CRT 2016 Endovascular Intervention of Aortoiliac Bifurcation Disease

CRT 2016 Endovascular Intervention of Aorto-iliac Bifurcation Disease Vinay Kumar MD, FACS, ABVM President, Endovascular options Dallas, Texas

Disclaimer • Nothing to Disclose.

AOI Disease • Most misunderstood process – Often difficult to diagnose by referring physician due to overlap of symptoms – High thigh and buttock claudication is often misinterpreted as OA disease • 30 -40% patients are young, often females, presenting as CLI : Toe ulcers, painful spots on toes

AIOD or “Leriche syndrome” • • Disease was first described by Rene Leriche in early 1900 Present as “Leriche triad” – Classically, it is described in male patients as a triad of symptoms consisting of: – Claudication of the buttocks and thighs – atrophy of the musculature of the legs – Impotence (due to paralysis of L 1 nerve) Surgicalthe therapy with Aorto iliac/ Aorto femoral bypass or Endarterectomy is standard of therapy Axillo –femoral bypass in High risk patients
 Balloon Angioplasty")
AIOD : Endovascular Approach • Endovascular Therapy : SOC (standard of care) Balloon Angioplasty Balloon angioplasty with Stent placement Bx Stents Sx Stents Covered Stents Bx/ Sx Atherectomy DES DEB

TASC Classification • Simple Form • Type A • Type B • Complex form : C and D lesions • Bilateral severe ostial disease of iliac arteries with calcification • CTO • Unilateral /bilateral common iliac artery • Unilateral /bilateral ext iliac artery • Combination of the two • Aorto-iliac disease • Aortic stenosis or occlusion

Treatment Considerations 1. Procedure should be individualized based on patient and anatomy 2. Need to know when to stop 3. Need to be aware of perforation or RUPTURE “FATAL” Remember Some surgical procedure also very simple 1. Fem-fem Cross over graft 2. Axillo- femoral bypass

Challenges of AI intervention • Severe calcified lesions -Specially females with small vessels • Complications: Embolization, Perforation, Rupture Thrombosis • Difficulty regaining access to the true lumen in TASC C and D • Restenosis • re-occlusion

Techniques Treatment process Approach Crossing the lesion Treatment 1. Femoral : uni/Bil, SFA 2. Brachial/Axillary/Radial 3. combined 1. Guide wire 2. CTO Devices 3. Re-entry Devices 1. Balloon Angioplasty 2. Bare metal stent : Bx or Sx 3. Covered stents : Bx or Sx 4. DEB/Stent

CTO tools • • • Front Runner Crosser catheter Wildcat Ocelot True path Viance

Reentry tools Basis 1. Enter the false lumen 2. Reenter true lumen by a needle. 1. Blindly 2. Vision : Ivus or U/s Pioneer catheter Off Road Stingray

Techniques of Aorto- iliac reconstruction • Depend upon location of disease – Aorta alone – Iliacs alone – Aorto- iliac • Double Barrel • V : Reverse V – Kissing technique • Top head and V

AOI reconstruction : Complicated procedures • Knowledge – – Wires Catheters CTO and Re entry devices Stent • Location and how to • Types of stent appropriate for location • Proficiency – Approaches – Femoral – Brachial/ Axillary/Radial • Combined App – SFA approach – Hybrid • Direct surgical with Endovascular

AOI Reconstruction : Double Barrel • Reconstruction is done with Two Stents placed from bilateral femoral approach • SX or BX stents can be placed • Aim is raise the aortic bifurcation • Keep stent approximately 5 - 10 mm in Aorta Double Barrel

Double Barrel with BX Palmaz stent

Double Barrel • Durability also depends upon the type of stent • Covered stents tend to perform better in our experience

Long-term results of double-balloon percutaneous transluminal angioplasty of the aorta and iliac arteries. Insall RL, Loose HW, Chamberlain J. Eur J Vasc Surg. 1993 Jan; 7(1): 31 -6 • • Seventy-nine patients with AOI disease within 0. 5 cm of the aortic bifurcation. Seven patients had repeated angioplasties, a total of 86 procedures over an 8 year period up to December 1990. Average follow-up of 49 months (median 51 months, range 7 -93), only six patients (7%) developed late recurrence of symptoms requiring further treatment. The cumulative success rate beyond 5 years' follow-up was 80%. Complications requiring surgical intervention occurred in four patients (5%). Double-balloon percutaneous transluminal angioplasty was seen to be an effective procedure which produced lasting improvement and is recommended as the first choice treatment for localized stenotic and occlusive disease at the aortic bifurcation

Double Barrel • Advantage – Simple – Easy to position stents – Good short term durability – Questionable long term durability • Disadvantage – Inability to perform over the horn intervention for lower extremity : Femoral approach

AOI reconstruction : V or Kissing Technique Reverse V, or Kissing • Similar to double Barrel • Stents are placed at the origin of iliac arteries • Can be done with Bx or Sx stent • Bx preferred due to better Hoop Strength

V technique • Advantages – Precise stent placement W/o overlap in aorta – Future cross over interventions • Disadvantages – Aortic bifurcation may be misleading – Kissing stent may not be perfect reverse V – Lead to re occlusion

Kissing stents

Aortic disease progression in future may need further intervention

Percutaneous reconstruction of the Aorto-iliac bifurcation with the "kissing stents" technique: long-term follow-up in 106 patients. Haulon S, Mounier-Véhier C, Gaxotte V, Koussa M, Lions C, Haouari BA, Beregi JP. , J Endovasc Therapy 2002 • • • One hundred six patients (97 men; mean age 52. 5 +/- 10. 2 years, range 3378) were treated with the kissing stents technique for bilateral aortoiliac stenosis (55, 51. 9%), unilateral occlusion of the common iliac artery (CIA) with contralateral stenosis (47, 44. 3%), and bilateral CIA occlusion (4, 3. 8%). Clinical examination and duplex scans were performed prior to discharge and at 1, 6, and 12 months, followed by yearly examinations thereafter. Primary and secondary cumulative patency rates at 36 months were 79. 4% and 97. 7%, respectively. Balloon-expandable stents had a non-significantly higher patency rate compared to self-expanding stents. • CONCLUSIONS: Based on our experience, aortoiliac endovascular reconstruction with the kissing stents technique is a safe and effective procedure, representing an alternative to conventional surgery in selected patients.

Top head and V Aortic stent Important to place iliac stent inside aortic stent, to prevent development of stenosis between stents Iliac stents creating reverse V BX SX Covered stent All can be used for reconstruction

Top head and V : With Wall stents 1993 • Aortic stent – 20 x 50 Wallstent • Two iliac stents – 7 Years later 8 x 40 Wallstent Post BA

Case 1 40 yr old smoker female Exam : • Non palpable DP and PT • Non palpable femoral pulsations • Doppler on femoral : + • Bil femoral bruits • Weak Doppler signals Dp/PT Resting ABI 0. 6 After exercise 0. 4

U/S Guided bilateral femoral access Brachial artery L prepared for puncture

Top head and V reconstruction with, three BX stents Palpable DP/PT No foot pain Discoloration reversed At 2 yr Follow up 10 x 40 Genesis, post dilated to 14 mm 6 x 40 Bx stents in iliac arteries Patient stopped smoking Remains asymptomatic Walking 1. 5 miles every day

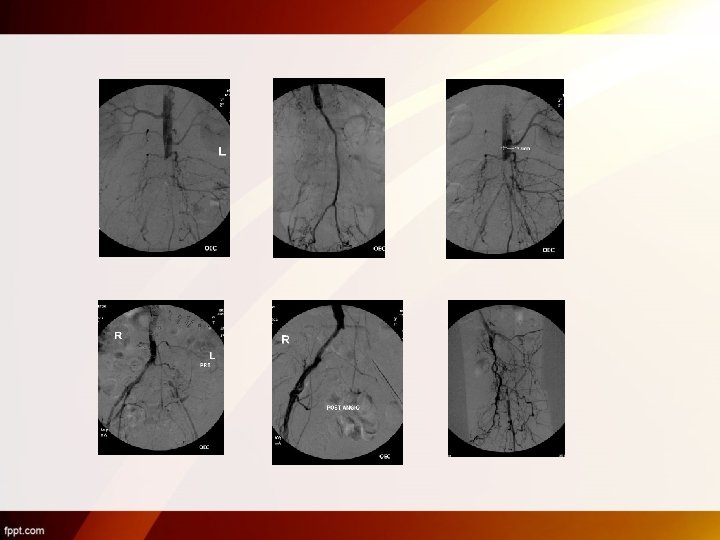
Case 2 : Combined Approach, Brachial and Bil femoral : Reverse V with Covered stents 54 yr old obese black female with DM, HTN Bil thigh and hip pain No foot pain Treated for OA Both wires went Subintimal in Aorta Bilateral reentry was done with Outback catheter

Two outback devices placed simultaneously Looped glidewire 1 2 8 x 59 i. Cast Covered stents x 2

Case 3 69 Yr old male SFA puncture


Final Result

Direct surgical approach • High Bifurcation • Small Caliber SFA – Ideal for direct exposure – Sheath entery site can closed with a vascular suture

Complications Perforation

Complications Thrombus

• Post surgical thrombectomy

Conclusion • Aorto iliac Occlusive disease is ideally suited for endovascular therapy. • May be treated with Variety of techniques including, double Barrel, V and High top and V • Chronic occlusions are prone to multiple complications and therapeutic issues, extreme care is warrented • It is important to individualize the procedure to prevent interventional nightmares

• Thank you
- Slides: 40