CRT 2020 Washington DC USA Feb 22 25

CRT 2020 Washington, DC, USA, Feb 22 -25, 2020 Vertebral stenting Step by step for the beginner Horst Sievert (FAAC, FESC, FSCAI) Kolja Sievert, Ilona Hofmann, Sameer Gafoor, Stefan Bertog, Predrag Matić, Markus Reinartz, Bojan Jovanovic, Shahrak Zaker, Iris Grunwald, Nalan Schnelle, Robert Andel, Anja Vogel, Pamela Ilioska, Kai Ruffmann, Gerhard Sell Cardio. Vascular Center Frankfurt - CVC, Frankfurt, Germany

Horst. Sievert. MD@aol. com

Vertebral Stenosis • Almost always at the origin • Natural history - is good if asymptomatic (although we do not have good data) - 10 -20% stroke rate per year if symptomatic • Risk of hemodynamic ischemic stroke only in case of contralateral stenosis, occlusion or hypoplasia

Anatomical variations • Left vertebral from the aortic arch 2 -4% - Between left CCA and subclavian • Right vertebral from the right CCA or the aortic arch • Vertebral fails to join the basilar artery 0. 5% 0. 2%

Step by step • • • Pre-treatment with aspirin and plavix No sedation Access femoral, radial or brachial Heparin 5, 000 (or ACT > 250 s) Embolic protection ? - Distal filter - Proximal occlusion (subclavian artery)

Balloon angioplasty only? • Not recommended because - residual stenosis is common - spasm may occur - dissection may occur and extend distally - high re-stenosis rate • Always stent!

DES or BMS? • No randomized trials • Results of non- randomized trials are conflicting - One large non-randomized trial 1 did not show a difference • Re-stenosis rate DES vs BMS 22. 8% vs 19. 4% - Another study 2 showed a significant benefit • TVR DES vs BMS 6. 3% vs. 20. 2% 1 Maciejewski D, Advances in Interventional Cardiology, 2019 2 Lipo Song, et al. J of Endovascular Therapy: April 2012, Vol. 19, No. 2, 231 -238.
 and/or 6 F long")
Step by step • 6 F guiding catheter (FR 4) and/or 6 F long sheath • Cranial angulation for visualization of the vertebral ostium • Do not touch the ostium! - buddy wire in the subclavian artery to stabilize the guiding catheter • • • 0. 014" coronary wire for lesion crossing Predilatation rarely needed Balloon expandable stents for ostial lesions Self expanding stents for distal lesions Avoid stent protrusion into the subclavian artery - Re-stenosis is frequent and crossing the stent may be difficult

J. R. , m. , 79 y. • Feb 2019: - Basilar stroke - i. v. lysis - Angiography showed basilar artery stenosis • no intervention performed • June 2019: - Basilar artery stenosis resolved Left internal carotid artery 60% Ostial stenosis of the right vertebral artery, PSV 3 m/s Left vertebral does not join the basilar artery • Stroke assumed to be embolic from the right vertebral artery stenosis • Referred for right vertebral artery stenting

Left vertebral artery did not reach the basilar artery

Ostial stenosis of the right vertebral artery Does not look very tight but PSV was 3 m/s

No relevant basilar artery stenosis

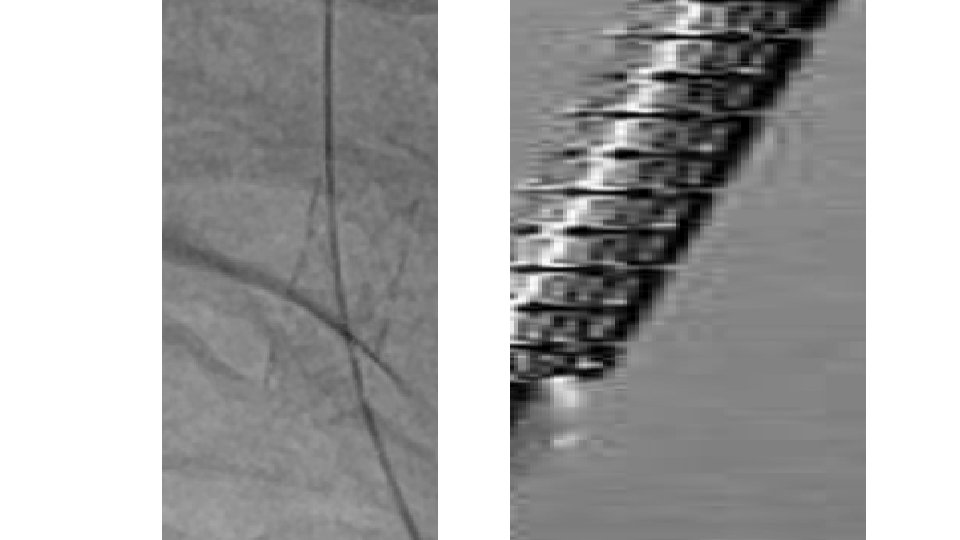
AP, 15° cranial Ostial stenosis of the right vertebral artery 6 F FR-4 guide Movement of the catheter due to heart beats and respiration 0. 035" buddy wire in the subclavian artery Guiding catheter not touching the ostium

How to place the stent exactly at the ostium with all that movement?

Additional 0. 014" wire through the proximal stent strut

3. 5 mm/8 mm DES Additional 0. 014" wire through the proximal stent strut

Thank you for your time! – Time is brain! Horst. Sievert. MD@aol. com
- Slides: 18