Delicate Normal pulp connective tissue with tiny blood


► Delicate Normal pulp connective tissue with tiny blood vessels, lymphatics, nerves, and undifferentiated connective tissue cells.

Significances of pulp anatomy in inflammation -The pulp is enclosed within unyielding walls of dentine. -Nerves, arteries and veins enter through a small apical foramen. -Lack of collateral circulation. -The pulp responds very definitely to sudden temperature changes. -The pulp lacks the power of regeneration.
. ► Non-living irritants.")
Aetiological factors of pulp disease ► Living irritants (microbial). ► Non-living irritants.
 Microorganisms may gain entrance into the pulp through: ►An open cavity.")
Living irritants (microbial) Microorganisms may gain entrance into the pulp through: ►An open cavity. ►Gingival crevice and periodontal ligament. ►Extension of periapical infection from adjacent infected teeth. Haematogenous infection (anachoresis).

Non-living irritants Physical: Mechanical, aeronautical, irradiation. thermal, electrical, Chemical: Acids, alkalis, poisons. Pulp inflammation caused by dentist's procedures referred to as "Odonto-Iatrogenic Pulpitis"

Classification of pulp disease 1. Type of inflammation: a. Focal reversible pulpitis. b. Acute pulpitis. c. Chronic pulpitis. 2. Extent of pulp involvement: a. Partial pulpitis or subtotal pulpitis. b. Total pulpitis or generalized pulpitis. 3. Direct communication between pulp and oral environment: a. Open pulpitis. b. Closed pulpitis:
 is the earliest form of pulpitis. ►")
► It Focal Reversible Pulpitis (Pulp hyperemia) is the earliest form of pulpitis. ► It is a reversible condition provided the irritant is removed before the pulp is severely damaged. Clinical Features: - A tooth is sensitive to thermal changes, particularly cold. - Pain disappears upon removal of the irritant. -Teeth show deep carious lesions, large metallic restorations, or restorations with defective margin

Pathogenesis and Histologic Features *Dilatation of the pulp vessels. *Inflammatory fluid exudates. *The escape of the fluid exudates haemo-concentration increased viscosity blood circulates at a slower rate Thrombosis.

Inflammation Acute Chronic Acute exacerbation Resistance of patient Virulence of irritant

►Follows Acute Pulpitis hyperaemia. ►OR an acute exacerbation of a chronic inflammatory process. ►Cardinal signs of inflammation occur.

Mechanism and Microscopic findings of acute pulpitis l. Starts when the carious products reach the pulp through dentinal tubules and limited to the part of the pulp directly below carious lesion (partial acute pulpitis). In cases of continuing or increasing irritation, abscess formation occurs. l Abscess formation occurs when the entrance to the pulp is minute and drainage is inadequate. l

► Abscesses can be formed in different parts of the pulp at the same time the whole pulp is transformed into a dead mass of tissue (total suppurative pulpitis).
.")
► Vascular dilatation. ► Congestion of blood vessels. ► Pavementing of polymorphonuclear leucocytes (PNL). ► Migration of PNL. ► Fluid leaks out from the capillaries. ► Oedema compress the tissue.

►leukocytes die releasing proteolytic enzymes dissolve the pulp tissue liquefaction necrosis and the production of pus (abscess). ►The first abscess is seen in pulp horns. ►Surrounding the abscess there is a dense mass of lymphocytes, plasma cells and monocytes.

►Swelling of odontoblastic nuclei. ► Disintegration of nuclei. ►Deposition of collagen walling off the infectious material (acting as a local protective barrier). ►If the process enclosed within a collagen wall, this may calcify. ►Towards the normal pulp there are dilated vessels.

Clinical features ►Pain: Severe continuous throbbing pain. Or less severe and intermittent attacks. Severity of pain increases while the patient is lying down and with change in temperature. ► The extreme pain is due to: *Pulp inflammation, oedema is confined in a rigid chamber of dentine. *The products of inflammation such as histamine and serotonin, act upon the nerve endings to produce pain. ► Electric vitality tester: the tooth reacts at lower threshold than normal.

Treatment ► Removal of the cause. ► Pulp capping. ► Or root canal treatment.

Chronic Pulpitis Causes: ► As a sequel of acute pulpitis. ► When the irritant is not severe e. g. : § Organisms are of low virulence. § Caries is progressing slowly. ► The pulp is capped following traumatic exposure. ► Caries is not completely removed from a cavity. ► In normal teeth through haematogenous infection (Anachoretic pulpitis).

Classification ►Chronic closed pulpitis. ►Chronic open pulpitis: § Chronic open ulcerative pulpitis. § Chronic open hyperplastic pulpitis (pulp polyp. ).

Mechanism and microscope findings ► Bacterial toxins reach the pulp via lymph which circulates in the dentinal tubules. ► Toxins irritating odontoblastic processes. ► Odontoblasts lay down new dentine that tends to reduce the access of irritants to the pulp. ► Small numbers of bacteria enter the pulp "pioneer organisms". ► Introduction of lymphocytes and plasma cells. ► Formation of small abscess may occur. ► Capillaries prominent, fibroblastic activity is evident, and collagen fibers form bundles. ► This is an attempt to wall off the infected area.

Clinical features: ► Intermittent dull aching pain. ► Less sensitivity to heat and cold. ► Electric pulp tester: the tooth responds at a higher level than normal.

Treatment ► Root canal treatment ► Or extraction.

Chronic Open Ulcerative Pulpitis *Entire or the greater part of pulp shows chronic inflammatory changes. *In the area of carious exposure the pulp tissue is replaced by granulation tissue. *Oedema escapes through the exposure. *Symptoms: none to a minimum dull pain made worse by thermal changes.
 ► It occurs chronic from onset or as")
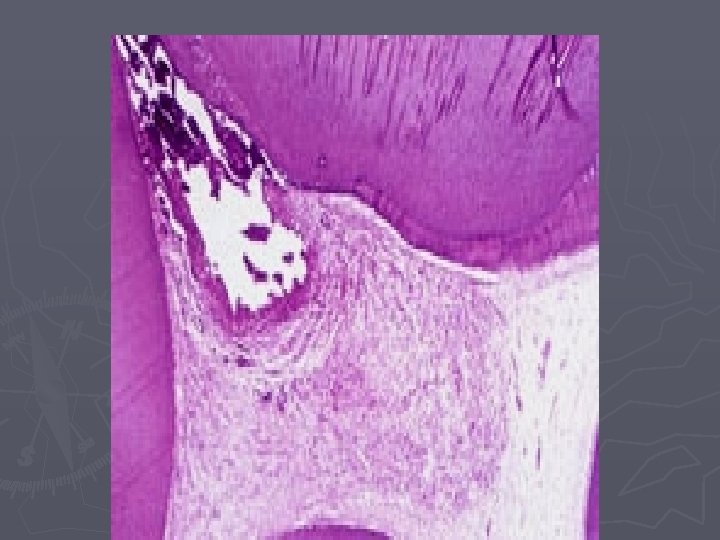
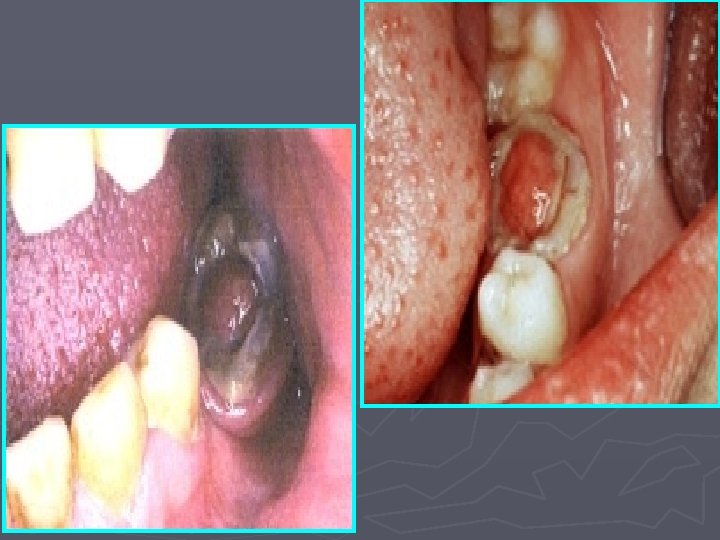
Chronic Open Hyperplastic Pulpitis (pulp polyp) ► It occurs chronic from onset or as a chronic stage of acute pulpitis. ► It occurs particularly in deciduous molars and first permanent molars. ► In which extensive carious lesions lead to wide exposure of the pulp.

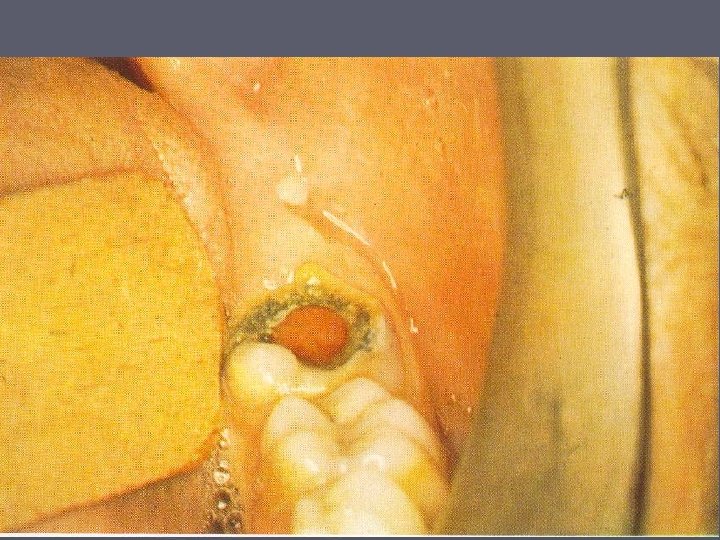
►A Clinical Features globular mass of tissue protruding from the pulp chamber. ► Pinkish or dark fleshy red in color. ► In teeth of children and young adults, with large apical foramina and excellent blood supply. ► When the polyp is young, it bleeds easily. ► With age, the structure may become pedunculated, lobulated. ► On palpation with a probe, it is slightly sensitive but usually it is painless. ► The tooth is vital

Sequence of events ► Caries produces acute pulpitis. However, because of the wide exposure, this does not lead to pulp necrosis but gradually to chronic pulpitis. ► Chronic pulpitis is characterized by formation of abundant granulation tissue. ► The latter protrudes out of the exposure into the cavity. ► Desquamated cells from the oral mucosa get implanted on the granulation tissue and, by rapid proliferation and migration, come to cover the entire surface.
 and")
Microscopic Features ► Vital pulp tissue with chronic inflammatory cells (plasma cells, lymphocytes) and granulation tissue. ► Granulation tissue gets covered by stratified Squamous. ► Source of the epithelium: ► Desquamated epithelial cells of the oral cavity carried by saliva. ► Rubbing against buccal mucosa, tongue or gingival.
 ►Untreated pulpitis may lead to death of the pulp. ►The")
Pulp Necrosis (pulp gangrene) ►Untreated pulpitis may lead to death of the pulp. ►The inflammatory exudates compressed within a hard shell of dentine leads to compression of blood vessels particularly the apical leading to necrosis.

Clinical features ► Cessation of all symptoms. ► Discoloured tooth ► Teeth do not respond to either cold or electric pulp tests ► May range from being asymptomatic to being very sensitive to percussion

Pulp Necrosis Microscopically Either an empty pulp chamber and canals or isolated areas of necrotic structureless masses.

Thank you
- Slides: 35