Current Clinical Practice for Cholecystectomy after ERCP 2018



, which enlarges biliary")











")
 ≥ 18 in age with admission,")
 l Planned CCY within")
 at 365 days after")









 – Missing patients who")

- Slides: 35
Current Clinical Practice for Cholecystectomy after ERCP 2018. 06. 21. R 3 이철형 / Pf. 안동원
Introduction l Gallstone disease affects >20 million Americans annually, estimated costs at $6 billion l Choledocholithiasis typically originate from GB, complicates biliary obstruction, ascending cholangitis, gallstone pancreatitis l Cholecystectomy(CCY) after endoscopic retrograde cholangiopancreatography(ERCP) reduces recurrent biliary events comparing to expectant managemet
Introduction l In clinical settings, clinicians somewhat reluctant to undergo surgery d/t patient’s age, comorbidities l There are no societal guidelines regarding the optimal timing for CCY after choledocholithiasis requiring ERCP and practice patterns are variable among institutions
Background − Endoscopic removal of biliary stones need endoscopic spincterectomy (ES), which enlarges biliary orifice, allowing passage of future stones − Previous studies revealed ES with CCY is superior to ES alone for surgically fit candidates − To assess CCY after ES for elderly patients, whom clinicians may defer CCY
Methods Design l Retrospective, cohort study l Patients ≥ 65 in age with choledocholithiasis after performing ES l Advantages of follow up CCY compared to surgical adverse events l 1 st Jan, 2009 ~ 31 Dec, 2014, The Truven Health Analytics Market. Scan databases
Methods Study sample l International Classification of Diseases, 9 th revision, Clinical Modification (ICD-9 -CM) diagnosis codes l Current Procedural Terminology (CPT) codes l Identify Patients ≥ 65 in age, who underwent ES for choledocholithiasis, ascending cholangitis, or gallstone pancreatitis l Exclusion criteria – underwent CCY prior to index ES – Diagnosis Code ‘V 4579’ other acquired absence of organ l Divided into two groups, whether or not underwent CCY within 30 days of index ES
Methods Outcomes l Age, gender, Charlson comorbidities l Primary endpoints: choledocholithiasis, ascending cholangitis, gallstone pancreatitis, cholecystitis after 31 -365 days of Tx (index ES vs cholecystectomy for ES+CCY) – Chi test/Fischer’s test or Wilcoxon Rank Sum test – Multivariable logistric regression and propensity score matching l Secondary analysis: risk ratio of potential surgical complications within 30 days of CCY (ES+CCY group) or index ES (ES only)
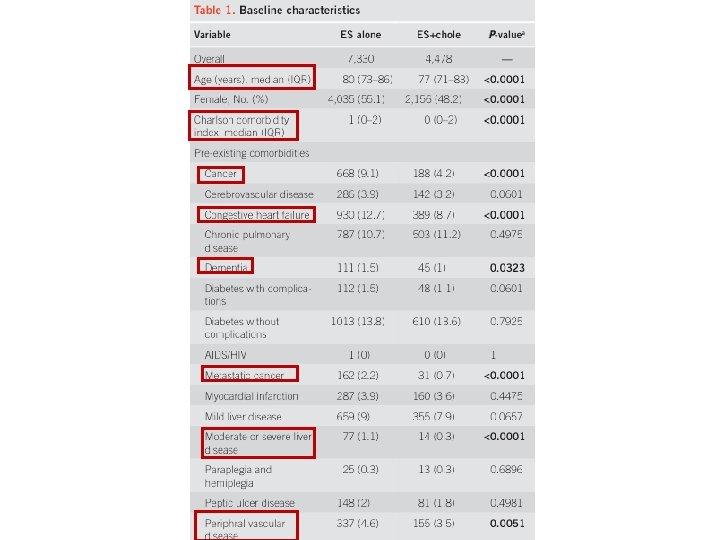
Results B. Joseph Elmunzer et al. Am J Gastroenterol 2017 112, 1596– 1602
Results ES alone 39. 3% vs ES+CCY 18. 0% in recurrent complication 16% of ES only group underwent subsequent CCY B. Joseph Elmunzer et al. Am J Gastroenterol 2017 112, 1596– 1602
Results B. Joseph Elmunzer et al. Am J Gastroenterol 2017 112, 1596– 1602
Results B. Joseph Elmunzer et al. Am J Gastroenterol 2017 112, 1596– 1602
Results B. Joseph Elmunzer et al. Am J Gastroenterol 2017 112, 1596– 1602
Results B. Joseph Elmunzer et al. Am J Gastroenterol 2017 112, 1596– 1602
Discussion l Large retrospective analysis, including elderly patients with major comorbidities l High 1 year f/u complications for ES alone (39. 3%) compared with ES+CCY group (18. 0%) l Limitations – Data quality from large insurance database – Causal interference d/t confounders – Selection bias – “carry forward diagnosis” – may inflate overall complications – Cannot exclude all people with prior CCY
Discussion l Adequacy of sphincterectomy? l Follow up cholecystectomy after ES for bile duct stones reduced risk of biliary complications about 50 -70% among elderly patients l Benefits does not outweighed by surgical complications
Methods Design l Retrospective, longitudinal, cohort study l Healthcare Cost and Utilization Project (HCUP) l Datas from 3 largest states, California (2009 -2011), New York (2011 -2013), Florida (2012 -2014) : ambulatory surgery, inpatient, emergency department databases l Utilizes ICD-9 -CM codes
Methods Cholecystecomy Cohorts l Inclusion criteria (5831 patients) ≥ 18 in age with admission, underwent ERCP with sphincterectomy/ stone extraction for choledocholithiasis/ in situ gallbladder with cholelithiasis **without concomitant cholecystitis l Exclusion criteria history of biliary stone disease, biliary stricture, cholangitis, peribiliary malignancy, prior bile duct surgery, prior percutaneous biliary drainage, severe acute pancreatitis l Total 4516 patients analyzed
Methods Cohorts l Underwent CCY during index admission (early CCY) l Planned CCY within 60 days of discharge (delayed CCY) l Did not undergo CCY within 60 days of discharge (no CCY)
Methods Outcomes l Primary outcome: rate of recurrent biliary event(RBE) at 365 days after discharge from index admission – symptomatic cholelithiasis, cholecystitis, choledocholithiasis, cholangitis, biliary pancreatitis l Rates of RBE were compared within 60 days of discharge and after 60 days – Within 60 days, delayed-CCY and no-CCY cohorts => composite cohort – If patients in the composite cohort underwent an elective CCY within 60 d, censored from observation on that date l Patients included after 60 days only if they survived the first 60 days without events
Methods Outcomes l Secondary outcomes: 1> mortality, both related to RBE and all cause at 365 d after d/c 2> total facility charges (NY, FL) l Covariates for adjustment – Demographic information, socioeconomic information, primary payer (insurance), patient comorbidities using Charlson Comorbidity Index (CCI) – Facilities classified by annual CCY volume (low – medium – high) l Statistical analysis – Kaplan-Meier: survival of each cohorts, compared with log-rank test – Rate of RBE: proportional hazards analysis
Results Robert J. Huang et al. Gastroenterol 2017, 153: 762 -771
Results Robert J. Huang et al. Gastroenterol 2017, 153: 762 -771
Results A. Early CCY 1. 0% vs delayed/no-CCY 11. 7% B. no-CCY had a cumulative RBE incidence of 10. 3% early / delayed CCY shows 1. 4% / 1. 3% 15 in no-CCY / 1 in early CCY died d/t RBE related hospitalization ÞRBE related mortality 16 fold higher ÞAll cause mortality 68 in no-CCY, 11 in early CCY => 7 fold higher Robert J. Huang et al. Gastroenterol 2017, 153: 762 -771
Results Robert J. Huang et al. Gastroenterol 2017, 153: 762 -771
Results Robert J. Huang et al. Gastroenterol 2017, 153: 762 -771
Results Robert J. Huang et al. Gastroenterol 2017, 153: 762 -771
Discussion l 41% of patients have undergone CCY of index admission, additional 11% undergone delayed CCY within 60 days l 48% patients fail to undergo CCY within 60 days of discharge l Performance of CCY (early or late) was protective against RBE, approximately 90% – Patients are at 10 -fold higher risk of RBE during awaiting delayed CCY l Predictors of early CCY: CCY volume of hospital, regional variations – Median income or insurance did not affect the rate of early CCY l Predictors of delayed CCY: race, insurance – Barriers of culture, language, medical literacy
Discussion l Early CCY strategy is preferable regarding to RBE and mortality – Substantial patients will have an RBE while awaiting delayed CCY – Important to patients with minority ethnicity, Medicaid or no insurance l Delayed CCY offer the merit of lower healthcare charge l No CCY is costlier than delayed CCY – And may also applied to early CCY
Discussion l Limitation – Restrospective study, confounding biases (medical comorbidities) – Missing patients who are moving in/out l Analyzed patients almost ¼ population of US l Data represents across the health care spectrum and actual clinical practices
Conclusion l Timely cholecystectomy after ERCP for choledocholithiasis have not done sufficiently d/t multifactorial reasons. l Clinicians should actively consider early/delayed cholecystectomy regarding to patient’s ethnicity, medical literacy and insurance status l Furthur prospective researches should be done regarding to patient comorbidities and evaluate actual risk of undergoing surgery l Innate limitations d/t retrospective study, need more sophisticated prospective study