Culture of Patient Safety Nurses Role in Establishment

Culture of Patient Safety: Nurse’s Role in Establishment and Sustainment Pat Posa RN, BSN, MSA, CCRN-K, FAAN Quality Excellence Leader St. Joseph Mercy Health Sytem Ann Arbor, MI patposa@gmail. com
 • Discuss 3")
Objectives • Understand the key components of High Reliable Organizations (HRO) • Discuss 3 components of HRO – Leadership commitment – Adoption of Safety Culture – Robust Process Improvement • Review strategies to create a culture of safety 2

How are we doing in preventing harm?

Value Sets Platform for Performance Improvement The Vision of Health Care in the U. S. –NOW- • Fragmented • Fee-for-service Cost Volumedriven healthcare • Connected • Bundled • Accountable VALUE- driven healthcare Quality 4

Hospital Performance Based Payments Hospital Acquired Conditions Ø 1% reduction to total DRG payments Readmissions Ø 3% reduction 8% of Based DRG Payments at Risk by 2017 EMR Meaningful Use Requirements Ø Reductions up to ¾ of update factor Value Based Purchasing (VBP) Ø 2% reduction

What is Patient Safety? Patient safety was defined by the IOM as “the prevention of harm to patients. ” Emphasis is placed on the system of care delivery that: (1) prevents errors (2) learns from the errors that do occur (3) is built on a culture of safety that involves health care professionals, organizations, and patients. Aspden P, Corrigan J, Wolcott J, et al. , editors. Patient safety: achieving a new standard for care. Washington, DC: National Academies Press; 2004. 6

Gains and Opportunities • Pockets of excellence coexist with enormously variable performance across the delivery system – In 2009, hospitals on average provided life-prolonging beta-blockers to heart attack patients 98% of the time. 97% of hospitals scored above 90% on this measure • BUT: – We have eluded thus far the ability to maintain consistently high levels of safety and quality over time and across all health care services and settings – We are experiencing an epidemic of serious and preventable adverse events – Risk of harmful error in health care may be increasing as the complexity of delivering effective care increases Chassin & Loeb, Health Affairs, April 2011 7

High Reliability Organizations • High Reliability: consistent performance at high levels of safety over long periods of time • Possess “Collective mindfulness” – Means that everyone who works in these organizations, both individually and together, is acutely aware that even small failures in safety protocols or processes can lead to catastrophic adverse events, if some action is not taken to solve the problem • Two other features: – Eliminate deficiencies in safety processes through the use of powerful tools to improve their processes – Create an organizational culture that focuses on safety, in which they remain constantly aware of the possibility of failure Chassin & Loeb, Health Affairs, April 2011; Chassin & Loeb, The Milbank Quarterly, Vol 91 No 3, 2013 pp 459 -490 8

Five Principles of High Reliability Anticipation—”Stay out of Trouble” Manage the Expected 1. Preoccupation with failure 2. Sensitivity to operations 3. Reluctance to simplify Containment – “Get out of Trouble” Manage the Unexpected 4. Commitment to resilience 5. Deference to expertise

Five Principles of High Reliability 1. Preoccupied with failure – Always alert to the smallest signal that a new threat to safety may be developing 2. Resist temptation to simplify their observation and their experiences of their environment – Threats to safety can be complex and present themselves in many ways 3. Sensitivity to operations – Earliest indicators of threats to organizational performance typically appear in small changes in the organizations operations; – therefore they make sure that all workers involved in operations report any deviations from the expected performance – Make sure everyone not only feels free to speak up but recognized their obligation to do so Managing the Unexpected; Weick, K and Sutcliff, K. 2007 10

Five Principles of High Reliability 4. Commitment to resilience – An organization’s capability to recognize errors quickly and contain them, thereby preventing harm 5. Deference to expertise – Enhance their resilience – When confronted with a new threat, identify the individual with the greatest expertise relevant to managing the new situation and place the decision making plans/authority with that person or group March 13, 2015 Center for Patient Safety 9 th Annual Patient Safety Conference 11

• Leadership engagement • Culture of safety • Implementation framework that deals with both technical and adaptive change Chassin & Loeb, Health Affairs, April 2011; Chassin & Loeb, The Milbank Quarterly, Vol 91 No 3, 2013 pp 459 -490

High Reliability Maturity Model: Components Leadership Commitment Safety Culture • Board • CEO/Management • Physicians • Quality Strategy • Quality Measures • Information Technology • Trust • Accountability • Identify Unsafe Conditions • Strengthening Systems • Assessment Process Improvement • Methods • Training • Spread Stages of Maturity Beginning Developing Advancing Approaching

High Reliability: Stages of Maturity Source: Du. Pont Sustainable Solutions

Leadership Commitment

Leadership • Alignment and agreement of the Board, senior management, physicians and nurse leaders – Must share the vision of eventually eliminating all harm to patients (and employees) • Not satisfied with current level of safety; always looking to improve Target Zero

Leadership • Ensure quality strategy and measures align and support journey to zero harm • Motivate staff to uphold a fair and just safety culture • Provide a transparent environment in which patient safety events are honestly reported • Model professional behavior • Remove intimidating behavior that might inhibit a culture of safety • Provide the resources and training necessary to take on improvement initiatives

Leadership • Walk Rounds – Vice President or higher – Support the work of the team – Round on unit – be purposeful… • Script the rounds – How will the next patient in this unit be harmed? – How can I help to remove barriers, so that the safety defects you are most concerned about can be better addressed? – How well does teamwork occur on this unit? – What doesn’t work well? • If there is a learning board, use this as the meeting point on the unit. Source: Sexton, JB, Engaging Leaders Webinar, 2010 18

Goals of Executive Safety Partnerships • Near Term Goal: to build capacity for quality improvement within the unit • Medium Term Goal: to have staff bring up solutions rather than problems • Long Term Goal - For staff to say: – – “We don’t need to meet monthly with the executive” “I would feel safe being treated here as a patient” “I felt like I was heard today” “I made a difference today” 19

Do you have the right structure? Donebedian Model Structure Process Outcome 1. What is your quality structure? 2. Do you have physician co-leading/involved in QI activities? 3. Patient care unit leadership– Unit care teams: Medical Director, Nurse manager, Clinical Nurse Leader/CNS, quality or performance improvement specialist 4. What is your shared governance structure? What role does your unit base practice council play in patient safety and quality?

High Reliability Maturity Model: Components Leadership Commitment Safety Culture • Board • CEO/Management • Physicians • Quality Strategy • Quality Measures • Information Technology • Trust • Accountability • Identify Unsafe Conditions • Strengthening Systems • Assessment Process Improvement • Methods • Training • Spread Stages of Maturity Beginning Developing Advancing Approaching

Create a Culture of Safety

Safety Culture Components in HRO Component Description Trust Workers exhibit enough trust in their peers and management that they routinely recognize and report errors and unsafe conditions. Eliminate intimidating behavior Accountability Establish codes of behaviors. Establish equitable disciplinary procedures and a safety culture that supports personal accountability. Just Culture Identifying Unsafe Conditions Retrospective analysis of reported adverse events moving toward reporting and analysis of close calls and unsafe conditions to correct situation before harm occurs Strengthening Systems Evaluate safety systems (as opposed to isolated safety events) proactively so weaknesses can be identified and resolved Assessment Measure culture of safety and define focused interventions to remedy where fall short

Medical errors most often result from a complex interplay of multiple factors. Only rarely are they due to the carelessness or misconduct of single individuals. Lucien L. Leape, MD Harvard School of Public Health 24

Key Component of a Safe Culture “A fundamental principle has to be the development and then enforcement of procedures and standards. We can’t make real progress without them. When a (caregiver) doesn’t follow them, something has to happen. Today, nothing does, and you a have vicious cycle in which people have no real incentive to follow the rules because they know there are no consequences if they don’t. So there are bad doctors and bad nurses, but the fact that we tolerate them is just another systems problem. ” Dr. Lucian Leape

Balance no-blame with accountability =Just Culture 1 • A system that: - Holds itself accountable - Holds staff members accountable - Has staff members who hold themselves accountable 26

Introduction to Just Culture Principles 27

Understanding Risk and Human Behavior 1 At-Risk Behavior: Choosing to behave Human Error: in a way that Inadvertently increases risk where completing the wrong risk is not action; slip, lapse, recognized, or is mistakenly believed to be justified Reckless Behavior: Choosing to consciously disregard a substantial and unjustifiable risk 28

Managing Error and Risk 1 Human Error At-Risk Behavior Reckless Behavior Product of our current system design and behavioral choices A choice: risk believed insignificant or justified Conscious disregard of substantial and unjustifiable risk Manage through changes in: • Choices • Processes • Procedures • Training • Design • Environment Manage through: • Removal of incentives for atrisk behaviors • Creation of incentives for healthy behaviors • Situational awareness Manage through: • Remedial action • Punitive action Console Coach Punish 29

A Positive Culture of Safety …. . recognizes the inevitability of error and proactively seeks to identify latent threats 30 Nieva, V F Qual Saf Health Care 2003; 12(suppl)
 to improve our Safety Culture •")
We used CUSP (Comprehensive Unit based Safety Program) to improve our Safety Culture • Created through a collaborative effort of the Agency for Healthcare Research and Quality and state and national-level innovators in patient safety • Dovetails with, and supports, a range of quality and safety improvement models • Encompasses a wide range of safety tools and approaches • Based on the understanding that all culture is local, and that work to improve culture must be owned at the unit level • Believes that harm is not an acceptable “cost of doing business” • Can be applied by anyone, anywhere

The Comprehensive Unit-based Safety Program 1. Educate on the Science of Safety 2. Identify Defects (Staff Safety Assessment) 3. Senior Executive Partnership 4. Learn from Defects 5. Implement Teamwork & Communication Tools www. ahrq/cusp

Safe Design Principles • Understand system determines performance • Use strategies to improve system performance – Standardize – Create Independent checks for key process – Learn from Mistakes • Apply strategies to both technical work and team work. • Recognize that teams make wise decisions with diverse and independent input CUSP: Science of Safety, AHRQ 33

How did we implement CUSP at St. Joe’s • Developed multidisciplinary team – Included all 3 ICUs, medical directors of each unit, nurse managers and CNLs, bedside RNs, respiratory therapy, pharmacy, nutrition, and physical/occupational therapy • Administered Culture of Safety Assessment • Educated team and then entire staff on ‘Science of Safety” – Put it into the orientation curriculum • Asked front line staff 2 questions: (identifying defects) – How will the next patient be harmed? – What can you do to prevent that harm? – These question became part of Executive Safety Rounds

Continuing with CUSP Implementation • Senior Executive assigned to each unit – Held quarterly safety rounds in each unit – Identify 2 issues from each round and defined action plan to resolve. Share with staff at the next rounds

Focus on Learn from Defects

What Is a Defect? • Anything that you do not want to happen again.

Errors Provide Useful Information • We can learn more from our failures than from success • Our processes can be improved when studied “Give me a fruitful error anytime, full of seeds, bursting with its own corrections. You can keep your sterile truth to yourself. ” Vilfred Pareto ©copyright 2008 by the Trustees of Columbia University in the City of New York Rights Reserved 38

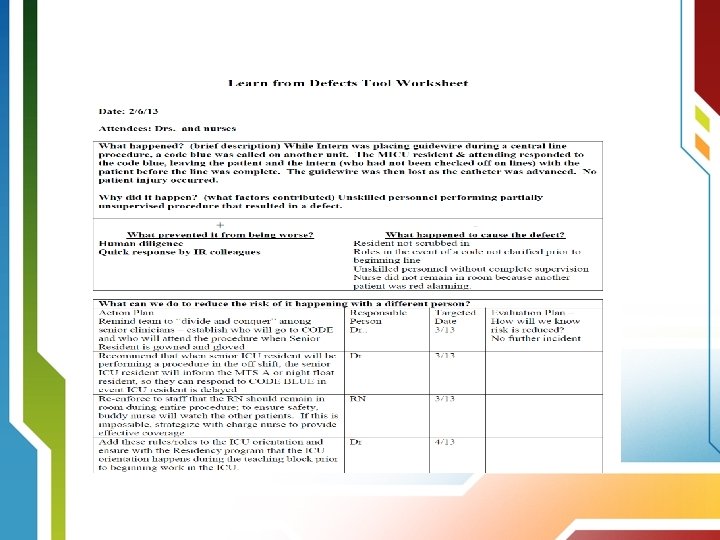
Learn from a Defect • Designed to rigorously analyze the various components and conditions that contributed to an adverse event and is likely to be successful in the elimination of future occurrences. • Tool can serve to organize factors that may have contributed to the defect and provides a logical approach to breaking down faulty system issues – Patient, team, task, caregiver factors – Training, education, technology factors – Local or institutional environment 39

Learning From Defects What happened? 1 Why did it happen? 2 How will you reduce it happening 3 again? How will you know the risk is 4 reduced? With whom will I share the 5 learnings From view of person involved

Brainstorm #1

Brainstorm # 2 Why Did It Happen?

Brainstorm # 3 Solution Finding…. All ideas are Welcome Necessary

Start with Low Hanging Fruit

A Good Solution Must Be… • Clear in how we measure the success • Trialable and easy to test • Compatible with or improve existing workflows • Low cost, low fidelity

Building Resiliency Into Interventions Forcing functions and constraints Automation and computerization Strongest Standardization and protocols Checklists and independent check systems Rules and policies Education and information Vague warnings – Be more careful! STRENGTH OF INTERVENTION 46 Weakest
 – Started doing one a")
Continuing with CUSP Implementation • Learning from defects (LFD) – Started doing one a quarter – Used this tool to resolve VOICE issues – Use LFD process to respond to staff’s response to “how will the next patient be harmed” – Rolled out housewide with expectation that each unit would do one per month – Expectation that every hospital acquired infection was reviewed using LFD – LFD used for post fall huddle and after skin injury

CLABSI LFD

Improve Communication and Teamwork
 51")
Communication Breakdowns Cause Treatment Delays Root Causes of Treatment Delays(1995 -2004) 51
 52")
Communication Breakdowns Cause Infection-associated Events Root causes of infection-associated events (2005) 52

Effective Teamwork’s Positive Impact on Health Care • • • Reduced length of stay Lower nurse turnover Higher quality of care Greater ability to meet family member needs Better patient outcomes Better patient experience with care scores 53

% of respondents within an ICU reporting good teamwork climate Teamwork Climate Across Michigan ICUs The strongest predictor of clinical excellence: caregivers feel comfortable speaking up if they perceive a problem with patient care No BSI = 5 months or more w/ zero No BSI 21% No BSI 31% No BSI 44%

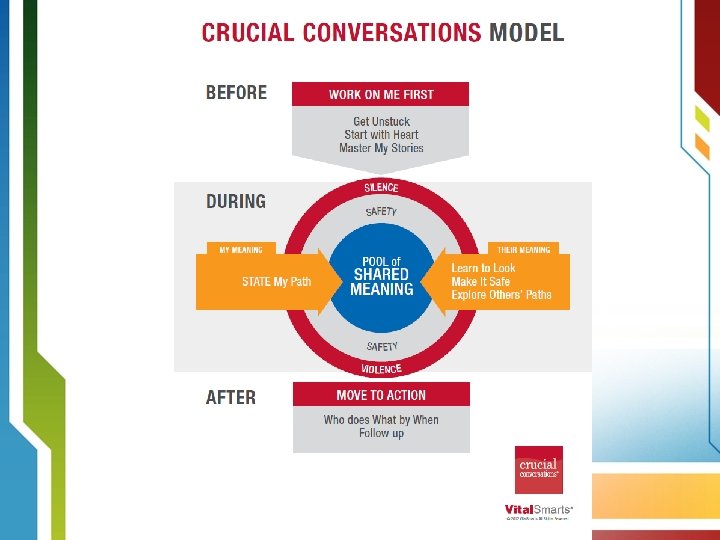
Tools and Strategies to Improve Safety and Teamwork • • • Learn from a defect SBAR (Team STEPPS) Daily rounds/goals Pre-procedure briefing (Team STEPPS) Morning briefing (Team STEPPS) Huddles Shadowing Crucial Conversations Executive Safety Rounds/Partnership Handoff standardization (Team STEPPS) 55

SBAR provides… • A framework for team members to effectively communicate information to one another • Communicate the following information: – – Situation―what is the situation? Background―what is the clinical background? Assessment―what is the problem? Recommendation―what do I recommend/request be done? Remember to introduce yourself… 56

Multidisciplinary Rounds with Daily Goals – What is it? • A strategy to assemble the patient care team members to review important patient care and safety issues and improve collaboration on the overall plan of care for the patient • Improve communication among care team and family members regarding the patient’s plan of care • Goals should be specific and measurable • Documented where all care team members have access • Checklist used during rounds prompts caregivers to focus on what needs to be accomplished that day to safely move the patient closer to transfer out of the ICU or discharge home • Measure effectiveness of rounds—team dynamics, communication, quality measure compliance, LOS 57

Evidence For Impact Of MDR Rounds • Research studies on the effect of structured interdisciplinary rounds show: – Earlier identification of clinical issues – More timely referrals – Improved ratings by nurses and physicians on teamwork, communication and collaboration. • Research also indicates variable effects on LOS and cost, with some studies showing improvement and others having no impact. Improving teamwork: impact of structured interdisciplinary rounds on a medical teaching unit. O'Leary KJ, et. al, Journal Of General Internal Medicine [J Gen Intern Med], ISSN: 1525 -1497, 2010 Aug; Vol. 25 (8), pp. 826 -32; PMID: 20386996 Bhamidipati, V. Elliott, D. et al. Structure and Outcomes of IDR in Hospitalized Medicine Patients: Systematic Review. Journal of Hosp Med Vol 11 No 7 July 2016 58

Multidisciplinary Rounds with Daily Goals Challenges and Opportunities • Should be done in ICUs and all units in hospital • Hard initiative to implement, especially if you have an open unit and/or no intensivists or in non-ICU area – Standardize the structure and process for all units – Benefits seen even if physician can not attend consistently or at all – Second rounds should be done in afternoon—include at least physician and bedside nurse • Evaluate if goals for day have been met; readjust if necessary • Identify if patient can be discharged (or transferred ) the next day and if so, what needs to be accomplished 59
 • Focused first on defining")
Multidisciplinary Rounds with Daily Goals Challenges and Opportunities (continued) • Focused first on defining daily goals and recording those either on the white board in the room or on a sheet of paper • Then standardize rounds—who should attend and what is discussed • Implemented nursing objective card—to clearly define role of nurse in multidisciplinary rounds 60

Critical Care Nursing Script for Rounds

Why Checklists? • Levels of cognitive function are often compromised with increasing levels of stress and fatigue in certain fields of work. • Aviation, aeronautics, and product manufacturing have come to rely heavily on checklists to aid in reducing human error. • The checklist is an important tool in error management across all these fields, contributing significantly to reductions in the risk of costly mistakes and improving overall outcomes. • Such benefits also translate to improving the delivery of patient care. • Despite demonstrated benefits of checklists in medicine and critical care, the integration of checklists into practice has not been as rapid and widespread as with other fields. J Crit Care 2003; 21: 233 6 2

Huddles • Enable teams to have frequent but short briefings so they can stay informed, review work, make plans, and move ahead rapidly. • Allow fuller participation of front-line staff and bedside caregivers, who often find it impossible to get away for the conventional hour-long improvement team meetings. • They keep momentum going, as teams are able to meet more frequently. • Use this strategy to begin to recover immediately from defects---IE: falls, sepsis. Use daily to focus on unit outcomes 63

Components Metric 1: Quality/Safety Metric 2: Patient Satisfaction Metric 3: Operations Daily Critical Communications Information Ideas in Motion How to do it? • Beginning or mid shift • 5 -10 minutes • Lead by member of unit leadership team 64

SICU Huddle Board 65

Surgical Unit Huddle Board

Medical Unit Huddle Board

Tools to help staff speak up Crucial Conversations Framework

High Reliability Maturity Model: Components Leadership Commitment Safety Culture • Board • CEO/Management • Physicians • Quality Strategy • Quality Measures • Information Technology • Trust • Accountability • Identify Unsafe Conditions • Strengthening Systems • Assessment Process Improvement • Methods • Training • Spread Stages of Maturity Beginning Developing Advancing Approaching

Process Improvement Components in HRO Component Description Methods Process improvement methods can vary. To be robust should include a combination of lean, six sigma, and change management Training Organization provides varying levels of training in performance improvement to staff inside and outside of the quality department Spread Nearly all employees should be trained at levels appropriate to each one’s job

Robust Process Improvement. Expectation around use of A 3

Journey to High Reliability “Free from Harm” • High Reliability: consistent performance at high levels of safety over long periods of time • We must strive to possess “Collective mindfulness” – Means that everyone who works in these organizations, both individually and together, is acutely aware that even small failures in safety protocols or processes can lead to catastrophic adverse events, if some action is not taken to solve the problem • Key components of high reliable organizations include: Leadership, Safety Culture and Robust Process Improvement • Achieving high reliability in hospitals will require substantial change over time

High Reliability in Health Care “The road to high reliability is an ongoing journey. It’s a commitment to patient safety and the way we deliver quality health care” Mark Chassin, Md, FACP, MPH President and Chief Executive Officer of The Joint Commission Resources available: http: //www. centerfortransforminghealthcare. org/hro_portal_main. aspx

THANK YOU
- Slides: 75