Day 3 Preventing mistakes errors and making corrections


























- Slides: 29
Day 3: Preventing mistakes, errors and making corrections – Implementing CAPA 11/22/2020 1
Introduction Medication errors responsible for numerous adverse outcomes, including death This results in high cost (emotional and financial)
General framework for handling dispensing errors 11/22/2020 3
NCCMERP Index for Categorizing Medication Errors. 10 Reprinted with permission. Copyright © 2001, National Coordinating Council for Medication Error Reporting and Prevention. All rights reserved. EVALUATION AND GRADING OF SEVERITY
At which stage do Errors Occur? Prescribing Transcribing Dispensing Administering INVESTIGATION AND STAGING 39% 11% 12% 38%
Prescribing errors causes and factors There is an increasing body of knowledge ◦ ◦ ◦ New therapeutic entities Drug interactions Allergies database Food-drug interactions Post-marketing data Insufficient training in clinical pharmacology and therapeutics Inadequate internship and mentoring into effective prescribing Know it all attitude Overwork, inadequate time for refection and good decision-making Distractions
Summary on causes of prescribing errors 11/22/2020 7
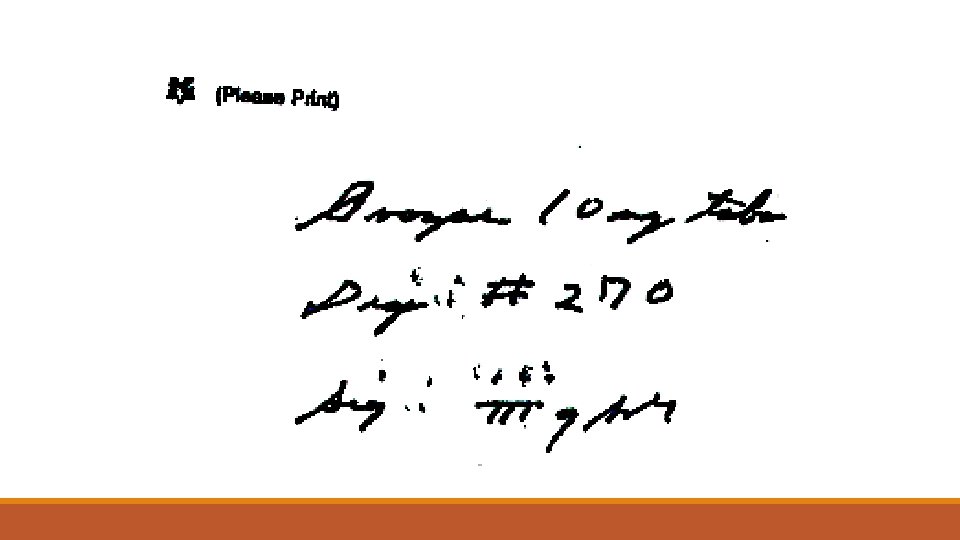
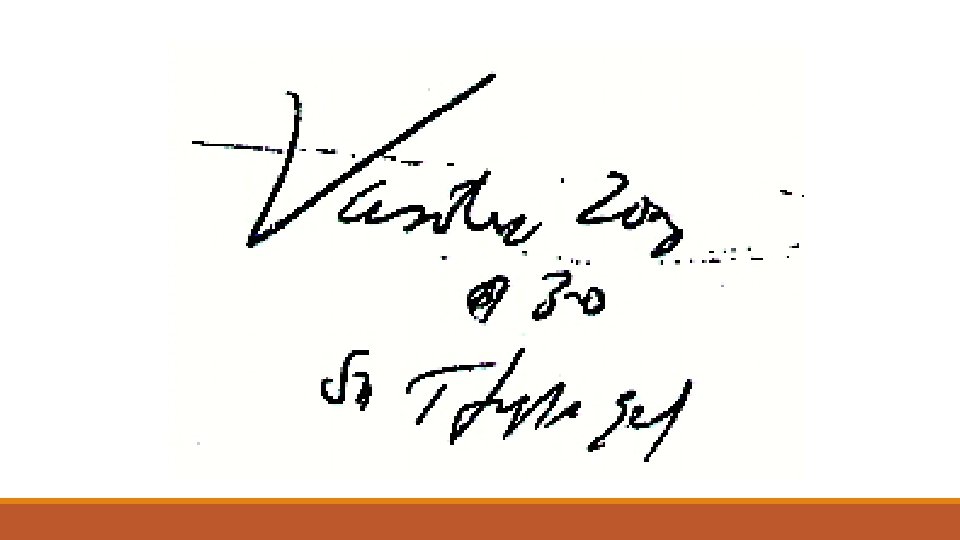
Written Medication Orders: Illegible Handwriting 16% of physicians have illegible handwriting Common cause of prescribing/dispensing errors Delays medication administration Interrupts workflow
Cohen MR. Medication Errors. Causes, Prevention, and Risk Management; 8. 1 -8. 23.
THE ABBREVIATION PROBLEM U ug q. d. qod SC TIW
Written Medication Orders: Do Not Use Abbreviations Drug names “QD” or “OD” for the word daily Letter “U” for unit “µg” for microgram (use mcg) “QOD” for every other day “sc” or “sq” for subcutaneous “a/” or “&” for and “cc” for cubic centimeter Cohen MR. Medication Errors. Causes, Prevention, and Risk Management; 8. 1 -8. 23. “D/C” discontinue discharge Jonesfor EH. Clev Clin J Med 1997; 64: or 355 -9.
Dosage problem
Unit problem
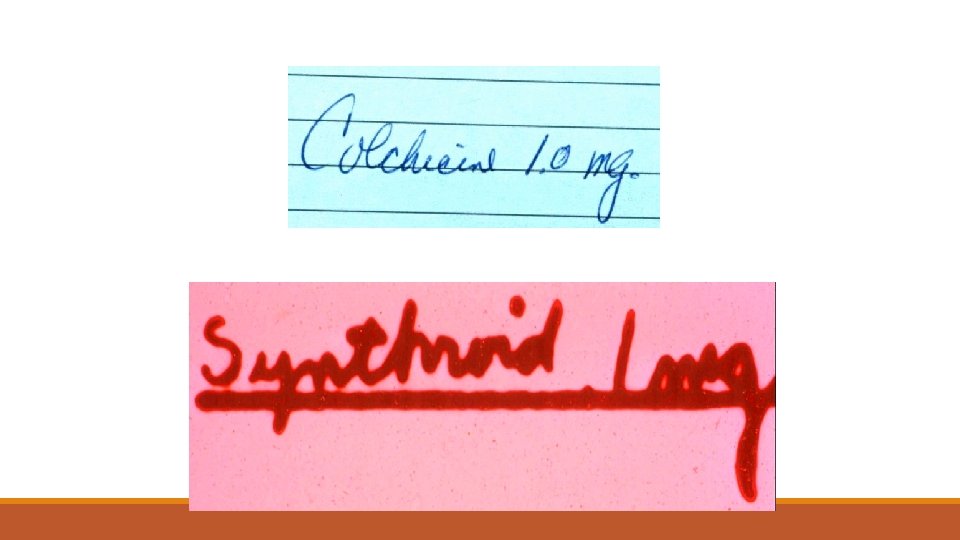
Written Medication Orders: Decimals Avoid whenever possible ◦ Use 500 mg for 0. 5 g ◦ Use 125 mcg for 0. 125 mg Never leave a decimal point “naked” ◦ Haldol. 5 mg Haldol 0. 5 mg Never use a terminal zero ◦ -Colchicine 1 mg not 1. 0 mg Space between name and dose ◦ Inderal 40 mg
Written Medication Orders: Drug Names “Look-Alike” or “Sound-Alike” Drug Names “Confirmation Bias” Addition of Suffixes ◦ Example Adalat CC 30 mg vs. Adalat 30 mg Cohen MR. Medication Errors. Causes, Prevention, and Risk Management; 8. 1 -8. 23. Cohen MR. Am Pharm 1992; NS 32: 21 -2.
Look-alike And Sound-alike Drug Names Accupril® Accutane® Alprazolam Lorazepam Cardene® Cardura® Flomax® Fosamax® Lamisil® Lomotil® Nizoral® Neoral® Plendil® Prilosec® Zantac® Zyrtec®
Dispensing Incidents/ Errors • Dispensing errors, significant other errors, omissions, incidents, or other non-compliances, including complaints of a non-commercial nature arising both within and external to the pharmacy, may be the subject of investigation. • Pharmacists should therefore follow a risk management procedure, including appropriate record keeping. 11/22/2020 20
11/22/2020 21
11/22/2020 22
11/22/2020 23
Dispensing Errors: Common Causes Work environment ◦ Workload ◦ Distractions ◦ Cluttered, disorganized work areas ◦ Use of outdated or incorrect references
11/22/2020 25
11/22/2020 26
Dispensing Errors: The Numbers ØOne study reported a 98. 3% accuracy in dispensing medications; or 1. 7% inaccuracy rate. ØBased on the above figure, how many dispensing errors cannot you predict from your pharmacy? ØYou need to know how many prescriptions your pharmacy fills per day.
Most Prevalent Dispensing Errors 1. Dispensing incorrect medication, dosage strength, or dosage form 2. Dosage miscalculations 3. Failure to identify drug interactions or contraindications
Types of Dispensing Errors Commission versus omission Mistake versus slip Potential versus actual