Cutaneous Manifestations of Nutritional Deficiency States and Gastrointestinal



 � Seen mainly in Asia and Africa, vitamin A deficiency")

 � The word \"pellagra\" is derived from two")



 � autosomal recessive syndrome � pellagrinous skin")

 � is most commonly seen in association with a")










 � � � After intestinal bypass surgery for")

 � � � Behcet's disease is a symptom complex of oral")



 � Histopathology: � The perianal mucosal lesions and oral lesions")











 reflects a primary infection with hepatitis B virus, acquired")


 � � � this rare but clinically distinctive dermarosis was")


- Slides: 58
Cutaneous Manifestations of Nutritional Deficiency States and Gastrointestinal Disease JAN 2015 F. Fadaei_Resident of Dermatology Kerman Medical University Of Science
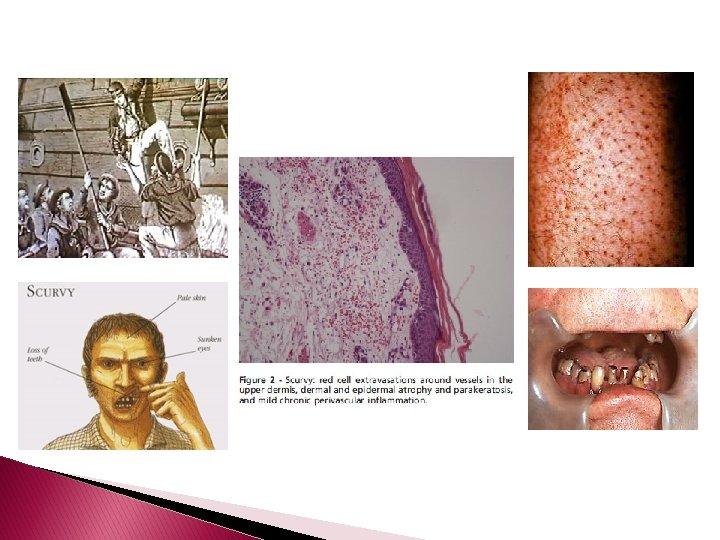
DEFICIENCIES OF VITAMINS, OTHER AMINO ACIDS, AND MINERALS scurvy � � � is due to vitamin C (ascorbic acid) deficiency. which is characterized by follicular purpuric macules with or without follicular hyperkeratosis and corkscrew hairs ecchymoses, particularly in the pretibial areas, and conjunctival and gingival hemorrhages, the latter associated with gingival hyperplasia. Subcutaneous hemorrhage with woody edema of the lower extremities and hemarthrosis may occur. Nonspecific aches and pains and impaired wound healing are frequent. Anemia, possibly related to decreased amounts of active folate and blood loss, is present in approximately 75% of individuals.
Histopathology � Follicular hyperkeratosis and perifollicular erythrocyte extravasation without an accompanying vasculopathy are characteristic. � Extensive extravasations are usually associated with deposits of hemosiderin within and outside of macrophages. � Most manifestations of scurvy can be attributed to defective collagen synthesis.
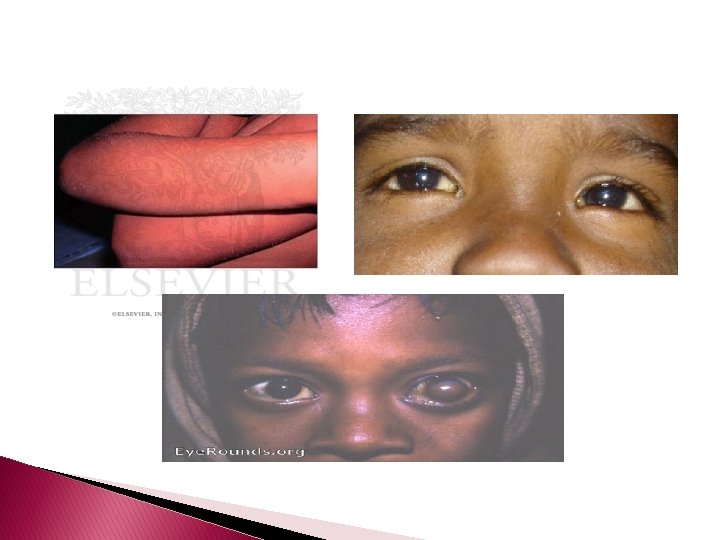
Vitamin A Deficiency (Phrynoderma) � Seen mainly in Asia and Africa, vitamin A deficiency is rare in the United States but may occur after intestinal bypass surgery for obesity or visceral myopathy. � Dryness and roughness of the skin along with conical follicular keratotic plugs characterize the cutaneous changes. � Night blindness, xerophthalmia, and keratomalacia also occur.
Histopathology � The skin shows moderate hyperkeratosis with distension of the upper part of the follicle by large, horny plugs. � Sebaceous glands are greatly reduced in size and may exhibit epithelial atrophy. � In severe cases both eccrine and sebaceous glands may exhibit squamous metaplasia.
Acquired Vitamin B 3 Deficiency (Pellagra) � The word "pellagra" is derived from two Italian words, "pelle, “ meaning "skin, " and "agra, " meaning "sharp burning" or "rough. " Although primarily ascribed to niacin (vitamin B 3) deficiency, other vitamin deficiencies or protein malnutrition appear integral to the development of the pellagra symptom complex. � Presenting as cutaneous lesions, gastrointestinal symptoms, and mental changes, pellagra has been ascribed the acronym of the three Os: dermatitis, diarrhea, and dementia.
� chronic alcoholics � anorexia nervosa, � malignant gastrointestinal tumors � intestinal parasitosis � Carcinoid syndrome � Pellagra has also been reported in patients receiving isoniazid, pyrazinamide, ethionamide, azathioprine, chloramphenicol, and anticonvulsants
Three basic skin eruptions occur in pellagrins � The first is a photo-induced eruption that is intensely erythematous and subsequently exfoliates to yield a hyperpigmented residuum. � � The second eruption comprises painful erythematous erosions in genital and perineal areas possibly induced by pressure, heat, and trauma. The increased skin fragility may reflect aberrations in the collagen and elastic fiber content of the skin. Pellagrins may develop a seborrheic dermatitis-like rash involving the face, scalp, and neck. Oral manifestations include beefy, red, cracked lips and a fissured or smooth, red, sore tongue.
Histopathology � � Psoriasiform epidermal hyperplasia with hyperkeratosis, parakeratosis, and a lymphocytic perivascular inflammatory cell infiltrate characterize initial lesions. Additional features include scattered necrotic keratinocytes, granular cell layer loss, and architectural disarray with dysmaturation of the epidermis. Depigmentation of the basal layer with accumulation of fat droplets is described, as is vacuolation of cells within the granular and spinous layers. Epidermal atrophy, hypermelanosis, vascular ectasia, and sebaceous atrophy characterize end-stage lesions. � Seborrheic dermatitis-like lesions may show sebaceous gland hyperplasia with follicular dilation. � Fragmentation, swelling, and thickening of elastic fibers, swelling of collagen fibers, and merging of elastic tissue with collagen have been described.
Congenital Vitamin B 3 Deficiency (Hartnup's Disease) � autosomal recessive syndrome � pellagrinous skin , neurologic abnormalities including mental deterioration and cerebellar ataxia, and abnormal aminoaciduria � The intermittent skin eruption is seen primarily in the summer at times of maximal sun exposure and at times resembles either poikiloderma vasculare atrophicans or, when vesicles are prominent, hydroa vacciniforme. � Hartnup's disease, in contrast to pellagra, does not respond to treatment with niacin.
Histopathology � The histopathology usually resembles that of pellagra. � Poikilodermatous lesions manifest flattening of the epidermis and ptominent dermal melanophage accumulation.
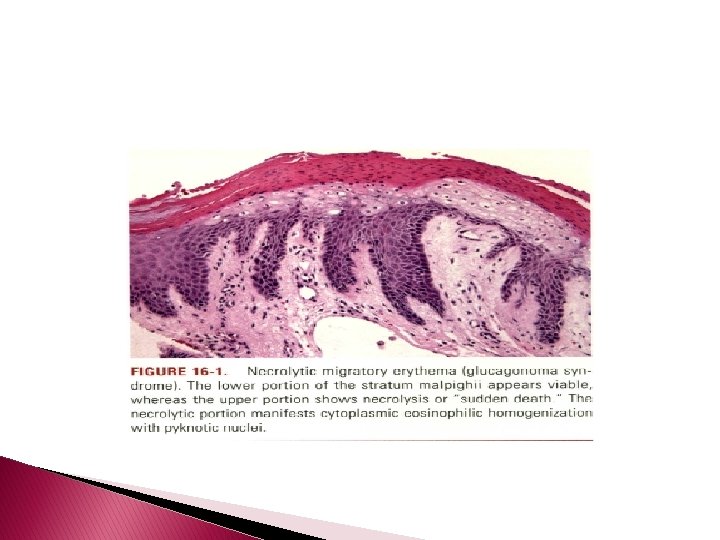
Necrolytic Migratory Erythema (Glucagonoma Syndrome) � is most commonly seen in association with a glucagonsecreting alpha cell tumor of the pancreas. � Surgical extirpation of the neoplasm may result in resolution of the eruption, as may amino acid and fatty acid infusion.
� The manifestations of glucagonoma syndrome include cutaneous and mucosal lesions, weight loss, anemia, adultonset diabetes, glucose intolerance, elevation of serum glucagon levels, and thromboembolism. Skin lesions are seen mainly on the face in perioral and perinasal distribution, the perineum, genitals, shins, ankles, and feet and include erythema, erosions, and flaccid vesicularpustular lesions that rupture easily and often have a circinate appearance due to peripheral spreading. � Rapid healing and the continuous development of new lesions result in daily fluctuations of the eruption.
Histopathology � � � The characteristic acute lesion shows abrupt necrosis of the upper layers of the stratum spinosum, which may detach from the subjacent viable epidermis. Keratinocyte degeneration varies from marked hydropic swelling to cytoplasmic eosinophilia and nuclear pyknosis. Neutrophilic chemotaxis to the necrotic epithelium may eventuate in a subcorneal pustule. Chronic lesions have as their hallmark a psoriasiform dermatitis. In both acute and chronic lesions there is architectural disarray, reflecting a maturation defect; it manifests as basal layer hyperplasia, vacuolar change, and a deficient granular layer. The epidermis is surmounted by a broad parakeratotic scale.
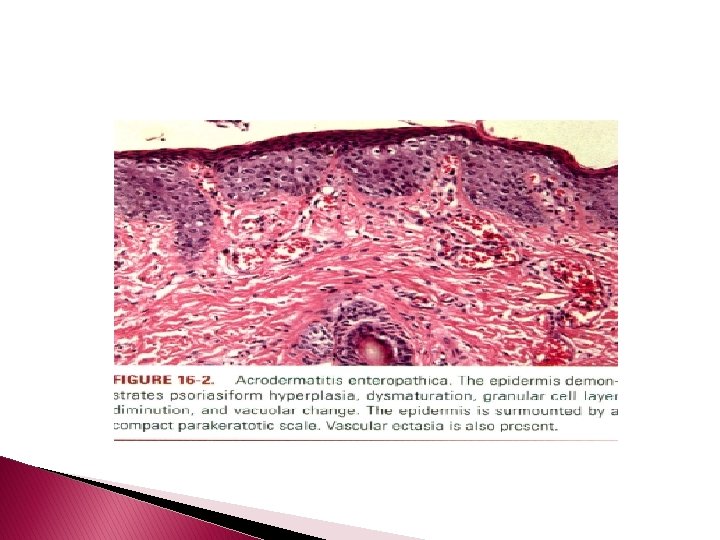
Acrodermatitis Enteropathica � � zinc Caused by defective intestinal absorption of , it usually manifests in the first 4 to 10 weeks of life in bottle-fed infants as an acral and periorificial eruption with intractable diarrhea and diffuse partial alopecia. The skin exhibits areas of moist erythema, occasionally associated with vesiculobullous and/or pustular lesions. Untreated cases eventuate in death from malnutrition and infection because of immunologic defects reflecting zinc deficiency, the latter including decreased natural killer cell activity, impaired delayed-type hypersensitivity, and thymic atrophy. Paronychia, stomatitis, photophobia, blepharitis, conjunctivitis, corneal opacities, and hoarseness are additional manifestations. An acquired form occurs in patients receiving intravenous hyperalimentation with low zinc content , in infants who are fed breast milk low in zinc , in patients with Crohn's disease, in patients with ornithine transcarbamylase deficiency , in patients with status post pancreaticouodenectomy , and in the setting of AIDS nephropathy when proteinuria eventuates in excessive loss of protein-bound zinc.
Histopathology � The upper part of the epidermis shows pallor due to intracellular edema and is surmounted by a confluent, thick, parakeratotic scale that may contain neutrophils. � There is granular cell layer diminution and focal dyskeratosis. � As with necrolytic migratory erythema, there may be architectural disarray and dismaturation. Subcorneal vesicles may be present. � The epidermis manifests variable psoriasiform hyperplasia and atrophy and, in a few instances, acantholysis.
Kwashiorkor � � � Kwashiorkor is a form of protein malnutrition coupled to carbohydrate excess resulting in reduction of a patient's weight by 20% to 40%. Primary manifestations include generalized hypopigmentation that begins circumorally and in the pretibial regions. With disease progression, hyperpigmented plaques with a waxy texture develop over the elbows and ankles and in the intertriginous areas. Dryness, desquamation, and decreased skin elasticity occur. “ Crazy pavement" or "Aaky-paint dermatosis“ describes the extensive desquamation with erosions and fissuring, vesicles, and bullae that may be seen in severe cases. Prominent edema can mask the underlying muscle and subcutaneous tissue atrophy. Hair abnormalities include a diffuse alopecia, alternating bands of normal and hypo pigmented hair referred to as the "flag" sign, and an unusual reddish-brown discoloration called hypochromotrichia. Extracutaneous manifestations include cerebral atrophy secondary to loss of myelin lipid , diarrhea, hepatic steatosis, and mucosal abnormalities such as a smooth tongue, angular stomatitis, and perianal and nasal erosions.
Histopathology � The histologic picture of skin lesions is not diagnostic but is said to resemble that of pellagra. � The changes include psoriasiform hyperplasia with hyperkeratosis and increased pigmentation throughout the epidermis or atrophy with irregular shortening and flattening of the rete.
CUTANEOUS MANIFESTATIONS OF GASTROINTESTINAL DISEASE
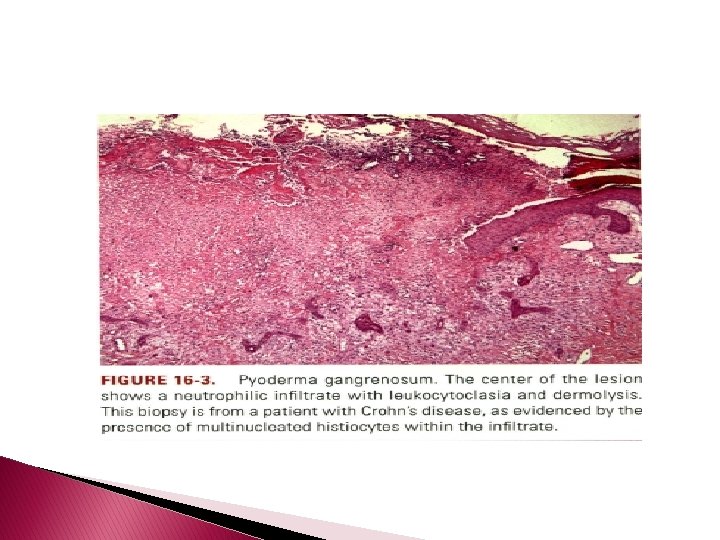
Pyoderma Gangrenosum � � � Beginning as folliculocentric pustules or fluctuant nodules, the lesions ulcerate and have sharply circumscribed violaceous, raised edges in which necrotic pustules may be seen. The disease most commonly occurs on the lower extremities and trunk in adults who are 30 to 50 years old. Occasionally it occurs in childhood, affecting the buttocks, perineal region, and head and neck area. Koebnerization occurs at sites of trauma, including intravenous puncture sites, surgical wounds, and peristomal sites. Roughly 70% of cases are associated with inflammatory bowel disease, hematologic disorders including acute lymphoid and myeloid leukemias and myeloma, rheumatologic conditions including RA & LE, and hepatopathies , including chronic active hepatitis, primary biliary cirrhosis, & sclerosing cholangitis
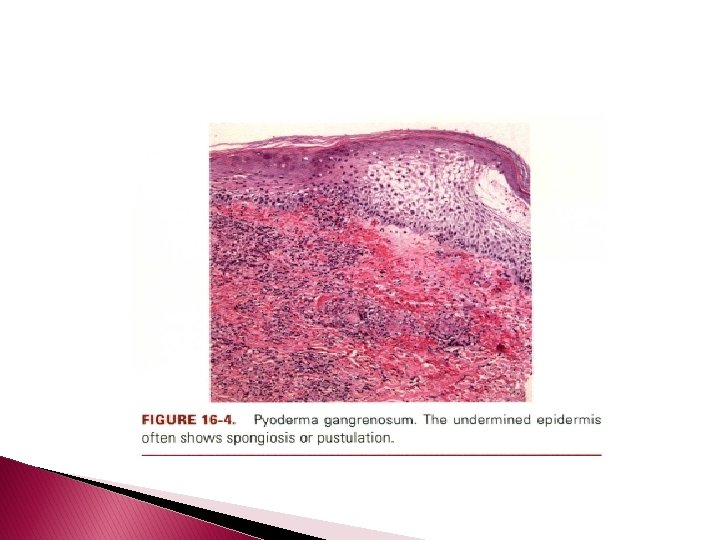
Histopathology � � � Pyoderma gangrenosum exhibits a dichotomous tissue reaction, showing central necrotizing suppurative inflammation, usually with ulceration, and a peripherallymphocyric vascular reaction comprising perivascular and intramural lymphocytic infiltrates, usually without fibrin deposition or mural necrosis. Transitional areas show neutrophils in a loose cuff around the angiocentric lymphocytic infiltrates, defining a mixed lymphocytic and neutrophilic vascular reaction termed a Sweets-like vascular reaction. Bullous lesions may also demonstrate a Sweet's-like vascular reaction with perivascular disintegrating neutrophilic infiltrates and hemorrhage without mural necrosis or luminal fibrin deposition. At variance with Sweet's syndrome is destruction of the connective tissue framework with resultant tissue pathergy. Although a leukocytoclastic vasculitis may be observed in areas of maximal tissue pathology, pyoderma gangrenosum does not reflect a primary vasculitis.
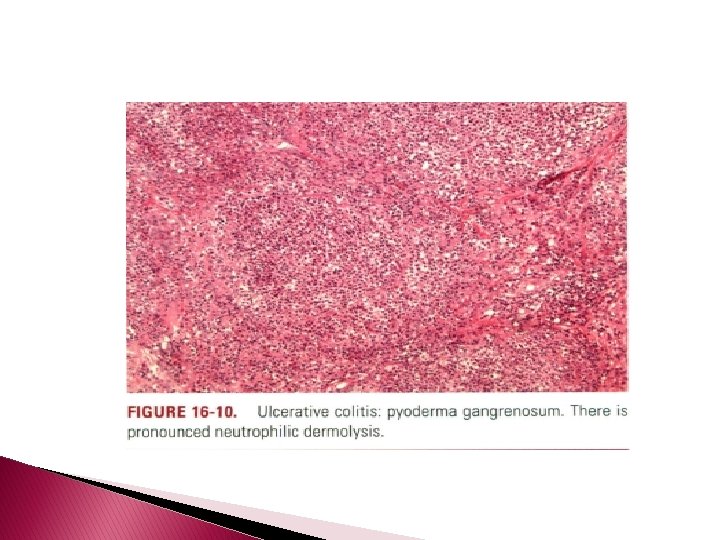
� In some cases a necrotizing pustular follicular reaction may be the central nidus of the lesion, particularly in the vesicular pustular variant associated with ulcerative colitis or shows a neutrophilic infiltrate with leukocytoclasia and dermolysis. � In the superficial granulomatous variant, florid pseudoepitheliomatous hyperplasia may be observed along with the intraepithelial and superficial dermal suppurative granulomatous inflammation with admixed plasma cells and eosinophils. � Cases of pyoderma gangrenosum associated with Crohn's disease may have areas of granulomatous inflammation.
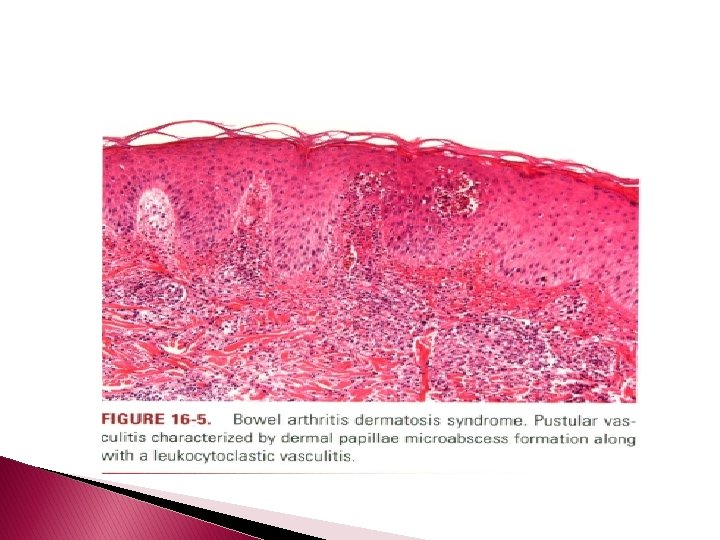
Bowel-Associated Dermatosis-Arthritis Syndrome (Bowel Bypass Syndrome) � � � After intestinal bypass surgery for morbid obesity or after extensive small bowel resection, some patients develop an intermittent eruption, mainly on the extremities, comprising purpuric macules and papules that may evolve into necrotizing vesiculopustular lesions. Polyarthritis, malaise, and fever are often associated with and may precede the eruption. Although originally called the bowel bypass syndrome, it now bears the more appropriate appellation bowel arthritis dermatosis syndrome because a similar picture may develop in patients with diverticulosis, peptic ulcer disease, and idiopathic inflammatory bowel disease
Histopathology � Characteristically, there is a perivascular Lymphocytic infiltrate with a peripheral cuff of disintegrating neutrophils, erythrocyte extravasation, & absent or minimal fibrin deposition consistent with a Sweet'slike vascular reaction; leukocytoclastic vasculitis occurs less often. � Papillary dermal edema may be striking and may lead to subepidermal vesiculation. � Epidermal pustulation, variable epithelial necrosis, & massive superficial dermal neutrophilia complete the picture & define pustular vasculitis.
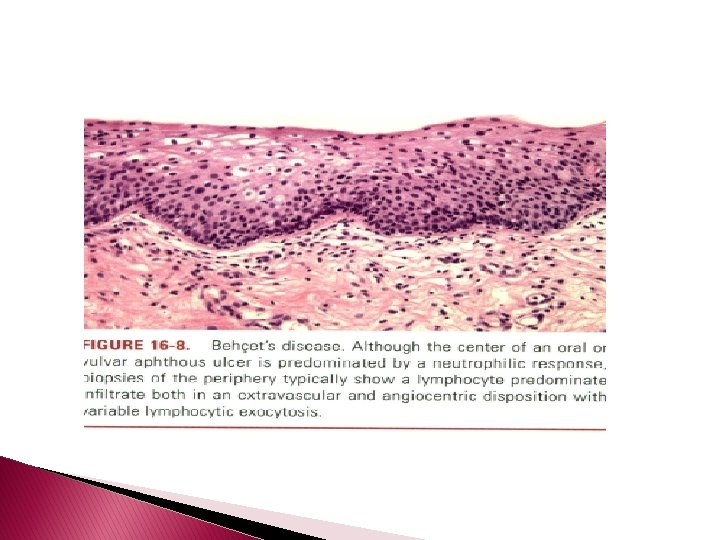
Aphthosis (Behc~et's Disease) � � � Behcet's disease is a symptom complex of oral and genital ulceration and iritis that has a worldwide distribution but is most common in the Pacific rim and eastern Mediterranean. The presence of oral ulceration plus any two signs of genital ulceration, skin lesions (e. g. , pustules or nodules), or eye lesions (e. g. , uveitis or retinal vasculitis) is diagnostic. The cutaneous lesions include erythema nodosum-like nodules, vesicles, pustules, pyoderma gangrenosum, Sweet's syndrome, a pustular reaction to needle trauma, superficial migratory thrombophlebitis, ulceration, infiltrative erythema, acral purpuric papulonodular lesions, and acneiform folliculitis.
� � � The extracutaneous manifestations are categorized as oral and/or genital aphthae; vasculo-, ocular-, entero-, or neuro- Behcet's disease; renal disease; and arthritis. Oral apthosis recurring at least three times over a 12 -month period is essential to the diagnosis. In vasculo-Behcet's disease, aneurysms & occlusive venous & arterial main vessel lesions occur. The ocular manifestations include uveitis, hypopyon iritis, optic neuritis, and choroiditis. Entero-Behcet'sdisease manifests as diarrhea, constipation, abdominal pain, vomiting, and melena. Neuro-Behcet's disease presents as brainstem dysfunction, meningoencephalitis, organic psychiatric symptoms, and mononeuritis multiplex. Asymptomatic microhematuria and/or proteinuria are among the renal manifestations. An oligoarthritis may involve the wrist, elbow, knee, or ankle joints. Morbidity and mortality in one large series of Turkish patients were greatest in young males; both the onset and the severity of ocular disease were greatest early in the course of disease, suggesting that the "disease burden" in Behcet'sdisease is greatest early and that it tends to "burn out“ over time. However, neurologic and major vessel disease can occur at any time and can have late onset 5 to 10 years into the course of illness.
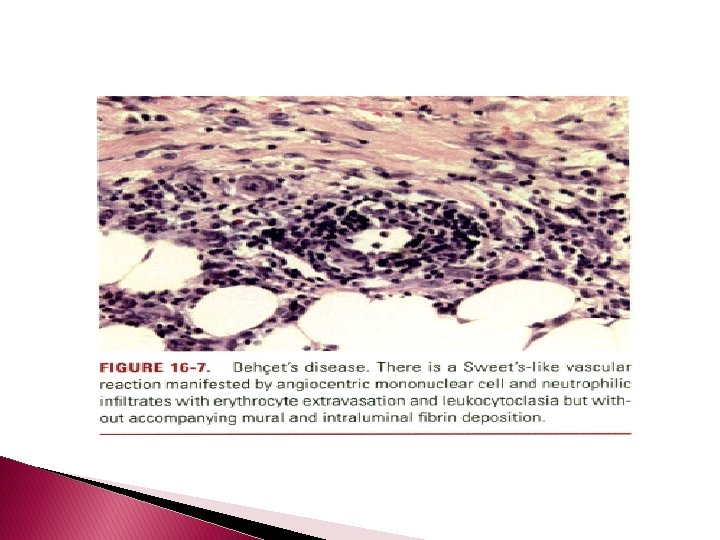
Histopathology � � � The cutaneous lesions can be categorized histopathologically into two main groups: vascular and extravascular with or without vasculopathy including acneiform. The pathologic spectrum of the cutaneous vasculopathy encompasses a mononuclear cell vasculitis with variable mural and luminal fibrin deposition; a paucicellular thrombogenic vasculopathy; and a neutrophilic vascular reaction involving capillaries and veins of all calibers. The mononuclear cell reaction may be frankly granulomatous or it may be lymphocytic predominant to define a lymphocytic vasculitis. The neutrophilic vascular reaction may resemble that of Sweet's syndrome or a leukocytoclastic vasculitis. Diffuse extravascular mononuclear cell- and/or neutrophil predominant
� inflammation of the dermis and/or panniculus may occur with or without the afore mentioned vascular changes. � The histiocytes infiltrating the panniculus may manifest phagocytosis of cellular debris. � Suppurative or mixed suppurative and granulomatous folliculitis with or without vasculitis characterizes the acneiform lesions. � Acral purpuric papulonodular lesions show a lymphocytic interface dermatitis with lymphocytic exocytosis, dyskeratosis, and a perivascular lymphocytic infiltrate, recapitulating the mucosal histopathology.
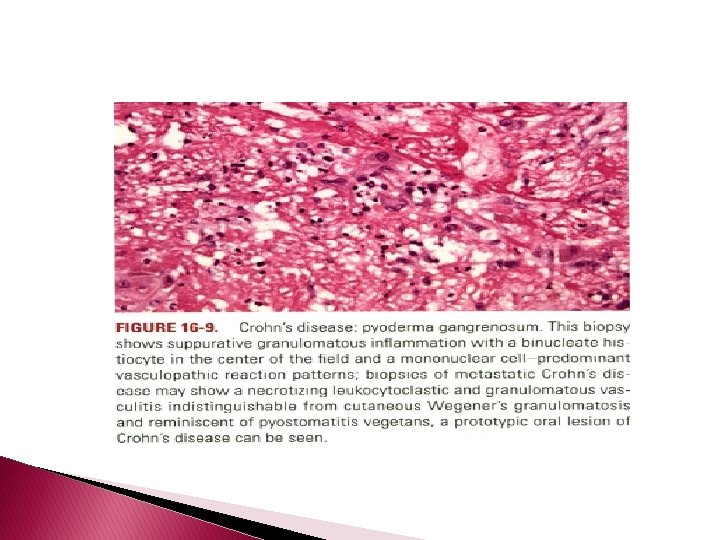
Crohn's Disease (Regional Enteritis) � Histopathology: � The perianal mucosal lesions and oral lesions of pyostomatitis vegetans show pseudoepitheliomatous hyperplasia in conjunction with suppurative granulomatous inflammation within the epithelium and subjacent corium. � The most frequent histologic patterns seen in metastatic Crohn's disease are nonsuppurative granulomata, which may assume a sarcoidal or diff. Use pattern, the latter often in close apposition to the epidermis in the fashion of a lichenoid and granulomatous dermatitis &granulomatous vasculitis.
� Histologic examination of the erythema nodosum-like lesion may show one of 4 patterns: � (a) septal panniculitis consistent with classic erythema nodosum, � (b) dermal-based sarcoidal granulomata � (c) a dermal-based small-vessel granulomatous or leukocytoclastic vasculitis, � (d) benign cutaneous polyarteritis nodosa. � The latter shows mural infiltration by histiocytes and neutrophils with variable mural fibrinoid necrosis confined to the muscular arteries of the subcutaneous fat
�A pauci-inflammatory thrombogenic vasculopathy characterizes the cutaneous infarcts associated with lupus anticoagulant. � Necrobiosis lipoidica-like or granuloma annulare -like foci may also be seen defined by areas of collagen necrobiosis with concomitant mucin or fibrin deposition and a palisading histiocytic infiltrate. Unlike idiopathic granuloma annulare or necrobiosis lipoidica, there usually is an accompanying leukocyroclastic vasculitis, thrombogenic or granulomatous vasculopathy, and foci of extravascular neutrophilia. �
� Dense neutrophilic infiltration of the dermis accompanied by scattered giant cells has been reported. � We have also seen this pattern of suppurative granulomatous inflammation in concert with the afore mentioned necrobiosis lipoidica or granuloma annulare tissue reaction. � Cases of lip swelling show non necrotizing granulomatous inflammation � The histology of pyoderma gangrenosum has been previously discussed. A suppurative panniculitis may also be seen
Ulcerative Colitis � Ulcerative colitis is an idiopathic inflammatory bowel disease involving the large intestine, with rectal involvement being almost ubiquitous. � It is characterized by glandular destruction and inflammation of variable intensity. Glandular dysplasia eventuating in carcinoma complicates the clinical course, particularly in patients with disease of pediatric onset.
Histopathology � The histology of pyoderma gangrenosum and erythema nodosum is discussed elsewhere. � Cutaneous vasculitis in association with ulcerative colitis includes Ig. A-associated leukocytoclastic vasculitis and benign cutaneous polyarteritis nodosa. �A pauci-inflammatory thrombogenic vasculopathy involving vessels throughout the dermis and subcutis characterizes the histomorphology of associated lupus anticoagulant and/or cryofibrinogenemia.
Celiac Disease � Celiac disease is a malabsorption syndrome with a prevalence of up to 1% of the adult population of Western countries and is associated with HLA-DQ 2 (DQAl */DQBl *2) in greater than 90% of celiac disease patients. � It reflects small-intestinal mucosal injury caused by a humoral immune response to ingested gluten and is associated with dermatitis herpetiformis in roughly 25% of cases.
�A leukocytoclastic vasculitis has also been described in patients with celiac disease. � The presence of Ig. A or Ig. G anti-tissue transglutaminase and antiendomysial antibodies is seen in 80% to 90% of patients with active gut mucosal inflammation and has a high specificity for the diagnosis.
Sclerosing Cholangitis and Primary Biliary Cirrhosis � Pyoderma gangrenosum, particularly a disseminated superficial vesiculopustular variant , and dermatitis herpetiform is have been described in association with sclerosing cholangitis � In addition, diffuse superficial pyoderma gangrenosum has been described in patients with ulcerative colitis, an associated finding in 70% of patients with sclerosing cholangitis.
Histopathology � Vesiculopustular pyoderma gangrenosum is characterized by a necrolyric subepithelial blister in which massive papillary edema is accompanied by sheets of neutrophils within the blister cavity and prominent leukocytoclasia often centered around follicles. � Peripheral to the areas of neutrophilia, angiocentric mononuclear-cell infiltrates with minimal accompanying vascular injury are observed
Hepatitis � Hepatitis can be broadly categorized into infectious and noninfectious causes. � Most of the former are viral and are mediated by hepatitis A, B, C, and delta agent, cytomegalovirus, EBV, and, rarely, varicella, measles, and herpes simplex virus. � Chronic active hepatitis of autoimmune etiology is a necroinflammatory disorder of unknown etiology with a predilection for young women. � Both the clinical presentation and liver chemistry profile may resemble those of infectious hepatitis. � Hepatitis C antibodies have been demonstrated in patients with classic autoimmune hepatitis, a finding reputed to represent a nonspecific response that disappears during remission.
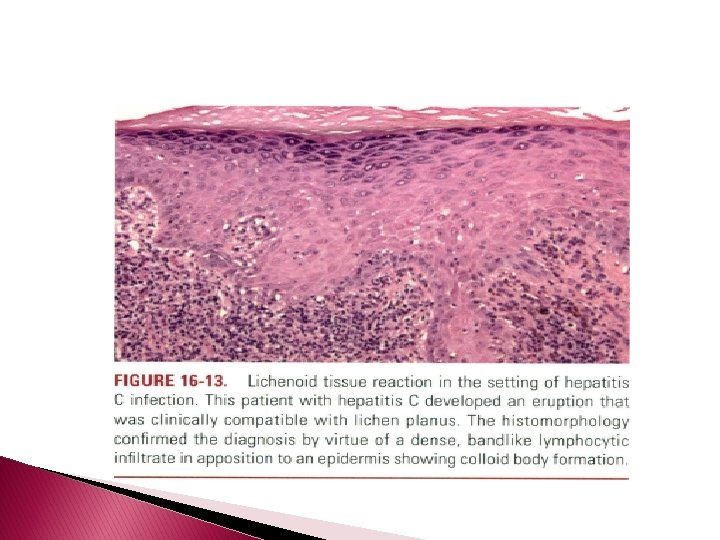
� The principal cutaneous manifestations of viral and autoimmune hepatitis are lichen planus, leukocytoclastic vasculitis, porphyria cutanea tarda , erythema multiforme, pyoderma gangrenosum , and Gianotti� Crosti syndrome.
� Papular acrodermatitis (Gianotti-Crosti syndrome) reflects a primary infection with hepatitis B virus, acquired through the skin or mucous membranes, and comprises a nonpruritic, erythematous, papular eruption on the face, extremities, and buttocks. � The eruption usually lasts about 3 weeks and is associated with lymphadenopathy and an acute, usually anicteric hepatitis of at least 2 months' duration that only rarely progresses to chronic liver disease.
Histopathology � The histologic appearance of the papules in Gianotti-Crosti syndrome includes a moderately dense infiltrate of lymphocytes and histiocytes in the upper and middermis that are found mainly around capillaries that exhibit endothelial swelling, accompanied by erythrocyte extravasation. � Focal spongiosis, parakeratosis with mild acanthosis, and a focal interface dermatitis complete the picture
� the skin lesions of hepatitis C can be classified by the dominant reaction pattern, the most common being vasculopathies of neutrophilic and lymphocytic vasculitis and pauci-inflammatory subtypes; palisading granulomatoun inflammation; sterile neutrophilic folliculitis; neutrophilic lobular panniculitis; benign cutaneous polyarteritis nodosa; neutrophilic dermatoses including neutrophilic urticaria and pyoderma gangrenosum; and interface dermatitis
Acrokeratosis Neoplastica (Bazex's Syndrome) � � � this rare but clinically distinctive dermarosis was originally associated with either a primary malignant neoplasm of the upper aerodigestive tract-most commonly squamous cell carcinoma-or metastatic cancer to the lymph nodes of the neck. Other associated malignancies have since been described, including poorly differentiated carcinoma, adenocarcinoma, and small-cell carcinoma among others. Greater than 90% of the patients are male, and most are older than 40 years of age. Thickening of the periungual and subungual skin and of the palms and soles occurs initially when the neoplasm is silent. Subsequently, the skin of the ears, nose, face, and trunk and extremities becomes involved and shows a violaceous color, peeling, and fissuring. The palmar lesions may resemble those of Reiter's disease.
Histopathology � Ill-defined perivascular lymphocytic infiltrates containing a few pyknotic neutrophils in the upper dermis along with mild acanthosis, hyperkeratosis, and scattered parakeratotic foci are described. � Eosinophilic and vacuolar degeneration of the spinous layer may be noted
Thanks for your attention