgery – 52% (Rudolph et al. , 2009) § Terminal illness – 88% (Massie etl al. , 1983; Lawlor et al. , 2000)

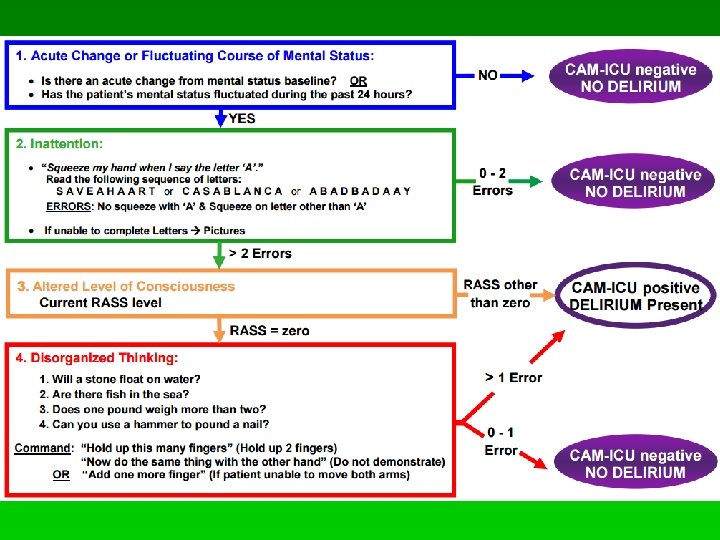
Incidence and detection - ER § Elie et al. , 2000 § 10% of 447 ER patients over 65 delirious § Detection by ED physician § Sensitivity: 35%, Specificity: 99% § Han et al. , 2014 § 12% of 406 ER patients over 65 delirious § Detection by ED physician using CAM-ICU § Sensitivity: 72% (better than RAs) § Specificity: 99% § Han et al. , 2014 § CC of “altered mental status”: 38% sensitivity, 99% specificity (when not coma, non-verbal etc. )
 § Clear immediate increase in suffering")
Impact (reviewed by Maldonado et al. , 2009) § Clear immediate increase in suffering of patient and family § Increased morbidity and mortality § Prolonged hospital stays § Increased cost of care § Increased hospital-acquired complications § Poor functional and cognitive recovery § Decreased quality of life § Increased placement in intermediate- and long-term care facilities

Impact – ER specific § Han et al. , 2010 / 2011 § 628 ER patients over age 65 § 17% delirious § 6 -month mortality: § 37% in delirious group § 14% in non-delirious group § Median length of stay: § 2 days for delirious § 1 day for non-delirious

Distress § Rate of diagnosable PTSD was 9. 2% at 3 months post-ICU in 238 post-ventilated patients with a strong association between PTSD and recall of delusional memories (Jones et al. , 2007) § Delirium is even more distressing for spouses than for patients (Breitbart et al. , 2002)

Milbrandt et al. , 2004 § 224 consecutive mechanically ventilated ICU patients (after excluding 51 with coma leading to death) § 82% developed delirium, mean duration 2 days

Barrough, 1601 “It commeth to passe also that the soporiferous diseases being ended, there ensueth forgetfulnesse: which when it chanceth then a cold distempure is the cause that the memorie is perished or grievously hurt. ”

Maclullich et al. , 2009 § Reviewed 9 recent studies with total of 2025 patients § 8/9 studies found a significant association between delirium and cognitive impairment § What is the relationship? § CNS insult causes both in parrallel? § Premorbid dementing process unmasked in form of delirium by stress/insult? § Delirium causes things like dehydration, poor nutrition, suboptimal care etc. and this leads to longterm cognitive impairment? § Delirium is a neurotoxic state? § Delirium management is neurotoxic?

Witlox et al. , 2010 § Meta-analysis of elderly patients with delirium § Delirium associated with increased risk of death (38% vs. 28% in controls at average follow-up of 23 months) § Delirium associated with increased risk of institutionalization (33% vs. 11% in controls at average follow-up of 15 months) § Delirium associated with increased risk of dementia (63% vs. 8% in controls at average follow-up of 4 years) § Above results are independent of age, sex, comorbid illness, illness severity, and baseline dementia
 Hypoxia")
Risk factors § Infection § § § Withdrawal Acute metabolic Trauma CNS (structural) Hypoxia § § § Deficiency of vitamins Endocrine Acute vascular Toxins/Medications (Lexicomp is your friend) Heavy metals

Deleriogenic Medications § Anticholinergic § e. g. diphenhydramine, hydroxyzine, atropine, amitriptyline, imipramine, paroxetine, doxepin, furosemide, prochlorperazine § Benzodiazepines § Barbiturates § Opiates § Especially meperidine § ? Morphine > Hydromorphone > Oxycodone (rotation can help) § Incontinence meds § e. g. oxybutynin § Cardiac meds § e. g. digitalis, quinidine, procainamide, lidocaine, beta-blockers § GI meds § H 2 -blockers (e. g. cimetidine, ranitidine), PPIs, metoclopramide § Many others: e. g. phenytoin, steroids
: 8139 consecutive patients undergoing CABG")
Cardiac Surgery Risk Factors § Giltay et al. (2006): 8139 consecutive patients undergoing CABG and/or valve procedure § Post-op psychotic symptoms associated with age, renal failure, dyspnea, heart failure, and LVH pre-operatively and hypothermia, hypoxemia, low hematocrit, renal failure, high sodium, infection, and stroke perioperatively

Sockalingam et al. 2005

van der Mast et al. , 1996 § “Of all the reported differences in the studies, only year of publication is significantly related to the incidence of delirium after cardiac surgery, the later publications showing a tendency towards a lower incidence. ” § “… a cautious conclusion may be drawn that no strong risk factor has been identified…”
 § Acetylcholine § Anticholinergic drugs induce delirium §")
Pathophysiology: Neurotransmitters (Reviewed by Trzepacz, 1994) § Acetylcholine § Anticholinergic drugs induce delirium § Correlation between poor cognitive function and serum anticholinergic level § Serum anticholinergic levels decrease as delirium resolves § Reversal of anticholinergic delirium with physostigmine
 § Dopamine § Effective treatment with dopamine receptor")
Pathophysiology: Neurotransmitters (Reviewed by Trzepacz, 1994) § Dopamine § Effective treatment with dopamine receptor blockers like loxapine or haloperidol § Norepinephrine § Glutamate § Serotonin § GABA § Histamine
")
Pathophysiology (Maldonado, 2008)

Pathophysiology
: motor activity at the wrist over five")
Wrist actigraphy § Osse et al. (2009): motor activity at the wrist over five 24 hr cycles after elective cardiac surgery

Jacobson et al. , 2008 § Elderly delirious postoperative patients: § Fewer nighttime minutes resting § Fewer minutes resting over 24 hrs § Greater mean activity at night § Smaller change in activity from day to night § Delirium may be simultaneous wakefulness and sleep § REM intrusion into wakefulness might cause visual hallucinations

Slatore et al. , 2012 § Assessed sleep quality and screened for delirium in veterans referred to hospice (55% had cancer) using the Pittsburgh Sleep Quality Index (PSQI) and the Confusion Assessment Method (CAM) § Sleep quality was significantly worse in 33 participants who became delirious than in 42 who did not § Hazard ratio for developing delirium of 2. 37 for every point of worse sleep on the PSQI (where 1 = very good; 4 = very bad)
 demonstrated that sleep is associated with a")
Glymphatic system § Xie et al. (2013) demonstrated that sleep is associated with a 60% increase in the interstitial space causing striking increase in exchange between CSF and interstitial fluid § Increased rate of β– amyloid clearance

Definitive treatment: § Find the underlying cause or causes and treat it/them
 § In a study of 852 elderly")
Non-pharmacological interventions (Inouye et al. , 1999) § In a study of 852 elderly patients admitted to a general medical service, Inouye et al. reduced the incidence of delirium from 15% to 9% with a number of non-pharmacological interventions including promotion of sleep with sleep inducing stimuli (e. g. relaxation tapes, warm milk) and a sleep promoting environment (e. g. through noise reduction)
 and after")
Patel et al. , 2014 § Screened for ICU delirium before (n=167) and after (n=171) implementing measures to promote sleep § Noise and light reduction at night, minimize care that interrupts sleep at night, reduce daytime sedation when possible, address pain early, early mobilization § Found reduced incidence (14% vs. 33%) and duration (1. 2 vs. 3. 4 days) of delirium

Maldonado et al. , 2009 § 90 patients who underwent valve procedures randomly assigned to post-op sedation with dexmedetomidine, propofol, or midazolam (From Aantaa & Jalonen, 2006)

Maldonado et al. , 2009 § Incidence of delirium was 50% for both propofol and midazolam groups and only 3% for dexmedetomidine group § Possible benefits of dexmedetomidine: not GABAergic, not anticholinergic, sedating, promotes physiologic sleep pattern without significant respiratory depression, lowers opioid requirements
 demonstrated decreased incidence of delirium in older adult")
Melatonin § Al-Aama et al. (2011) demonstrated decreased incidence of delirium in older adult patients on a general medicine unit who received 0. 5 mg of melatonin nightly § Evidence that melatonin could actually aid in treating ongoing delirium is mostly limited to case studies (e. g. Hanania and Kitain, 2002) § Other findings suggest melatonin isn’t helpful (e. g. Ibrahim et al. , 2006)

Haloperidol § § § Standard treatment in most places Relatively little anticholinergic effect Little effect on orthostatic hypotension Less sedation good for hypoactive delirium Risk of QT prolongation Relatively high risk of extrapyramidal effects § No difference between IV and PO § Menza et al. (1987) and Maldonado (2000) both seriously flawed § Are reports of EPS with IV (Blitzstein & Brandt, 1997) § Small doses (e. g. 0. 5 mg IV BID or 1 mg IV QHS)
 is frequently cited")
Chlorpromazine § The double-blind randomized trial by Breitbart et al. (1996) is frequently cited as evidence haloperidol should be chosen over other antipsychotics § However, the findings showed the superiority of both haloperidol and chlorpromazine (a sedating low-potency antipsychotic) over lorazepam while showing equal effectiveness between the two antipsychotics § Sedating antipsychotic with IV option § An example of dosing: chlorpromazine 25 mg IV Q 6 H standing (give over 30 min; hold for SBP < 90; hold for sedation)

Methotrimeprazine § § § Also sedating and can be given SC or IV Significant analgesic effect Need to be cautious of hypotension e. g. 5 - 10 mg Q 1 H PRN for agitation Can go as high as 50 mg Q 4 H

Quetiapine § When we use low dose quetiapine at night, it’s primarily acting as an antihistamine § Maneenton et al. (2013) found no difference between 25 -100 mg/day of quetiapine HS and 0. 5 -2 mg/day of haloperidol HS in a double-blind, randomized trial of delirious patients eliciting CL consult § e. g. quetiapine 25 mg PO QHS § e. g. quetiapine 50 mg PO QHS § Caution re orthostatic hypotension

Olanzapine § A number of studies also support use of olanzapine (e. g. Breitbart et al. , 2002; Skrobik et al. , 2004; Grover et al. , 2011) § e. g. Olanzapine oral dissolving 2. 5 mg QHS § e. g. Olanzapine oral dissolving 5 mg QHS § § § Promotes appetite Reduces nausea Promotes sleep § Pro-cholinergic at lower doses, but becomes anticholinergic at larger doses
 § In 31 patients over 55 with post-operative")
Loxapine (Bates et al. , submitted) § In 31 patients over 55 with post-operative delirium referred to the CL service, loxapine was associated with a mean decrease of 8. 48 on the DRS-98 -R over the first 2 days of treatment § Only 3 participants had a worsening of delirium, and each of those 3 showed improvement from day 2 to day 4 § Mean number of days to resolution of delirum (DRS < 10) was 3. 2 § There was not a significant increase in QTc
")
Loxapine (Bates et al. , submitted)

Terminal Illness § Delirium interferes with identification of sources of distress like pain § How much should one investigate? § Definitive etiology discovered in less than 50%, and often irreversible when found (Bruera et al. 1992) § However, Tuma and De. Angelis (1992) report 68% can be improved even when 30 -day mortality is 31% § Lawlor et al. (2000): § 49% reversibility in advanced cancer patients admitted to palliative care § Reversibility associated with opioids, other meds, and dehydration being primary causes

Terminal Illness § Some view delirium as natural part of dying process § Some worry that antipsychotic will make patient more delirious § Evidence is that antipsychotic generally safe and effective at reducing distress § “Unfortunately, the hallucinations in delirium are rarely sugarplum fairies. ”

- Slides: 47