Cuerpo extrao digestivo CUERPO EXTRAO DIGESTIVO EPIDEMIOLOGIA u




 • SIALORREA • DISFAGIA")




 • ENDOSCOPIO FLEXIBLE O RIGIDO •")


















 • SIALORREA • DISFAGIA")




 • ENDOSCOPIO FLEXIBLE O RIGIDO •")

















- Slides: 64
Cuerpo extraño digestivo
CUERPO EXTRAÑO DIGESTIVO EPIDEMIOLOGIA u. El 80% de los casos ocurre en niños. u. La ingestión es accidental casi siempre. u. Generalmente son únicos. u. Ocurre estando al cuidado de sus padres. u. El 90% se elimina espontáneamente.
EDAD DE PRESENTACION u. El niño inicia la prehensión voluntaria y visualmente guiada entre los 3 y 6 m. u. A los 9 m. es capaz de coger un objeto. u. INGESTION DE CUERPO EXTRAÑO ENTRE LOS 6 M Y 3 AÑOS u. El adolescente ingiere cuerpos extraños mientras desarrolla sus actividades habituales por descuido
EDAD DE PRESENTACION
CUERPO EXTRAÑO DIGESTIVO FORMA DE PRESENTACION • ANTECEDENTE ( +) • SIALORREA • DISFAGIA ( ) • SENSACION DE CPO EXTRAÑO • TEMOR • ASINTOMATICO • ANTECEDENTE (-) • DISFAGIA ( ) • VOMITOS • TOS –DISFONIA • PLENITUD • COMPLICACIONES
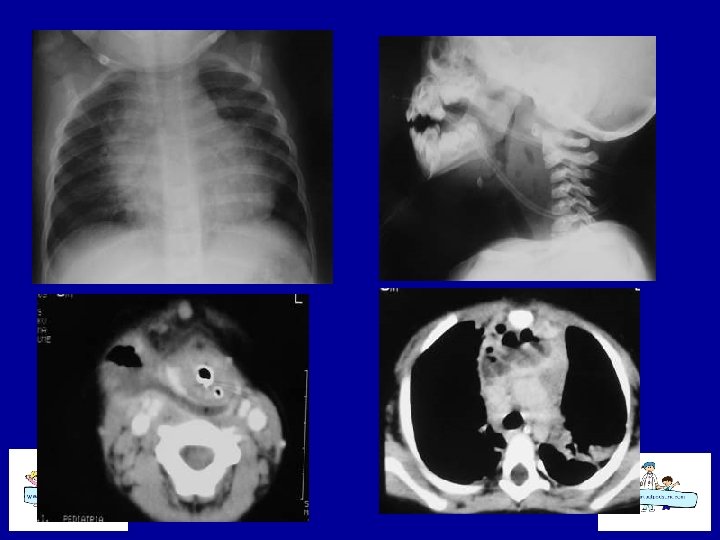
CUERPO EXTRAÑO DIGESTIVO UBICACIÓN DEL OBJETO • • • ESOF. SUP. ESOF. MEDIO ESOF INF ESTOMAGO DUODENO COLON
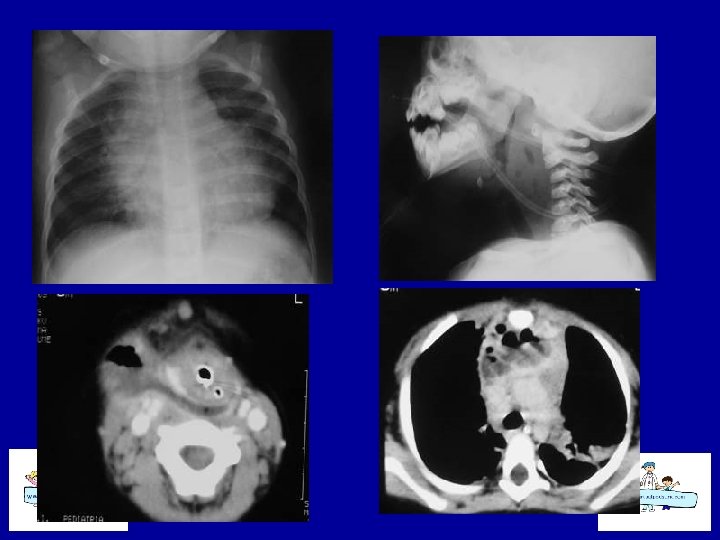
CUERPO EXTRAÑO DIGESTIVO METODO DIAGNOSTICO • ANAMNESIS • Rx SIMPLE: cuello, tórax y abdomen: siempre Ap y Lateral • Rx CONTRASTADA • ENDOSCOPÍA
CUERPO EXTRAÑO DIGESTIVO Patología Concomitante u ATRESIA ESOFAGICA OP. u R. G. E. RECIEN OP. u ESTENOSIS CONGÉNITA DEL ESOF. u OTRAS MALFORMACIONES DIGEST. u TRASTORNOS CONDUCTUALES
• OBJETOS • • • Moneda, Alfiler gancho, Alimentos Alfiler modista, Varios Metal Pila botón, Pilas, baterías Vegetal, Bolitas, vidrio Telas, latex, pelos
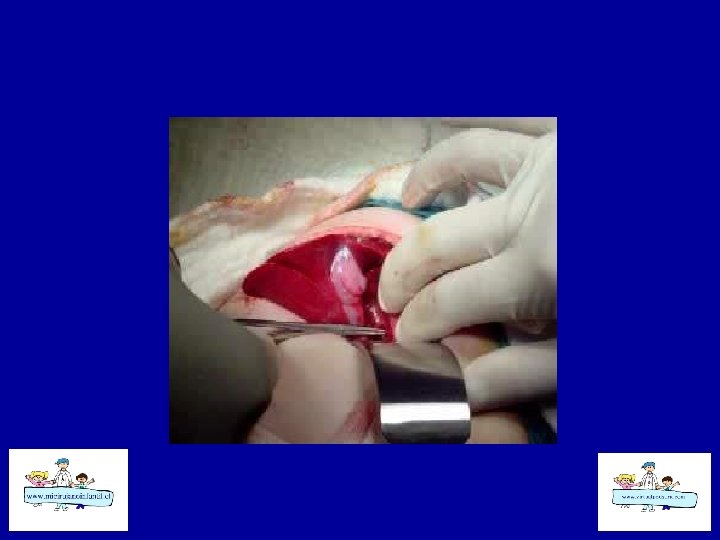
METODO DE EXTRACCIÓN • MOTILIDAD GASTROINTESTINAL (90 %) • ENDOSCOPIO FLEXIBLE O RIGIDO • SONDA FOLEY • EXTRACCION BAJO VISUALIZACIÓN DIRECTA CON PINZA MC-GILL • LAPAROTOMÍA C/ O S/ ENTEROTOMÍA
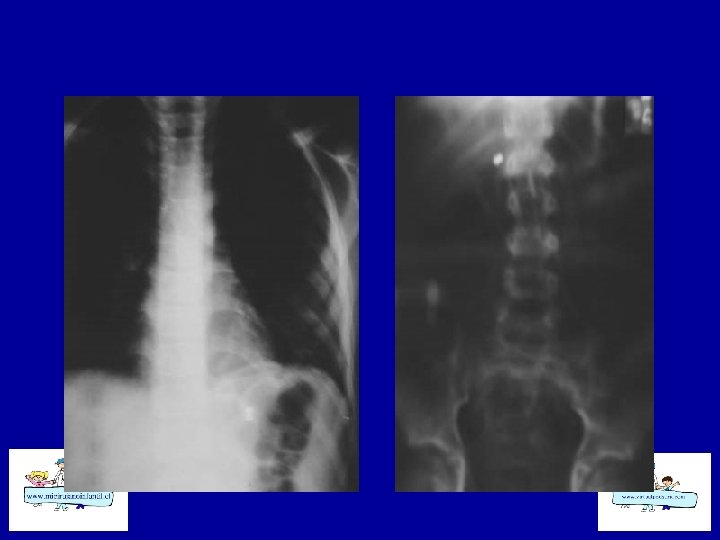
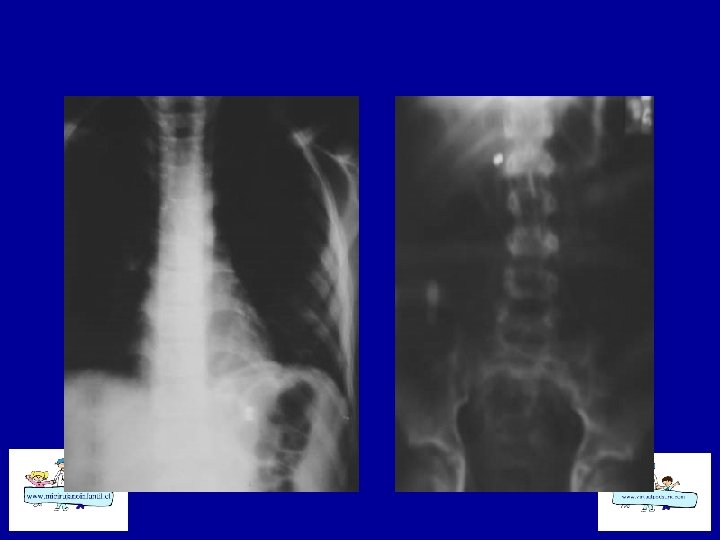
Estenosis Congénita del Esófago
Estenosis Congénita del esófago
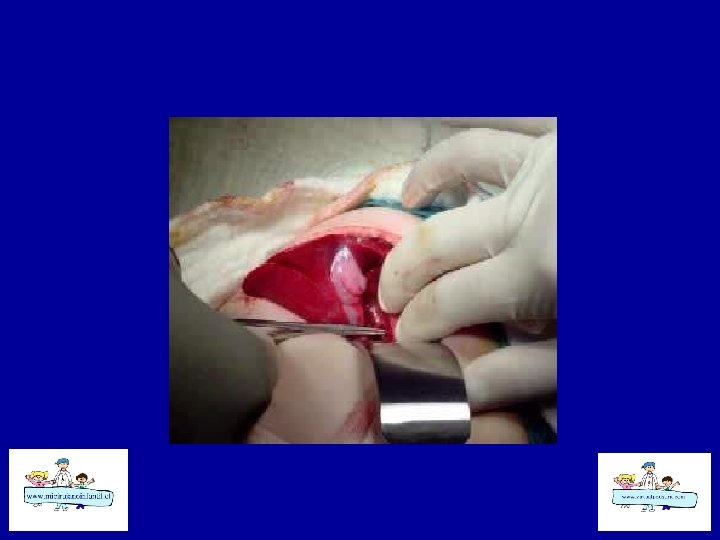
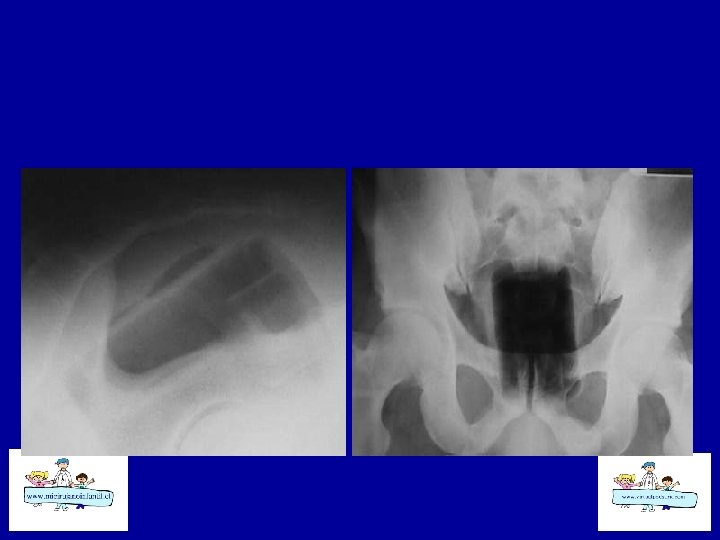
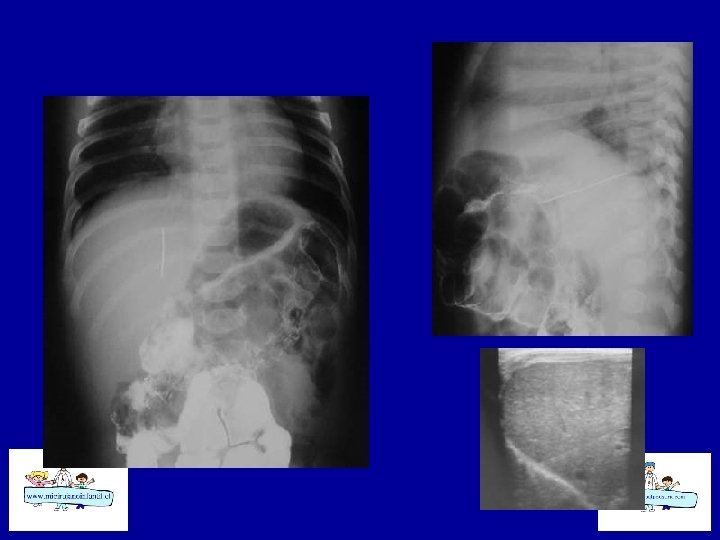
Tricobezoar Gástrico
Tricobezoar Gástrico
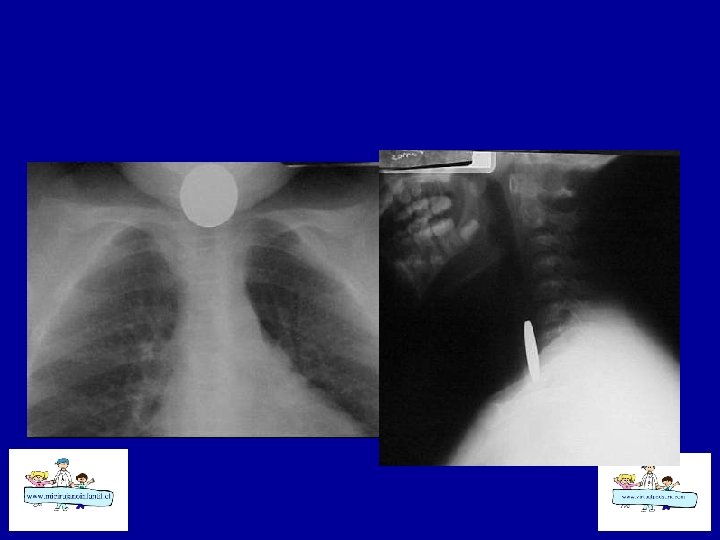
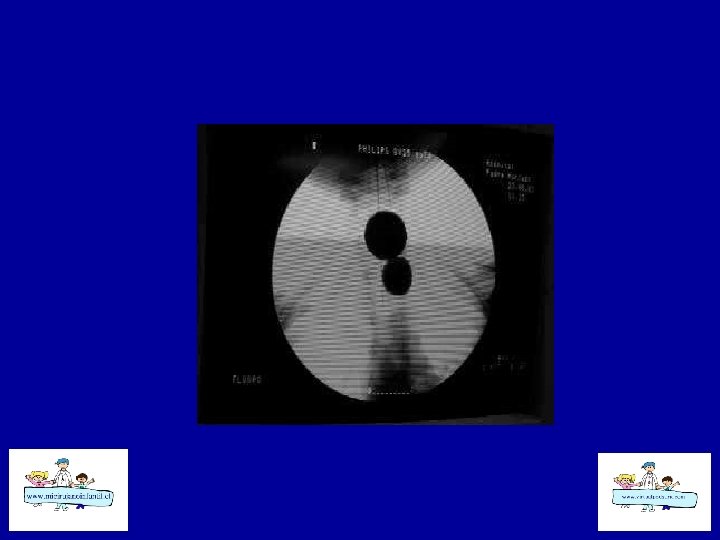
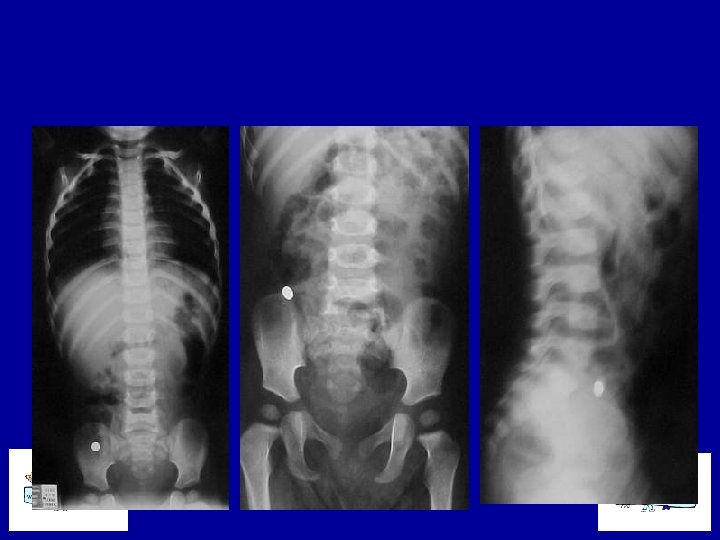
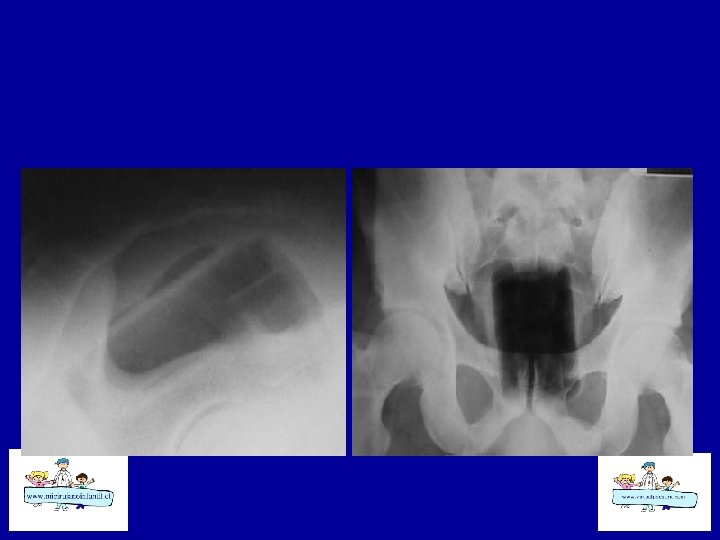
CUERPO EXTRAÑO DIGESTIVO PILAS TIPO BOTON • Generalmente son pequeñas, lisas, fáciles de tragar. • 90 % pasan sin problema • Se atascan en esófago si ø : 20 mm • Producen daño en 4 hrs y perforación en 6 -8 hrs.
CUERPO EXTRAÑO DIGESTIVO PILAS TIPO BOTON • Mecanismo de Daño 4 necrosis por presión 4 lesión directa por electrolitos 4 generación de corriente externa 4 toxicidad por Hg 4 Signos sugerentes de daño 4 edema * burbujeo esofágico 4 adherencia Litovitz
CUERPO EXTRAÑO DIGESTIVO CONTROVERSIAS • PILAS TIPO BOTON GASTRICAS 490 % migra libremente 4 Obs. por 48 hrs. en estómago 470% salen de estómago en 48 hrs. 4 En intestino : cirugía si permanecen en un mismo lugar 4¿Extraer las gástricas precozmente?
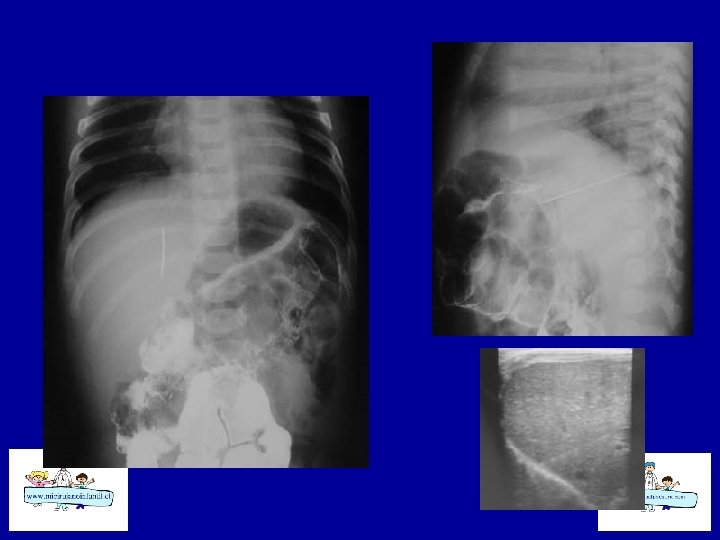
CONTROVERSIAS • OBJETOS PUNZANTES GASTRICOS 4 Representan el 10% de objetos ingeridos (ALFILERES DE GANCHO, MOLDADIENTES, AGUJAS, ETC). 4 Pueden presentarse con complicaciones. 4 Se reportan perforaciones
Cuerpo extraño digestivo
CUERPO EXTRAÑO DIGESTIVO EPIDEMIOLOGIA u. El 80% de los casos ocurre en niños. u. La ingestión es accidental casi siempre. u. Generalmente son únicos. u. Ocurre estando al cuidado de sus padres. u. El 90% se elimina espontáneamente.
EDAD DE PRESENTACION u. El niño inicia la prehensión voluntaria y visualmente guiada entre los 3 y 6 m. u. A los 9 m. es capaz de coger un objeto. u. INGESTION DE CUERPO EXTRAÑO ENTRE LOS 6 M Y 3 AÑOS u. El adolescente ingiere cuerpos extraños mientras desarrolla sus actividades habituales por descuido
EDAD DE PRESENTACION
CUERPO EXTRAÑO DIGESTIVO FORMA DE PRESENTACION • ANTECEDENTE ( +) • SIALORREA • DISFAGIA ( ) • SENSACION DE CPO EXTRAÑO • TEMOR • ASINTOMATICO • ANTECEDENTE (-) • DISFAGIA ( ) • VOMITOS • TOS –DISFONIA • PLENITUD • COMPLICACIONES
CUERPO EXTRAÑO DIGESTIVO UBICACIÓN DEL OBJETO • • • ESOF. SUP. ESOF. MEDIO ESOF INF ESTOMAGO DUODENO COLON
CUERPO EXTRAÑO DIGESTIVO METODO DIAGNOSTICO • ANAMNESIS • Rx SIMPLE: cuello, tórax y abdomen: siempre Ap y Lateral • Rx CONTRASTADA • ENDOSCOPÍA
CUERPO EXTRAÑO DIGESTIVO Patología Concomitante u ATRESIA ESOFAGICA OP. u R. G. E. RECIEN OP. u ESTENOSIS CONGÉNITA DEL ESOF. u OTRAS MALFORMACIONES DIGEST. u TRASTORNOS CONDUCTUALES
• OBJETOS • • • Moneda, Alfiler gancho, Alimentos Alfiler modista, Varios Metal Pila botón, Pilas, baterías Vegetal, Bolitas, vidrio Telas, latex, pelos
METODO DE EXTRACCIÓN • MOTILIDAD GASTROINTESTINAL (90 %) • ENDOSCOPIO FLEXIBLE O RIGIDO • SONDA FOLEY • EXTRACCION BAJO VISUALIZACIÓN DIRECTA CON PINZA MC-GILL • LAPAROTOMÍA C/ O S/ ENTEROTOMÍA
Estenosis Congénita del Esófago
Estenosis Congénita del esófago
Tricobezoar Gástrico
Tricobezoar Gástrico
CUERPO EXTRAÑO DIGESTIVO PILAS TIPO BOTON • Generalmente son pequeñas, lisas, fáciles de tragar. • 90 % pasan sin problema • Se atascan en esófago si ø : 20 mm • Producen daño en 4 hrs y perforación en 6 -8 hrs.
CUERPO EXTRAÑO DIGESTIVO PILAS TIPO BOTON • Mecanismo de Daño 4 necrosis por presión 4 lesión directa por electrolitos 4 generación de corriente externa 4 toxicidad por Hg 4 Signos sugerentes de daño 4 edema * burbujeo esofágico 4 adherencia Litovitz
CUERPO EXTRAÑO DIGESTIVO CONTROVERSIAS • PILAS TIPO BOTON GASTRICAS 490 % migra libremente 4 Obs. por 48 hrs. en estómago 470% salen de estómago en 48 hrs. 4 En intestino : cirugía si permanecen en un mismo lugar 4¿Extraer las gástricas precozmente?
CONTROVERSIAS • OBJETOS PUNZANTES GASTRICOS 4 Representan el 10% de objetos ingeridos (ALFILERES DE GANCHO, MOLDADIENTES, AGUJAS, ETC). 4 Pueden presentarse con complicaciones. 4 Se reportan perforaciones