Deep Vein Thrombosis Sahar Mirbaha Assistant professor of

Deep Vein Thrombosis Sahar Mirbaha, Assistant professor of EM, SBMU

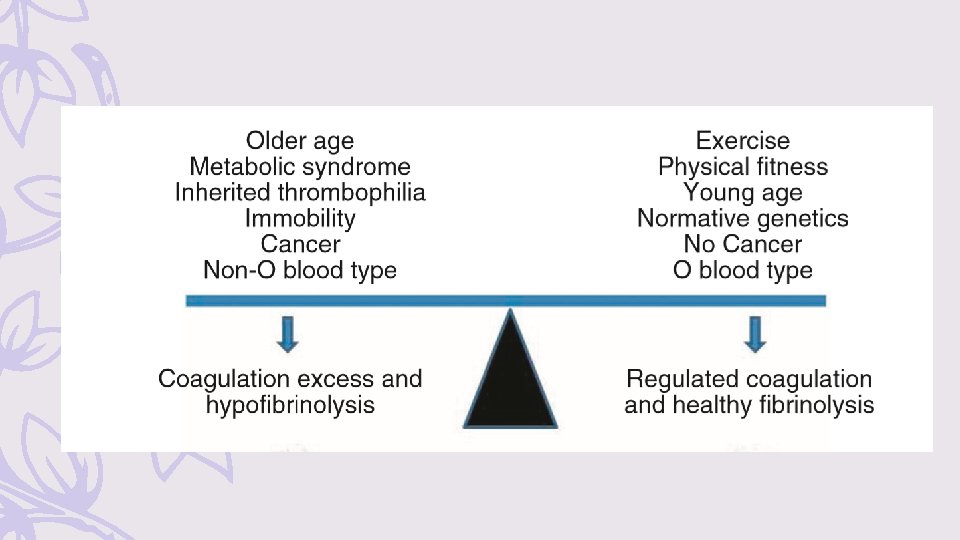
pathophysiology – blood clots form when fibrin production exceeds its elimination – Factors that enhance fibrinogen synthesis include : Ø systemic inflammation Ø traumatic or immune-related vascular trauma Ø inherited thrombophilias and hemoglobinopathies Ø cancer Ø pregnancy sluggish blood flow

The venous anatomy of the lower extremity is divided into the deep and superficial systems Ø The superficial venous system consists primarily of the greater and short saphenous veins and perforating veins Ø The deep venous system includes: – the anterior tibial, posterior tibial, and peroneal veins, collectively called the calf veins – The calf veins join together at the knee to form the popliteal vein, which extends proximally and becomes the femoral vein at the adductor canal
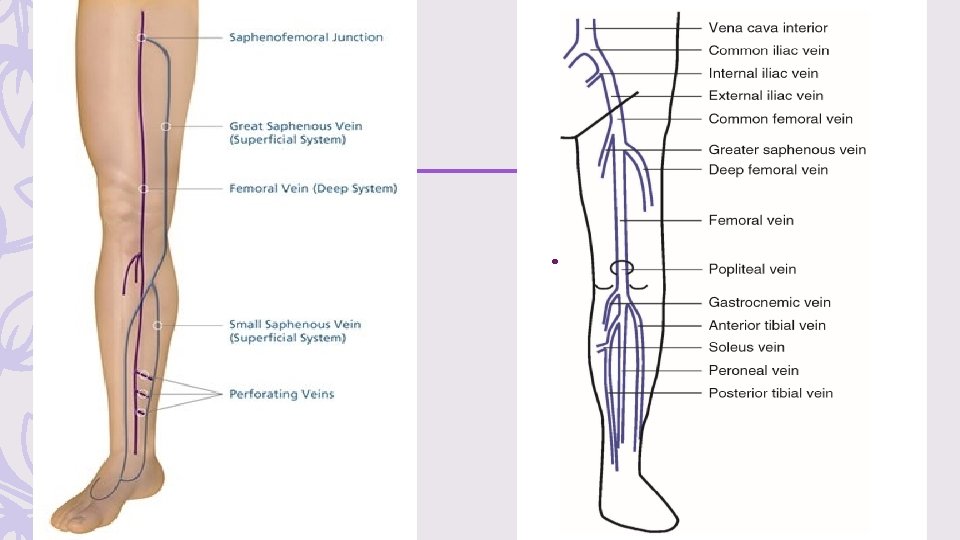

cont – Proximal DVT refers to a clot in the popliteal vein or higher. – whereas distal clot refers to an isolated calf vein thrombosis. – Distal greater saphenous vein clots are sometimes denoted as superficial thrombosis, but greater saphenous clots near its connection with the femoral vein should be referred to and treated as proximal DVT.

US – A two-point venous ultrasound includes the common femoral and popliteal vein. – A three-point ultrasound includes the common femoral, and popliteal veins. – A whole-leg ultrasound includes a three-point ultrasound and the peroneal and tibial calf veins.

Clinical Features – Hallmarks of DVT include unilateral limb pain and swelling – initially subtle and nonspecific symptoms, such as a mild cramping sensation or sense of fullness in the calf, without objective swelling on examination – other clinical signs include: edema, erythema, and warmth of the affected extremity, tenderness to palpation along the distribution of the deep venous system, dilation of superficial collateral veins, and a palpable venous cord.

cont – leg DVT occurs with a slightly higher frequency in the left leg compared with the right (May-Thurner syndrome ) : Y? – bilateral leg DVT is found in fewer than 10% of ED patients – Upper extremity DVT is, a thrombosis in the axillary vein, whereas thrombosis of the brachial vein is a superficial thrombosis. – In the absence of a catheter, the most frequent location of arm DVT is on the dominant hand side Fever suggests an alternative diagnosis, such as cellulitis


DIAGNOSIS 1. Diagnosis of DVT and PE starts with an estimation of the pretest probability (PTP). – Well’s score – One PTP score for pregnant patients, the LEFt score: 1 point in case of left (L) leg suspicion, 1 point for edema (E), and 1 point if the suspicion occurred during the first trimester (Ft) of pregnancy, with a score of 0 or 1 tantamount to a low PTP The PTP dictates the pathway for diagnostic testing

*A score <2 indicates that the probability of deep vein thrombosis is low
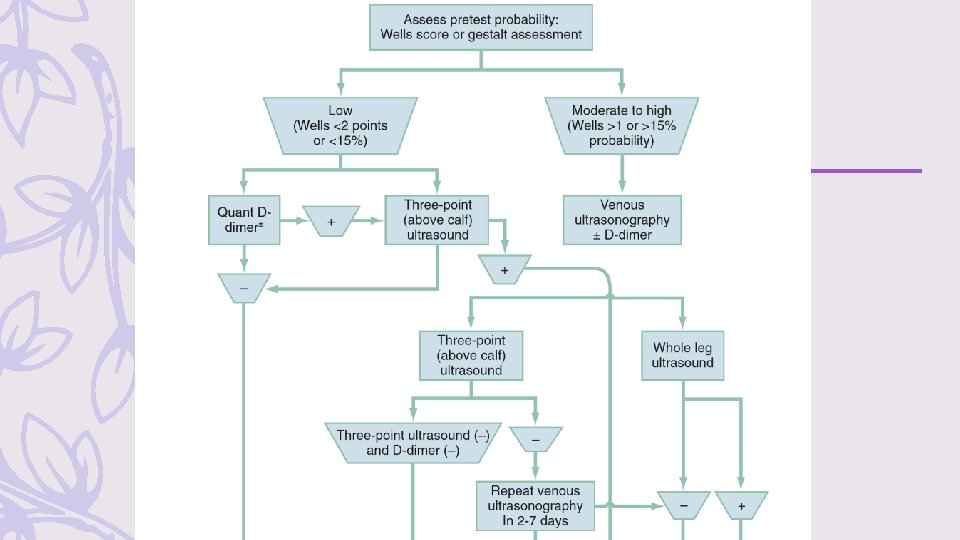

Diagnostic Testing – A normal quantitative D-dimer concentration in a patient with a low PTP can be used to exclude proximal DVT (diagnostic sensitivity ≅ 95%; specificity ≅ 50%). – Venous duplex ultrasonography, is the diagnostic test of choice in most centers. (sensitivity and specificity of approximately 95%, ). – A patient at a low PTP may have the diagnosis of DVT effectively excluded by a negative three-point venous duplex ultrasound, which images the common femoral, and popliteal veins.

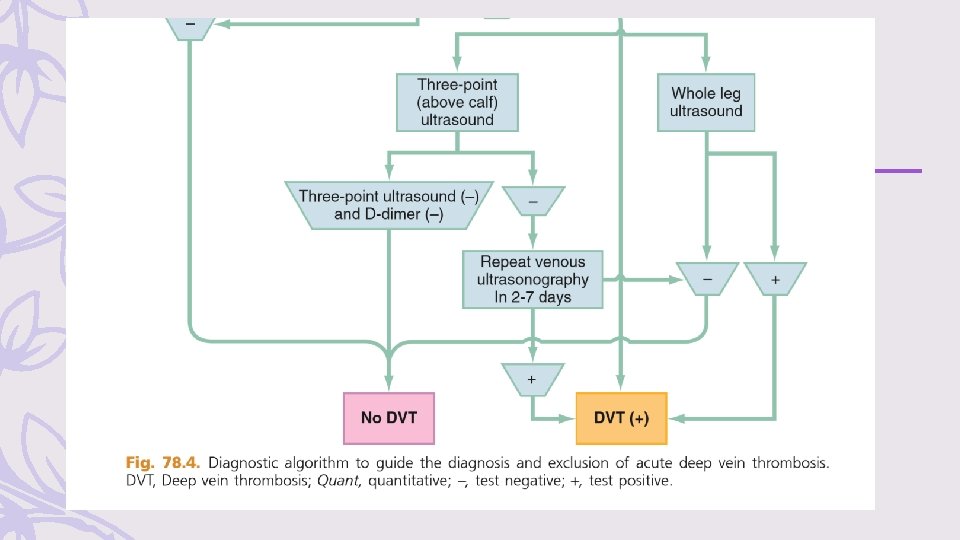
– patients at higher than low risk, a single negative three-point ultrasound is inadequate as a sole method to exclude DVT, whereas a single normal whole-leg ultrasound (including normal calf and saphenous veins) is sufficient to exclude DVT with any PTP. – A negative three-point ultrasound, together with a negative quantitative D-dimer, excludes DVT with any PTP – If a patient with a moderate to high PTP and elevated D-dimer level (or not performed), a negative three-point ultrasound at the index visit should be followed by a repeat ultrasound in 2 to 7 days – If negative, this is sufficient to exclude DVT

– Ultrasound cannot be used to rule out iliac or pelvic vein thrombosis. When duplex ultrasound is not available, – patients with a moderate to high PTP should receive empirical low-molecularweight (LMW) heparin while awaiting the availability of ultrasound imaging – patients with a low or moderate to high PTP with a negative D-dimer do not need empirical anticoagulation while they wait for diagnostic imaging

MRI – MRI is a logical option to evaluate the pelvic veins of patients at high risk for pelvic vein thrombosis (eg, those with gynecologic malignancy) and for pregnant patients – MRI is not the primary diagnostic test for patients with suspected DVT

Management Most patients with DVT can be treated at home Ø anticoagulation should be initiated emergently, unless contraindicated Ø patients should be encouraged to ambulate after anticoagulation for DVT to reduce the incidence of postthrombotic syndrome Ø Compression stockings can no longer be advocated routinely for DVT, although patients with persistent swelling or superficial thrombosis may benefit.

Superficial Leg Thrombophlebitis – patients with a clot in the greater saphenous vein that extends above the knee are at risk for progression to DVT – distal saphenous vein thrombophlebitis can adequately be treated with nonsteroidal antiinflammatory drugs, heat, and graded compression stockings, followed by a scheduled repeat ultrasound in 2 to 5 days – greater saphenous vein clot is proximal, near the connection with the femoral vein, anticoagulation is indicated full-dose LMW heparin or fondaparinux for 10 days followed by a repeat ultrasound If the repeat ultrasound shows improvement, anticoagulants can be discontinued

Isolated Calf Vein Thrombosis – it is clear that anticoagulation lowers the rate of proximal propagation and embolization – For tibial or peroneal vein thrombosis in an otherwise healthy ambulatory patient, with no other indications for anticoagulation, the recommendation is : short-term anticoagulation, most easily accomplished with rivaroxaban (15 mg bid for 14 days then 20 mg QD) or apixaban (10 mg bid for 7 days, then 5 mg bid for 7 days), or antiplatelet therapy with aspirin (325 mg/day of enteric-coated acetylsalicylic acid) and close follow-up with repeat duplex ultrasound scan at 2 to 5 days to evaluate for clot propagation.
 – Massive iliofemoral vein occlusion results in swelling")
Phlegmasia Cerulea Dolens (Painful Blue Leg) – Massive iliofemoral vein occlusion results in swelling of the entire leg, with extensive vascular congestion producing a painful cyanotic extremity – Prompt consultation with a vascular surgeon should be obtained because patients with phlegmasia cerulea dolens may require emergent thrombectomy. – If timely consultation is not possible, early thrombolytic therapy may be a limbsalvaging procedure in the absence of contraindications: – infuse alteplase via an infusion catheter placed into the thrombus. – transfer to an interventional radiology–capable center


Upper Extremity Venous Thromboses Upper extremity DVT can cause PE, and all patients with DVT above the elbow require definitive treatment – In the absence of pain or infection, catheter-associated DVT does not automatically warrant catheter removal if the catheter serves a current and vital purpose. – these patients should receive anticoagulation absent contraindications(at least 3 months) – Optimal treatment of isolated brachial vein thrombosis, often the result of a recent intravenous infusion (so-called infusion phlebitis) also remains uncertain, – the same management plan as described for superficial thrombophlebitis of the leg


Disposition – most patients with acute DVT can be discharged from the ED – Protocols that use monotherapy such as apixaban or rivaroxaban can facilitate this process. – selecting patients for home therapy using the modified Hestia criteria

- Slides: 27