CSOM ATTICO ANTRAL DISEASE DR MUBEENA 1 CHOLESTEATOMA

+ CSOM ATTICO ANTRAL DISEASE DR MUBEENA 1

+ CHOLESTEATOMA

+ n. The presence of stratified squamous epithelium in the middle ear or mastoid. n. Skin in the wrong place.

+ Misnomer ? n “Cholesteatoma" coined by the German physiologist Johannes Müller in 1838, is a misnomer because this entity does not contain cholesterol n the white-yellow keratin flakes found within cholesteatomas grossly resemble cholesterol crystals n ‘oma’ is a suffix for tumour 4

+ SYNONYMS: 1. KERATOMA 2. EPIDERMOSIS 3. CHOLESTEATOSIS

+ n Choleasteatoma consists of : q. PERIMATRIX – stroma of connective tissue q. MATRIX – keratinising squamous epithelium resting on thin stroma of fibrous tissues. q. KERATIN DEBRIS – central white mass produced by the matrix

+ Cholesteatoma has the capacity for progressive and independent growth at the expense of underlying bone and has a tendency to recur after removal. ”

+ CLASSIFICATION: 1. CONGENITAL 2. ACQUIRED- primary acquired secondary acquired

+ CONGENITAL CHOLESTEATOMA 6/11/2563 9

+ Pathogenesis n Congenital n Arise cells from embryonal rests of epithelial n COMMON SITES- middle ear – ASQ commonest site mastoid cerbellopontine angle petrous apex

+ 11 CONGENITAL CHOLESTEATOMAS n. Most involve the anterior superior quadrant of the middle ear 6/11/2563

+ n Clinical symptoms n Conductive hearing loss. n Otalgia n Vertigo or SNHL if labyrinth is invaded. IMAGING HRCT CT Scan – confirm location and size

+ LEVENSON’S CRITERIA n White mass behind the normal ear drum n • Normal pars flaccida and pars tensa n • No prior history of perforation / Otorrhoea n • No previous otological procedures

+ High Resolution Computed Tomography

+ 15 Surgical management of a congenital cholesteatoma n complete removal of the cholesteatoma matrix n The isolated middle ear cholesteatoma n removed transtympanically n Routine middle ear reconstructive techniques may be used if ossicles are eroded or removed or if the tympanic membrane is sacrificed. 6/11/2563

+ ACQUIRED CHOLESTEATOMA 6/11/2563 16
")
+ 17 The pathogenesis of acquired cholesteatoma There are four basic theories : (1) Invagination of the tympanic membrane (retraction pocket cholesteatoma) (2) basal cell hyperplasia (3) epithelial ingrowth through a perforation (the migration theory) (4)squamous metaplasia of middle ear epithelium 6/11/2563

+ Invagination theory. Wittmack 1939 Eustachian tube dysfunction -negative ME pressure -pars flaccida retraction -squamous debris collected in the sac

+2. Epithelial invasion theory: Haberman 1889: keratinising squamous epithelium from the surface of the TM or meatus invades into the middle ear from perforation in TM.

+ 3. Basal n cell hyperplasia theory: Reudi’s theory The basal cells of germinal layer of skin proliferate under the influence of infection and lay down keratinising squamous epithelium

+ 4. Squamous metaplasia theory: Wendt 1873: Simple cuboidal epithelium of ME cleft could undergo metaplastic transformation into keratinising epithelium because of repeated infection.

+ PRIMARY AQUIRED CHOLESTEATOMA

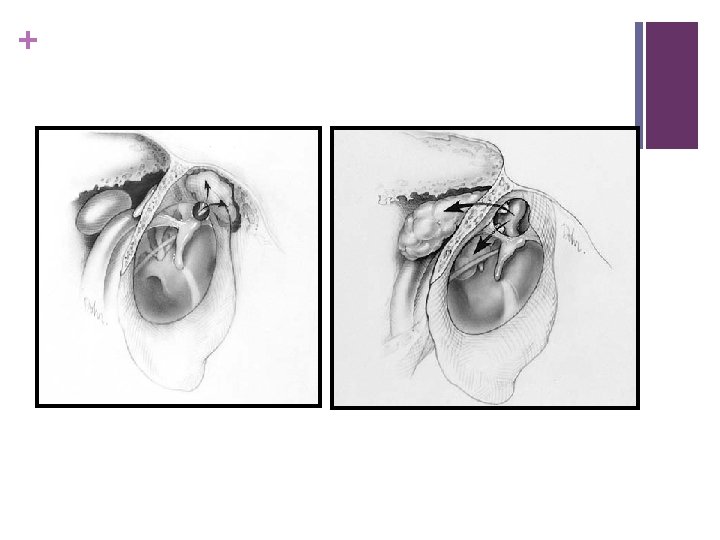
Primary acquired cholesteatoma + n Called primary as there is no history of previous perforation n Secondary to ET dysfunction n Retraction pocket choleasteatoma in Pars flaccida or PSQ retraction pocket n Invagination n Keratin pocket theory is most accepted debris collects in the retraction

+ Primary acquired cholesteatoma Normal TM Mesotympanic cholesteatoma primary acquired cholesteatoma

+ Primary acquired cholesteatoma

+ WHY ATTIC AND PSQ IS PREDISPOSED FOR RETRACTION ? n There a fewer connective tissue fibres within the lamina propria (middle layer of TM) as compared to pars tensa n Normal migratory pattern of TM epithelium changes within retraction pocket. This results in keratin formation and choleasteatoma n PSQ – weakest quadrant of the pars tensa

+ SECONDARY AQUIRED CHOLESTEATOMA

+ Secondary Acquired Cholesteatoma n Migration Theory – most accepted n Originates from a tympanic membrane perforation n As the edges of the TM try to heal, the squamous epithelium migrates into the middle ear

+ Microbiology: - Pseudomonas Proteus Mixed aerobic and anaerobic organisms

+Behaviour of choleasteatoma BONE RESORPTION n Pressure necrosis theory- unlikely n Enzymatic : theory by cytokine mediated inflammation Inflammation alpha Release IL-1, IL-6, IL-11, TGF- cause osteoclast activation Acid phosphatase, collagenase, acid proteases, cathepsin like proteolytic enzyme, matrix metalloproteases

+ 31 n bone erosion n Ossicles : most long process of incus n Bony labyrinth n facial nerve canal n tegmen tympani n Sinus plate 6/11/2563

+ ATTICOANTRAL TYPE n It involves POSTERIOR SUPERIOR part of the middle ear cleft (attic, antrum , posterior tympanum and mastoid)

+ Tubotympanic or safe type Atticoantral or unsafe type Discharge Intermittent , Profuse , mucoid , odourless , not blood stained Continuous , Scanty , purulent , foul smelling , and occasionally blood stained Perforation Central Attic or marginal Granulations Uncommon Common Polyp Pale Red and fleshy Choleasteatoma ABSENT PRESENT Complications rare common Audiogram Mild to moderate conductive Conductive or mixed deafness

+ PATHOLOGY n Cholesteatoma n Osteitis and granulation tissue n Ossicular necrosis n Cholesterol granuloma

+ Osteitis and granulation tissue

+ OSSICULAR NECROSIS n LONG PROCESS OF INCUS n Hearing loss more than TTD n Cholesteatoma hearers

+ CHOLESTEROL GRANULOMA n Granulation tissue with foreign body giant cells surrounding cholesterol crystals n Reaction to longstanding retention of secretion or haemorrhage

+ Symptoms n Ear discharge n Impaired n Tinnitus n Vertigo hearing- cholesteatoma hearer

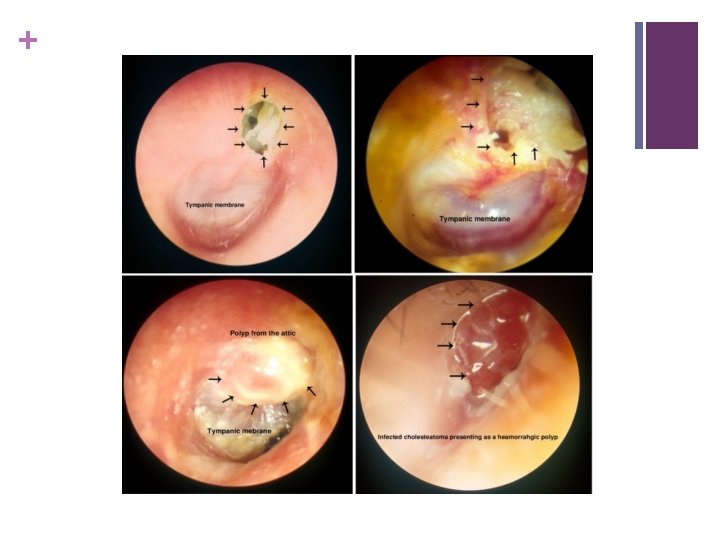
+ Signs n Retraction pocket in early stage n Characteristic n ‘Fishy n Attic/ discharge odor of cholesteatoma marginal or total perforation n Cholesteatoma seen as n Pearly white sac through translucent TM or as n Pearly white flakes of epithelium through mouth of the sac, or as n In-growing skin though perforation

+ Retraction pocket

+ MARGINAL PERFORATION

+ Primary acquired cholesteatoma

+ Other signs n Granulation tissue in the attic/ posterosuperior quadrant n Attic crust n Vascular n Attic polyp widening

+ Evaluation n Examination under microscope n Cultures should be obtained in infected ears � X RAY mastoid – extent of bone destruction Cholesteatoma- sclerosis with cavity. � Pure tone audiometry � HIGH RESOLUTION CT SCAN OF TEMPORAL BONE

+ Evaluation 1. Examination under microscope n Retraction pocket n Choleasteatoma- suction clearance and examination n Granulation from diseased bone n Aural polyps n Ossicles

+ Evaluation n. PURE TONE AUDIOMETRY – usually conductive loss, may vary greatly; confirm with tuning forks q pre-operative assessment q degree of hearing loss q. Type of hearing loss

+ Audiogram

+ Computed Tomography n Erosion of scutum n Destruction n Erosion n Low of ossicular chain of the labyrinth (fistula) tegmen / tegmen defect n Facial nerve dehiscence n Petrous Apex Involvement

+ Computed Tomography

+ Computed Tomography

+ Features indicating complications n Pain n Vertigo n Persistent headache n Facial weakness n Fever, nausea, vomiting n Irritability, neck rigidity n Diplopia n Ataxia n Abscess around the ear

- Slides: 54