Current Situation of Inflammatory Bowel Disease in Taiwan

Current Situation of Inflammatory Bowel Disease in Taiwan Disease and Treatment 1

Contents • Introduction of Inflammation Bowel Disease • Treatment Goals in IBD • The Biologics Application in IBD

Introduction of Inflammation Bowel Disease

Historical timelines of Crohn’s disease and Ulcerative Colitis throughout the world. Nature Reviews Gastroenterology & Hepatology 12, 720– 727 (2015)

The global prevalence of IBD on 2015 Nature Reviews Gastroenterology & Hepatology 12, 720– 727 (2015)

National health insurance database in Taiwan -- 1998 ~ 2010 -- UC CD Total 2357 558 Male 1434 384 Female 923 174 Age at diagnosis: UC vs. CD = 44. 7 vs. 37. 9 (p<0. 001) Male vs. Female = 46. 4 vs. 43. 7 in UC (p<0. 01) = 41. 1 vs. 36. 5 in CD (p=0. 01) Inflamm Bowel Dis 2013; 19: 2815
 Annual prevalence (/105) 5 8. 49 Series 1 Crohn’s disease")
Prevalence (per 10 inhabitants) Annual prevalence (/105) 5 8. 49 Series 1 Crohn’s disease 8. 0 Series 2 Ulcerative colitis 6. 0 4. 0 10. 7 x 2. 05 2. 0 0. 79 0. 0 10. 8 x 0. 19 98 99 00 01 02 03 04 05 06 07 08 09 10 Young age on set + low mortality rate = increasing prevalence Inflamm Bowel Dis 2013; 19: 2815

Annual incidence of IBD in Taiwan UC 1. 07 per 105 inhabitants 81% 0. 59 0. 17 59% 0. 27 CD per 105 inhabitants Inflamm Bowel Dis 2013; 19: 2815
 Ulcerative colitis Crohn’s disease Dignass A, et al. J Crohns")
Inflammatory bowel disease (IBD) Ulcerative colitis Crohn’s disease Dignass A, et al. J Crohns Colitis 2012; 6: 965– 990 J Chin Med Assoc 2012; 75: 151
 Ulcerative Colitis Target organ: colon Histopathology: goblet cell depletion, crypt")
Inflammatory bowel disease (IBD) Ulcerative Colitis Target organ: colon Histopathology: goblet cell depletion, crypt abscess Endoscopy: diffuse, continuous from rectum Clinical feature: chronic mucosal inflammation, Complication: dysplasia-colitic cancer, PSC, skin lesion, etc Dignass A, et al. J Crohns Colitis 2012; 6: 965– 990 J Chin Med Assoc 2012; 75: 151

UC: Clinical Features Proctitis 41% Left-sided colitis 37. 9% Pancolitis 21. 1% Rectal Rx Rectal + Systemic ● Tenesmus, urgency ● Faecal incontinence ● Passage of mucus and fresh blood ● Bloody diarrhoea ● Sometimes proximal constipation Poor prognosis: Pancolitis, Steroids, Young age, high CRP/ESR ● ● Diarrhoea Weight loss Fever Clinically significant blood loss ● Abdominal pain Dignass A, et al. J Crohns Colitis 2012; 6: 965– 990 J Chin Med Assoc 2012; 75: 151

Disease extent: as a predictor of long-term disease outcome in UC 35 30 25 20 15 10 5 0 Colorectal cancer in UC after 25 years 2 35% N=1161 19% 9% Proctitis Left-sided colitis Observed cases Percent Colectomy in UC after 5 years 1 Extensive colitis 80 N=3117 65 60 40 20 0 17 9 Proctitis Left-sided colitis Extensive colitis Standardised mortality ratio in UC after 10 years 3 2. 5 Ratio 2. 0 N=2509 1. 5 1. 0 0. 5 0 Proctitis Left-sided colitis Extensive colitis Langholz E, et al. Gastroenterology 1994; 103: 1444– 51 Ekbom A, et al. New Eng J Med 1990; 323: 1228– 33 Ekbom A, et al. Gastroenterology 1992; 103: 954– 60 12

Utilize Mayo Score to Clinical Activity Severity of disease Mayo index Mayo Subscore 0 1 2 3 Stool frequency Normal 1– 2/day >normal 3– 4/day >normal 5/day >normal Rectal bleeding None Streaks Obvious Mostly blood Mucosa Normal Mild friability Physician’s global assessment Normal Mild 0 1 Moderate Spontaneous friability bleeding Moderate 2 Severe 3 De Chambrun GP, et al. Nat Rev Gastroenterol Hepatol. 2010; 7 15 -29.
 Crohn’s disease Target organ: mouth ~ anus (entire digestive organ)")
Inflammatory bowel disease (IBD) Crohn’s disease Target organ: mouth ~ anus (entire digestive organ) Histopathology: granuloma, fissuring ulcer Endoscopy: longitudinal ulcer, cobble stone appearance, skip lesion Clinical feature: transmural inflammation, Complication: fistula, stenosis, anal lesion, skin lesion, etc Pariente B, et al. Inflamm Bowel Dis 2011; 17: 1415– 22

Crohn’s Disease is a Progressive Disease Progression of digestive damage and inflammatory activity in a theoretical patient with Crohn’s disease (消化道損害與發炎在CD病患身上會持續惡化) Stricture Fistula/abscess Stricture Disease onset Diagnosis Early disease Pariente B, et al. Inflamm Bowel Dis 2011; 17: 1415– 22 Inflammatory activity (CDAI, CDEIS, CRP) Digestive damage Surgery

Crohn’s Disease: 腸道內常見的併發症 50% 狹窄 30% 發炎 20% 廔管 https: //gi. jhsps. org/GDL_Disease. aspx? Current. UDV=31&GDL_Cat_ID=024 CC 2 E 1 -2 AEB-4 D 50 -9 E 02 -C 79825 C 9 F 9 BF&GDL_Disease_ID=291 F 2209 -F 8 A 94011 -8094 -11 EC 9 BF 3100 E

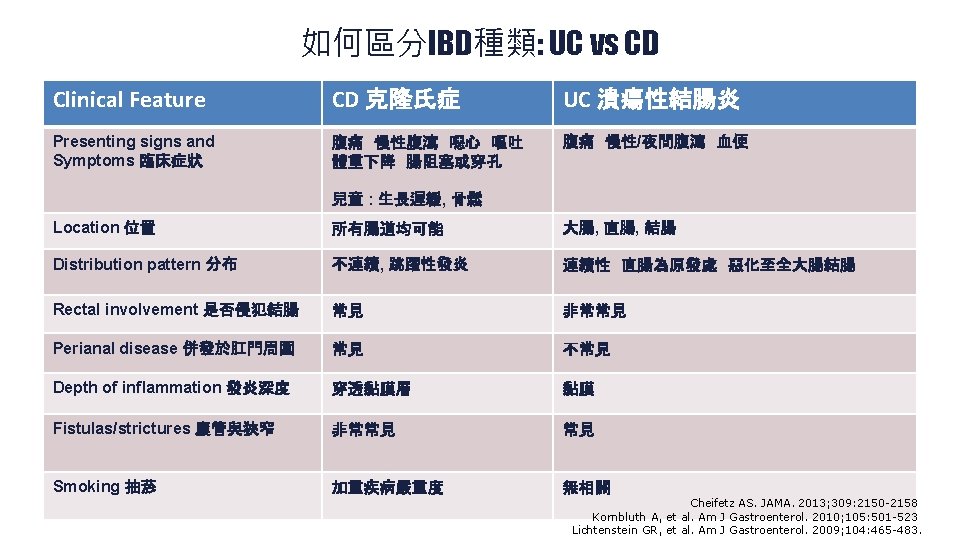
CD 與 UC: 臨床病灶、內視鏡與病理定義 https: //gi. jhsps. org/GDL_Disease. aspx? Current. UDV=31&GDL_Cat_ID=024 CC 2 E 1 -2 AEB-4 D 50 -9 E 02 -C 79825 C 9 F 9 BF&GDL_Disease_ID=291 F 2209 -F 8 A 94011 -8094 -11 EC 9 BF 3100 E

IBD: 腸道外的併發症 Dermatologic – Erythema nodosum, pyoderma gangrenosum • Hematologic – Anemia, venous thromboembolism • Hepatobiliary – Cholelithiasis, PSC – Musculoskeletal – Peripheral arthralgias and arthritis, spondyloarthritis • Ocular – Episcleritis, uveitis, scleroconjunctivitis • Renal – Nephrolithiasis 19 PSC = primary sclerosing cholangitis. Kornbluth A, et al. Am J Gastroenterol. 2010; 105: 501 -523; Lichtenstein GR, et al. Am J Gastroenterol. 2009; 104: 465 -483; Peyrin-Biroulet L, et al. Inflamm Bowel Dis. 2011; 17: 471 -478; Rothfuss KS, et al. World J Gastroenterol. 2006; 12: 4819 -4831.

Treatment Goals in IBD

預測 IBD疾病可能的病程 幾種可能的 IBD疾病惡化方式 腸道症狀的嚴重度 43% 0 預測較嚴重的 IBD 病程 Predictors 3% 10 yrs · 40 歲前確診 0 19% 10 yrs 32% · 肛門周圍潰瘍 · 需提前使用類固醇 · 嚴重的內視鏡潰瘍 0 10 yrs Solberg IC, et al. Clinical Gastroenterol Hepatol 2007; 5: 1430– 1438 不過, 目前缺乏bio-marker 來預測可能的疾病病程! Beaugerie L, et al. Gastroenterology 2006; 130: 650– 656 Lee JC, et al. J Clin Invest 2011; 121: 4170– 4179 Henckaerts L, et al. Clin Gastroenterol Hepatol 2009; 7: 972– 980 Solberg IC, et al. Clin Gastroenterol Hepatol 2007; 5: 1430– 8 Munkholm P, et al. Scan J Gastroenterol 1995; 30: 699– 706 Allez M, et al. Am J Gastroenterol 2002; 97: 947– 953 Weersma RK, et al. Gut 2009; 58: 388– 395 Rutgeerts P, et al. Gastroenterology 1990; 99: 956– 963

IBD的治療目標 改善疾病惡化 深部緩解 1, 3 黏膜癒合 1, 2 無類固醇緩解 臨床緩解 改善臨床症狀 治療策略需要訂定明確 的治療目標 1. Colombel JF, et al. N Engl J Med. 2010; 362(15): 1383 -95. 2. Baert FJ, et al. Gastroenterology 2010; 138(2): 463 -8. 3. Colombel JF, et al. Clin Gastroenterol Hepatol. 2013 Jul 12.

What is the Optimal Target? Symptoms Qo. L PCDAI Mucosal healing Colonscope: CDEIS, SES-CD Image: MRE, CTE 1. Colombel JF, et al. N Engl J Med. 2010; 362(15): 1383 -95. 2. Baert FJ, et al. Gastroenterology 2010; 138(2): 463 -8. 3. Colombel JF, et al. Clin Gastroenterol Hepatol. 2013 Jul 12. Laboratory CRP ESR Calprotectin Deep remission Disease modification Stricture, Fistula Surgery

我們可以選擇的治療策略 Severe Moderate IMS + TNF antagonist Corticosteroids + IMS 保守型 step-care 加速型 step-care IMS, immunosuppressive; TNF, tumour necrosis factor. Ordás I, et al. Gut. 2011; 60(12): 1754 -63. IMS + TNF antagonist 積極型 top-down

Sequential Therapies for IBD Disease Severity at Presentation Cyclosporine Colectomy Anti-TNF +/-IS Anti-Integrin +/- IS Severe Moderate Corticosteroid Mild Aminosalicylate Oral/Topical/Combo Anti-TNF/Anti-Integrin +/- IS Aminosalicylate/ Thiopurine Induction Maintenance Therapy is stepped up according to severity at presentation or failure at prior step Ordás I, et al. Gut. 2011; 60(12): 1754 -63.

Leading change: Local and Global Perspective Focus on Crohn’s Disease Management: treatment goals Treatment goals in IBD: can our current therapies deliver? 5 -ASA, mesalazine; AZA, azathioprine; MTX, methotrexate. Rutgeerts P, et al. Gastroenterology 2012; 142: 1102– 11 Colombel JF, et al. N Engl J Med 2010; 362: 1383– 95 Feagan B, et al. N Engl J Med 1995; 332: 292– 7 Candy S, et al. Gut 1995; 37: 674– 8 Lakatos PL, et al. Am J Gastroenterol 2012; 107: 579– 88 Sandborn WJ, et al. Gastroenterology 2012; 142: 257– 65 Ardizzone S, et al. Gut 2006; 55: 47– 53 Peyrin-Biroulet L, et al. J Crohns Colitis 2011; 5: 477– 83

The Role of Biologics in IBD Treatment

The Map of Inflammation in IBD Nature Reviews Gastroenterology & Hepatology 12, 271– 283
")
Structure of Different TNF Antagonists D. Tracey et al. Pharmacology & Therapeutics 117 (2008) 244 -279

Anti-α 4β 7 Anti TNF-α Availability and drug labelling of biologic agents for IBD Nature Reviews Gastroenterology & Hepatology 12, 537– 545 (2015)


Adalimumab – for Moderate to Severe Crohn’s Disease Patients CLASSIC 1: Induction of remission and response at Week 4 c d b e a ap < 0. 001; bp < 0. 05; cp = 0. 01; dp = 0. 007; ep = 0. 002 Clinical response Δ 70 or Δ 100 = CDAI* decreases from baseline ≥ 70 or ≥ 100 Hanauer SB, et al. Gastroenterology. 2006; 130: 323 -33.

CLASSIC II Adalimumab – for Moderate to Severe Crohn’s Disease Patients CLASSIC 2: Maintenance of remission and response through Week 56 (CDAI < 150) HUMIRA 40 mg weekly Placebo 94* 100 90 80 Patients (%) HUMIRA 40 mg eow 83* 84* 70 79* 60 50 40 30 50 20 10 0 4 8 12 16 20 24 28 32 Weeks LOCF; ITT population, n=55; *p<0. 05 versus placebo Sandborn WJ, et al. Gut. 2007; 56(9): 1232 -9. 36 40 44 48 52 56

Adalimumab – for Moderate to Severe Crohn’s Disease Patients CLASSIC 2: Safety analyses to the end of Week 56 Sandborn WJ, et al. Gut. 2007; 56(9): 1232 -9. Presentation Title | Date xx. xx | Company Confidential © 2012 37

Adalimumab – for Moderate to Severe UC Patients ULTRA 2: Induction of remission, response and mucosal healing at Week 8 Placebo (n=246) Proportion of patients (%) 100 HUMIRA 160/80* (n=248) p<0. 001 80 p=0. 032 60 50. 4 p=0. 019 40 20 0 41. 1 34. 6 31. 7 16. 5 9. 3 Clinical Remission Clinical Response Mucosal Healing Co-primary endpoint # Clinical remission: Mayo score ≤ 2 with no individual subscore >1. # Clinical response per partial Mayo score: decrease in Mayo Score ≥ 3 points and ≥ 30% from baseline, with a decrease in the rectal bleeding subscore ≥ 1 or an absolute rectal bleeding subscore of 0 or 1. # Mucosal healing: endoscopy subscore of 0 or 1. *160/80 mg HUMIRA at Week 0/2; 40 mg HUMIRA every other week beginning at Week 4 Sandborn WJ, et al. Gastroenterology 39 2012; 142: 257– 65

Adalimumab – for Moderate to Severe UC Patients ULTRA 2: Maintenance of remission and response at Week 52 (Week 8 ADA responders) Week 52 clinical remission Patients (%) 80 ADA, ITT 100 ADA Wk 8 responders 60 40 20 0 30. 9 28. 8 80 Patients (%) 100 17. 3 N=248 Week 52 clinical response ADA, ITT 60 40 ADA Wk 8 responders 49. 6 47. 2 30. 2 20 N=123 N=125 ADA (PMS) ADA (FMS) Non-responder imputation ITT, intent to treat; PMS, partial Mayo score; FMS, full Mayo score 0 N=248 N=123 N=125 ADA (PMS) ADA (FMS) Non-responder imputation Sandborn W, et al. ECCO 2012; P 207 Sandborn W, et al. Aliment Pharmacol Ther 2013; 37: 204– 13 Sandborn W, et al. Gastroenterology 2012; 142: 257– 65

ULTRA 2: treatment emergent adverse events in double blind period, safety analysis set Placebo (N = 260) Any adverse event Any AE at least possibly drug related Any serious AE Any AE leading to discontinuation of study drug Any infectious AE Any serious infectious AE Any malignancy Any Non-melanoma skin cancer (NMSC) Any malignant AE (excluding NMSC and lymphomas) Any malignant AE (including lymphomas and exclude NMSC) Any injection site reaction Any opportunistic infection (excluding TB) Any congestive heart failure Any demyelinating disease Any hepatic AE Any allergic reaction Any lupus-like syndrome Any hematologic AE Death Sandborn WJ, et al. Gastroenterology Vol. 142, Issue 2, Pages 257 -265. e 3 n (%) 218 (83. 8%) 86 (33. 1%) 32 (12. 3%) 33 (12. 7%) 103 (39. 6%) 5 (1. 9%) 0 0 10 (3. 8%) 3 (1. 2%) 0 0 7 (2. 7%) 1 (0. 4%) 0 0 0 E (E/100 PY) 1007 (845. 9) 202 (169. 7) 44 (37. 0) 47 (39. 5) 175 (147. 0) 7 (5. 9) 0 0 17 (14. 3) 3 (2. 5) 0 0 11 (9. 2) 1 (0. 8) 0 0 0 ADA 160/80 mg (N = 257) n (%) 213 (82. 9%) 101 (39. 3%) 31 (12. 1%) 22 (8. 6%) 116 (45. 1%) 4 (1. 6%) 2 (0. 8%) 1 (0. 4%) 31 (12. 1%) 5 (1. 9%) 1 (0. 4%) 0 10 (3. 9%) 4 (1. 6%) 1 (0. 4%) 5 (1. 9%) 0 E (E/100 PY) 1083 (744. 0) 271 (186. 2) 45 (30. 9) 24 (16. 5) 210 (144. 3) 4 (2. 7) 2 (1. 4) 1 (0. 7) 58 (39. 8) 6 (4. 1) 1 (0. 7) 0 16 (11. 0) 4 (2. 7) 1 (0. 7) 5 (3. 4) 0

Adalimumab treated UC case sharing Baseline Week 8 Week 26 Week 8 D R Mayo endoscopic subscore Mayo score 2 9 2 7 0 0 2 Adapeted from Dr. Tu’s slides.

Overall conclusions • IBD is a chronic, progressive inflammatory disease. • Impact of IBD on patients is highly burdensome: it affects the physical, social, and psychosocial wellbeing of patients. • Goals of therapy include: – Inducing and maintaining remission of symptoms and mucosal healing – Reducing the risk of complications – Avoiding the need for surgery – Improved survival • Biologics provide a promising treatment choice for IBD patients to achieve remission and mucosal healing. 43

- Slides: 44