CT Diagnosis of Small Bowel Obstruction Dr Sri
 Medistra Hospital")
CT Diagnosis of Small Bowel Obstruction Dr Sri Inggriani Sp Rad (K) Medistra Hospital Jakarta Konas XII Radiologi Makasar 20 -23 Nopember 2014

PROBLEMS • Based on evidence that some SBO resolve with conservative management and that the latest modalities of abdominal imaging allow confident diagnosis or exclusion of Small bowel Ischemia , early surgery is now performed more and more selectively • Therefore a full understanding of which imaging modalities to use , when to use and what imaging findings to look for to allow an individualized treatment approach is of very important

DEFINITIONS • Obstruction : is a mechanical blockage arising from a structural abnormality that presents a physical barrier to the progression of gut contents Obstruction is partial or complete simple or strangulated • Ileus : Is a paralytic or functional of variety obstruction • Accounts for 5% of all acute surgical admissions • Patients are often extremely ill , requiring prompt assessment, resuscitation and intensive monitoring

PATHOFYSIOLOGY § 8 L of isotonic fluid received by the small intestines (saliva, stomach, duodenum, pancreas and hepatobiliary ) § 2 L enter the large intestine and 200 ml excreted in the faeces § Air in the bowel results from swallowed air ( O 2 & N 2) and bacterial fermentation in the colon ( H 2, Methane & CO 2), 600 ml of flatus is released § Enteric bacteria consist of E. coli , anaerobes and strep. faecalis. § Normal intestinal mucosa has a significant immune role Distension results from gas and/ or fluid and can increase the hydrostatic pressure. Induced rapid Bacterial overgrowth. If mucosal barrier is breached it may result in translocation of bacteria and toxins resulting in septicemia.

PATHOFYSIOLOGY • Strangulation most commonly associated with adhesions when the distended bowel twists on its mesenteric pedicles-- arterial occlusion -- bowel ischemia and necrosis - peritonitis - death • Early detection of strangulation is important

What is the role of diagnostic imaging? You should be able to address the following questions : 1. 2. 3. 4. Is the small or large bowel obstructed ? What is the cause of this obstruction? How severe is this obstruction ? Is this a complex , strangulation present or simple obstruction ?

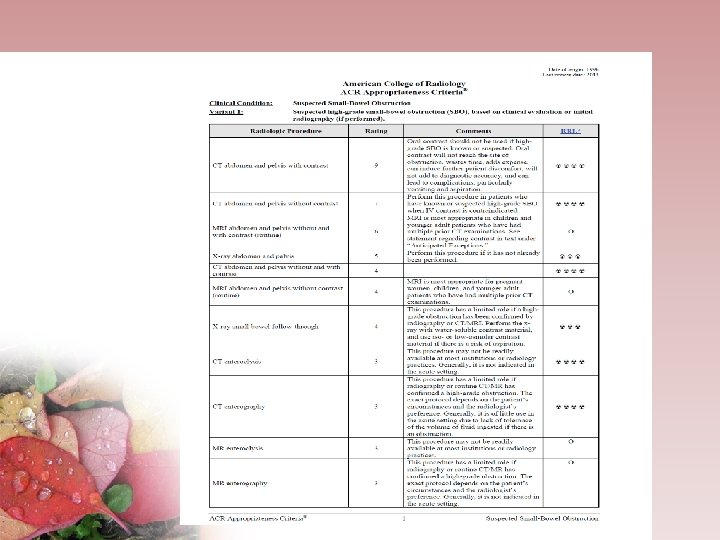
Different modalities to diagnose SBO • Plain abdomen : Diagnostic in 50 -60% of cases Equivocal in 20 -30% Normal / non spesific /misleading in 10 -20% • CT scan : In high grade SBO = sensitivity 82 %-100%. • CT had a capability for early demonstration of strangulation and now considered as the best modality for determining which patients would benefit from conservative management and close follow-up or is there a benefit from immediate surgical intervention.

Radiographics 2009 , 29 : 423 -439

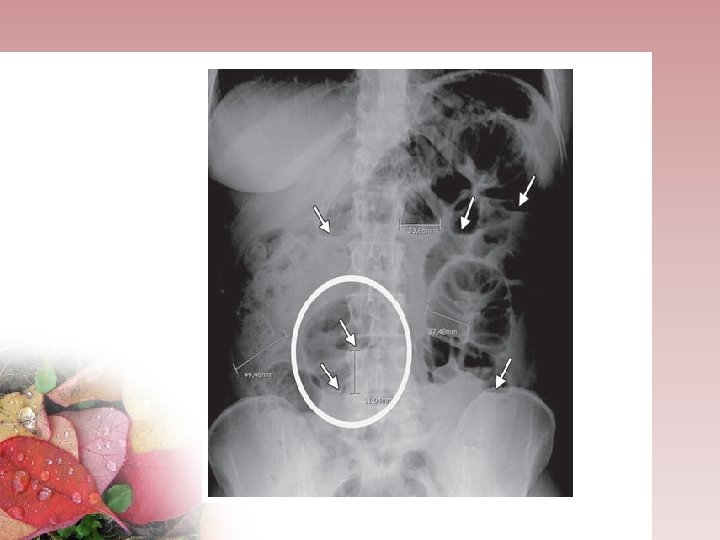
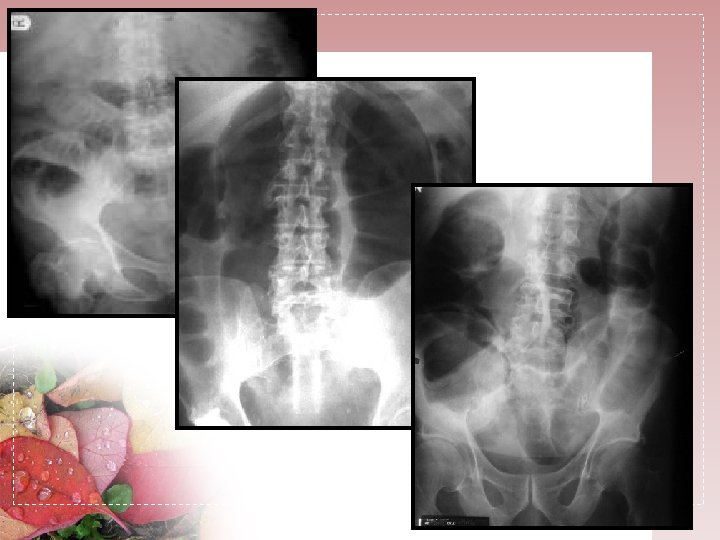
Plain Abdominal X-ray • At least 2 views ( supine or flat and upright or left lateral decubitus) • High grade SBO: presence of -> more than 2 ( two ) air-fluid levels, -> air-fluid levels wider than 2, 5 cm, -> air fluid levels differing more than 2 cm in height from one another within the small bowel loop. -> Small Bowel - Colon ratio > 0, 5

The Difference between small and large bowel obstruction Small Bowel • Central ( diameter 5 cm max) • Vulvulae conniventes Large bowel • Peripheral ( diameter max 8 cm ) • Presence of haustration
 Fluid Levels: Gastric")
Plain abdominal x-ray Plain film Always: Supine & Erect( diaphragm included) Fluid Levels: Gastric 1 -2 small bowel Check free gasses in 4 areas: Caecal Hepatobiliary Free gas under diaphragm Rectum Look for calcification Look for soft tissue masses, psoas shadow Look for fecal pattern

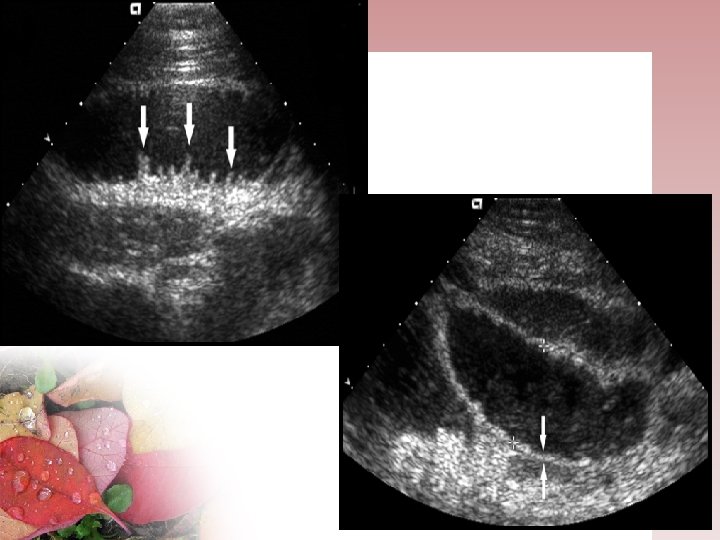
ULTRASONOGRAFY • Not commonly used in USA , it is frequently uses in many other countries , included Indonesia • Most of the time the bowel loops are filled with gas , cause non diagnostics sonogram • The fluid- filled bowel as a sonic window , could detect the level of obstruction. • The valvulae conniventes allows the obstruction to be localized to the small bowel • The peristalsis in the dilated segment is increased • The severity of the obstruction can also be assessed • The presence of free fluid is easily to detect • non radiating 90 % success rate in diagnosing intussusception or volvulus for pediatric patient • Operator dependent technique

CT SCAN • CT have great capability for early demonstration of strangulation. • CT is now considered the best modality for determining which patients would benefit from conservative management and close follow-up and which patients would benefit from immediate surgical intervention. Sensitivity and specificity = 92 % resp 71 %

CT scan Used always IV contrast (check for renal insuff , allergy etc ? ) Oral contrast , are not absolutely necessary (the retained intraluminal fluid serves as a natural contrast agent. ) Rectal contrast media is indicated Scrolling the CT data in a cine mode by acquiring thin section CT data in multiplanar sections , to look the transition point !! The answer of the cause of the obstruction is almost always in the transition point ( the mural thickening, the extraintestinal causes and the endoluminal causes /foreign objects )

CT scan • Is Small bowel obstructed ? CT CRITERIA 1. Diameter of small bowel loop is >2, 5 cm IN THE DILATED PROXIMAL (from outer wall to outer wall) to a COLLAPSED bowel loops distally or High grade SBO : > 50% difference in caliber between the proximal dilated bowel and the distal collapsed bowel. 2. . Small Bowel to Colon ratio > 0, 5 3. Small bowel feces sign , in low-grade subacute obstruction , rather to identify the transition point 4. A smooth beak indicates simple obstruction without vascular compromise. 5. Bowel wall thickening , porta venous gas , pneumatosis indicates early strangulation 6. No passage of contrast medium beyond the point of obstruction

CT scan Where is the Transition point ? • Scroll the CT image data in multiplanar images begin in a retrograde fashion by starting at the rectum and proceeding proximally toward the cecum, ileum and jejunum. • If the transition point is located proximal (jejunum or duodenum ) do the scrolling in antegrade approach starting at the stomach. • Always look for the presence of the small bowel feces sign , when present , it is usually present at the transition point

Causes of Small Bowel Obstruction

Cause of Large Bowel Obstruction Etiology: 1. Carcinoma: is the commonest cause, 18% of colonic ca. 2. Benign stricture: due to Diverticular disease, Ischemia, Inflammatory bowel disease. 3. Volvulus: Sigmoid Volvulus: results from long redundant, faecaly loaded colon with a narrow pedicle Caecal Volvulus 4. Hernia. 5. Congenital : Hirschsprung, anal stenosis and agenesis

Intrinsic cause of SBO Small bowel neoplasm Colonic neoplasm

Lymphoma Peritoneal mets from colon Ca

Perforated gallstone Rigler´s Triad: Small bowel obstruction Aerobilia Ectopic gall stone

In adults: > 90% lead point: tumor: lipoma, mets, hamartoma, carcinoid • 5% idiopathic Intussusception

Intramural hematoma due to anticoagulant therapy

Trombosis AMS/ VMS

EXTRINSIC CAUSE • Adhesions: ranging from 50%-80% of all cases , almost all of them are post operative Adhesive bands are not seen at conventional CT , only as an “abrupt changes “ in the caliber of the bowel is seen without any associated mass lesion Is the SBO simple or complicated ? Is the SBO simple or closed-loop obstructions ?

EXTRINSIC CAUSE Simple obstructions : when the bowel is occluded at one or several points along its course. Closed –loop obstructions : when a bowel loop of variable length is occluded at two adjacent point U shaped or C –shaped dilated small bowel Streched and prominent mesenteric vessels converging toward the point of torsion “beak sign “ at the site of torsion “whirl sign “ reflecting rotation of the bowel loops around the fixed point of obstruction cause a small bowel volvulus

EXTRINSIC CAUSE • Strangulation : • is a closed-loop obstruction associated with intestinal ischemia • 10 % of SBO -> need surgical treatment • Signs: • Thickened bowel wall Absent /asymmetric enhancement or delayed enhancement of bowel wall Increased attenuation of bowel wall on non contrast scan Gas in the portal vein and or in mesentery vein Halo / target sign Whirl sign , a twisting of mesenteric vasculature Pneumatosis intestinalis Hemorrhage in the mesentery Ascites

Small bowel adhesion

Simple adhesion

SBO due to postoperative adhesion

Multiple intrabdominal abcesses after appendectomi

Peritonitis TBC usus

Ischemic Strangulation bowel

Closed loop SBO -Intestinal volvulus

Hernia • Classified according to the anatomic location of the orrifice through which bowel protrudes • As the 2 nd common cause of SBO • Protruded small bowels in a abdominal or pelvic wall defect due to congenital weakness or previous surgery • The diagnosis is almost clinical
 : occur lateral to •")
External hernia : • 1. Inguinal hernia (most common) : occur lateral to • Indirect type • Direct type (less frequent ) , found medial to the inferior epigastric vesels the inferior epigastric vessels , observed in male children when the peritoneal extension accompanying the testis during embryonic development is not obliterated completely and can form in adults owing to weakness and dilatation of the inguinal canal. • 2. Femoral hernia (more in females patient, medial to the femoral veins ) • 3. Obturator hernia : uncommon , hernia in the obturator canal • (90% ) in older women due to enlargement of the canal after pregnancy

• 4. Ventral hernia : located in the anterior and lateral abdominal wall • 5. Umbilical hernia , most common type tend to be in woman • 6. Paraumbilical , epigastric and hypogastric hernia , below the umbilicus • 7. Spigelian / lumbar / incisional /parastomal hernia

Incarcerated Strangulated External Hernia

Strangulated Inguinal hernia

Internal Hernia : • • The responsible hernia orifices are usually pre existing anatomic structures such as foramina and fossa The pathological defects of the mesentery and visceral peritoneum which are caused by congenital mechanism , surgery and trauma are potential as herniation orifices. The diagnosis is difficult Less common • Type: • • • 1. Para duodenal = PD ( 53 %), most common 2. Peri Cecal ( 13 %) 3. Foramen Winslowi ( 8%) 4. Transmesenteric ( 8%) 5. Sigmoid mesocolon ( 6 %) 6. Retro anastomotic ( 5 %) • Internal hernia are silent, and the majority cause epigastric pain • and recurent. • A delay in diagnosis may lead to strangulation

• CT finding: • An abnormal cluster or sac like mass of small bowel loops at an abnormal anatomic location and the observation of engorged and converging vessels at the hernial orifice. • 1. Paraduodenal hernia , the most common type , a. Left PD hernia : >75% , develop through the fossa of Landzert at the duodenojejunal junction. CT : abnormal clustered of sac like mass of small bowel loops lying between stomach and pancreas. b. Right PD hernia: involve the fossa of Waldeyer , located behind the SMA and IMA to the transverse portion of the duodenal loop • •

• 2. Transmesenteric hernia : mostly due a defect of mesentery in the region of ligament of Treitz or Ilieo cecal valve • 3. Foramen of Winslow hernia : a comunication foramen between the lesser and greater sac ( located anterior to the IVC and posterior to the hepatoduodenal ligament ). The terminal ileum, cecum and Asc colon are involved
 shows the locations and directions of internal hernias")
Classification of Welch Drawing (coronal view) shows the locations and directions of internal hernias of the upper and lower abdominal peritoneal cavity. A foramen of Winslow hernia, B left paraduodenal hernia, C right paraduodenal hernia, D transmesenteric hernia, E pericecal hernia, F transomental hernia, G intersigmoid hernia.
 shows the locations of internal hernias, pouches, and fossae of the")
Drawing (superior view) shows the locations of internal hernias, pouches, and fossae of the pelvic cavity in a female patient. H supravesical hernia, I Hernia through the broad ligament, 1 Vesicouterine pouch, 2 Douglas (rectouterine) pouch, 3 Perirectal fossa.

Internal hernia Foramen Winslowi

Colon Descendens neoplasm

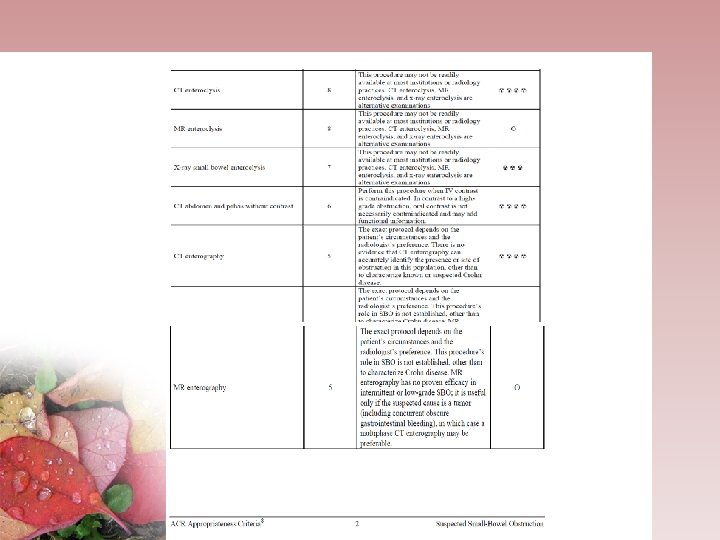
CT ENTEROCLYSIS Improved sensitivity and spesificity over standard barium SB studies and CT in evaluating of suspected intermittent of low grade SBO Could be considered as an alternative exam in patient with history of malignancy Low patient acceptance Depends on the skill of the radiologist

MRI • MRI also utilizes intraluminal air as a natural contrast agent • MR enteroclysis is comparable with CT enteroclysis • Using no radiation ( especially for pregnancy and childrens ) • Longer scanning time, need cooperative patient. • Lower availability, not widely used
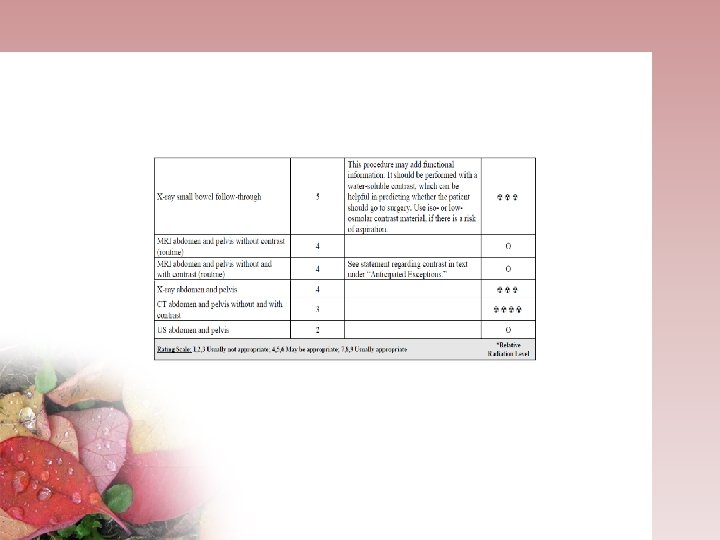

SUMMARY MSCT has emerged as the imaging modality for evaluating SBO and should be considered in the initial evaluation of patients with suspected SBO. The barium enema and small bowel examination play a less significant role and should not be used as a primary modality in diagnosing acute SBO If intermittent of low-grade SBO is a diagnostic concern, either CT or MR enteroclysis is prefered. • We could depict the following questions: Is the SB obstructed? How severe ? Where is it located , what is the cause , is strangulation present ?

SUMMARY • CT is the best modality to help distinguished the conservative management or immediate surgical intervention. Do a retro grade cine evaluation on CT to locate the transition point. The answer of the cause of the obstruction is always in the region of the transition point (mural thickening, endoluminal causes ? )

- Slides: 57