Current Standards for Treatment of DVT Rabih A

Current Standards for Treatment of DVT Rabih A. Chaer MD Assistant Professor of Surgery Division of Vascular Surgery University of Pittsburgh Medical Center

DISCLOSURES Rabih A. Chaer, MD I have no real or apparent conflicts of interest to report.

DISLOSURES • NONE

DVT / Chronic Venous Insufficiency • > 6 million people develop DVT annually • > 600, 000 episodes of pulmonary embolus annually • It is estimated that 5% of the Medicare population has or has had a venous stasis ulcer • The average cost to Medicare for treatment of venous stasis ulcers – $16, 000/month

l 1/3 of DVT leads to PE if patient not anticoagulated Mammen EF. CHEST 1992; 102: 640 S-644 S 50% mortality Hirsch, J et al. Venous thromboembolism, New York: Grune and Stratton 1981

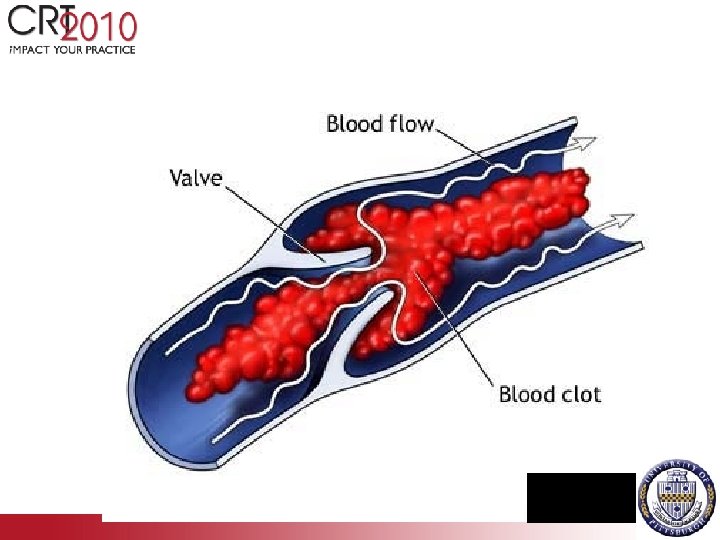
ILIOFEMORAL DVT • Phlegmasia alba dolens- pain, edema, blanching • Phlegmasia cerulea dolens- painful blue leg • <10% of patients with DVT

DEEP VEIN THROMBOSIS Proximal DVT- Not all the same – 95% of patients with iliofemoral DVT treated with anticoagulation alone have ambulatory venous hypertension at 5 yrs – 90% have CVI – 15% develop venous ulcers, 15% claudicate Lagerstedt et al. Lancet 1985 2: 515 -18 Akesson et al. Eur J Vasc Surg 1990 4: 43 -8

Varicosities / Post-thrombotic Syndrome

Venous Stasis Ulcer / Post-thrombotic Syndrome
 Advantages: • Reduces occurrence of")
Treatment Anticoagulation is Standard of Care (heparin, warfarin, LMWH) Advantages: • Reduces occurrence of a PE • Can decrease symptoms • Easy to administer LMWH Disadvantages: • Bleeding complications from long-term use of anticoagulants • Does not decrease thrombus burden • Has not been shown to reduce incidence of valve damage Abu. Rahma AF. Annals of Surgery 2001: 233(6): 752 -760.

Th Th ro m X X Prevent Extension X X + Reduce Recurrence X X + Restore Patency X X Preserve Valve Function X X N Reduce CVI + y om be bo gu oa An tic av C X o X Reduce PE ct la r Fi lte al x R ly tic tio n R x Acute DVT: Therapeutic Goals/Options

Thrombus Removal • Persistent proximal obstruction leads to distal valvular incompetence • Early spontaneous lysis preserves valve function • Thrombus removal in patients with acute iliofemoral DVT results in less postthrombotic morbidity Meissner et al. J Vasc Surg 1993; 18: 596 -605 Plate et al. Eur J Vasc Endovasc Surg 1997; 14: 367 -74

Thrombus Removal • Surgical removal • Catheter-directed thrombolytic therapy • Mechanical Thrombectomy Device
 Thrombolysis • • Activation of fibrin-bound plasminogen Accelerated lysis, less systemic")
Catheter- directed (intrathrombus) Thrombolysis • • Activation of fibrin-bound plasminogen Accelerated lysis, less systemic effect >85% success rate 5 -10% bleeding complications, mainly at puncture site • Intracranial bleeding rare- 3 patients in the national venous registry Mewissen et al. Radiology 1999; 211: 39 -49

Physiologic Outcomes • >60% thrombosis free survival at 1 year • Preservation of valve function with successful lysis: 72% of patients with complete lysis had normal valve function Mewissen et al. Radiology 1999; 211: 39 -49

Quality of Life Outcome • Catheter-directed urokinase for iliofemoral DVT vs anticoagulation alone. • Follow up at 16 and 22 months • Significantly better quality of life in the lysis group, especially in patients who had ≥ 50% lysis. Comerota AJ et al: Catheter-directed thrombolysis for iliofemoral deep venous thrombosis improves health-related quality of life. J Vasc Surg 2000; 32: 130 -137.

Pharmacomechanical Thrombolysis • 2008 ACCP Evidence Based Practice Guidelines 1 – “In selected patients with extensive acute proximal DVT (eg, iliofemoral DVT, symptoms for<14 days, good functional status, life expectancy of >1 year) who have a low risk of bleeding, we suggest that catheter-directed thrombolysis may be used to reduce acute symptoms and postthrombotic morbidity…” (Grade 2 B) – “We suggest pharmacomechanical thrombolysis…in preference to catheter directed thrombolysis alone to shorten treatment time if appropriate expertise and resources available. ” (Grade 2 C) 1 Executive Summary. Chest. 133(6), 2008.

Pharmaco. Mechanical Thrombolysis • Combines thrombolytic infusion with mechanical energy • Increases the surface area penetration of thrombolytics • Dissolves and macerates thrombus

Advantages of PMT • • • One session therapy Less lytic exposure Minimal or No ICU stay Less blood transfusion Shorter hospital stay Prompt clearance of essential outflow veins • Immediate symptom resolution

Pharmacomechanical Thrombectomy for Deep Venous Thrombosis: A Safe Alternative for High Risk Patients American Venous Forum Annual Meeting 2009 Division of Vascular Surgery University of Pittsburgh Medical Center Rao A, Chaer RA et al. J Vasc Surg. 2009 Nov; 50(5): 1092 -8.

Objectives • Pharmacomechanical thrombectomy in patients with contraindications to treatment – Chronic DVTs (>14 days) – Absolute/relative contraindications to lysis

Patients/Methods • Retrospective review of patients with symptomatic DVT treated between 2007 -2008 • Anticoagulation – Persistent severe symptoms • Treated with PMT – 1) Locally delivered lytic (t. PA) – 2) Angio. Jet (Possis Medical, Minneapolis, MN) or Trellis (Bacchus Vascular, Santa Clara, CA) systems • CDT used selectively (routine CDT vs EKOS) • Selective iliac PTA/stent • Selective caval interruption

PMT • • 43 patients: symptoms 13. 6± 9. 6 days 44%> 14 days, 35% high risk for bleeding 15 patients with thrombosed IVC filter 63% treated in one session, 16 required CDT for suboptimal PMT. • 35% iliac stenting • Successful >50% lysis and symptom resolution in 95%

FOLLOW UP • 100% limb salvage • No systemic bleed, 2 hematoma • 96% freedom from DVT recurrence and reintervention at 9 months

CONCLUSIONS • PMT effective and safe and can limit treatment to one session, even in some high risk patients • Effective in sub-acute DVT

CONCLUSIONS • PMT should be offered to candidate patients with symptomatic iliofemoral DVT • High risk patients should be considered but carefully selected and treated in one session • Further level I evidence is needed to determine the best treatment algorithm and the long term effect on PTS

ATTRACT TRIAL Acute Venous Thrombosis: Thrombus Removal With Adjunctive Catheter-Directed Thrombolysis • Randomized multicenter NIH sponsored trial • Outcomes: PTS, quality of life, relief of pain and swelling, safety and costs • 692 patients, 2 year follow up • 2 PMT groups

PITTSBURGH
- Slides: 29