De Quervain Tenosynovitis Presented by Dr Ahmed Samir

De Quervain Tenosynovitis ﺑﺴﻢ ﺍﻟﻠﻪ ﺍﻟﺮﺣﻤﻦ ﺍﻟﺮﺣﻴﻢ Presented by : Dr. Ahmed Samir Mohamed Lecturer of orthopaedic physical therapy

De Quervain Tenosynovitis

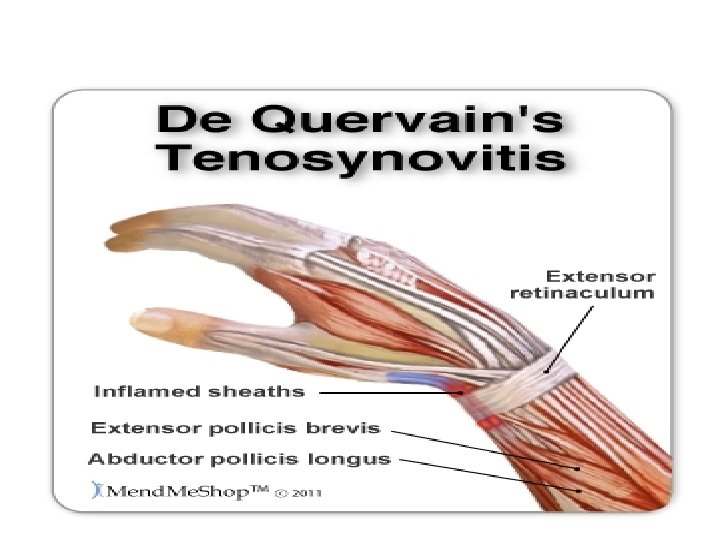
Pathological anatomy • The tendons of the abductor pollicis longus and the extensor pollicis brevis pass through the first dorsal compartment. • These muscles forming the lateral boundary of the anatomical snuff box. • These tendons are tightly secured against the radial Styloid by the overlying extensor retinaculum

Extensor Retinaculum And The Extensor Synovial Sheath

• Any thickening of the tendons from acute or repetitive trauma restrains gliding of the tendons through the sheath over the radial styloid process. • Efforts at thumb motion, especially when combined with ulnar deviation of the wrist, cause pain and perpetuate the inflammation and swelling, and lead to de Quervain tenosynovitis.

Clinically • Pain resulting from thumb and wrist motion. • tenderness and thickening at the radial styloid • Edema due to inflammation • Visible padded skin in this area

Visible padded skin

• Decreased thumb extension and radial deviation strength, secondary to pain and edema. • Decreased range of motion, secondary to pain, edema, and possible weakness. • Crepitation is rarely noted.

• Patients frequently are mothers of infants, and symptoms are often noted in both wrists. • Repetitive lifting of the baby as it grows heavier is responsible for friction tendinitis. • Day care workers and other persons who repetitively lift infants are frequently affected as well.

positive Finkelstein test

Finkelstein Test Finkelstein’s test is the classic provocative test for diagnosis of De Quervain’s disease. Action of the muscles involved in this disease: Extensor Pollicis Brevis (EPB) • Radial abduction of wrist (0 -25°) • Thumb extension (90°) Abductor Pollicis Longus (APL) • Wrist radial abduction (0 - 25°) • Thumb abduction (70°- 80°)

Finkelstein Test Patient position: Sitting or standing. Technique: To begin, the patient must sit comfortable and relaxed on the examination table. Next, examine the patients hand in the air, while the other hand rests just beside the body. The therapist then asks the patient to make a fist around a thumb and to perform a ulnar deviation. The test is positive if the patient complains of pain over the 1 st extensor compartment of the wrist.

Treatment Activity modification: 1 st of all, advice the patient to stop any activities that increase the symptoms (activities with ulnar deviation of the wrist or activities with the thumb if adducted and flexed).

Splints: Thumb splinting • The patient will usually be prescribed a splint for thumb immobilization

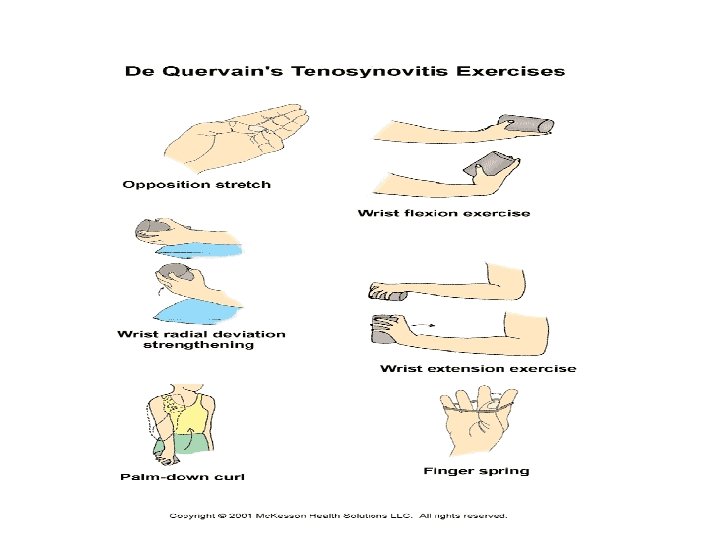
Physiotherapy modalities • Ice application to reduce pain and inflammation. • Phonopheresis or ultrasonic or Iontophoresis. • Electrical stimulation (TENS). • Gentle stretching ex: Gentle stretching in the pain free range for extensor pollicis muscle and abductor pollicis.

Once pain reduced • Deep friction massages just distal to the radial styloid process. • Gradual strength ex for the 1 st extensor compartement of the hand. • Strength for hand grip.

Trigger Finger

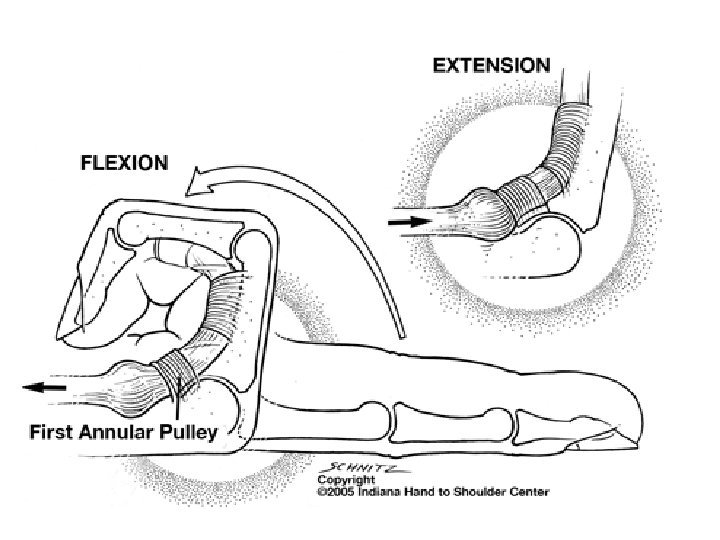
Normal anatomy: § Each digit of the hand has the ability to move freely throughout a full ROM into flexion and extension. § The efficiency, fluidity, and forcefulness of such movement is made possible by several "pulleys" along each digit of the hand. § These pulley systems are comprised of a series of retinacular-type structures that are either annular or cruciform in nature

Normal anatomy of the synovial sheath of the hand flexors

Trigger Finger • Trigger finger, or stenosing tenosynovitis, is caused by inflammation of the synovial sheath of flexor tendon of the finger, this lead to swelling of the affected finger and “triggering” of the finger and nodule formation. • Once nodule formed it becomes like a ball that pass though the annular ligament which act as a valve.

Clinically: • Pain and tenderness in the affected finger. • Finger stiffness. • Popping or clicking when you move your finger • tenderness or pain in the affected knuckle • the affected finger catching or locking in a bent position.

special Tests: • Open and Close hand check of pain, clicking and Loss of motion, particularly in extension

Stages of Stenosing Tenosynovitis: 1 = Normal 2 = A painful nodule 3 = Triggering 4 = The proximal interphalangeal (PIP) joint locks into flexion and is unlocked with active PIP joint extension 5 = The PIP joint locks and is unlocked with passive PIP joint extension 6 = The PIP joint remains locked in a flexed position

Physical therapy intervention: • Splint:

Ice application TENS Phonophoresis Laser therapy Massage Stretching exercises.

Tendon gliding Exercises Active and active assisted movement Strengthening Exercises Strengthening exercises for the wrist, elbow and shoulder muscles

Ref: • http: //www. physio-pedia. com • Apleyʼs system of orthopaedic and fracture. 9 th edition, 2010 • Clinical Orthopaedic Rehabilitation. 2 nd Edition, 2003.

Thank you

Thank you
- Slides: 32