CRT 2013 Washington DC February 23 26 th

CRT 2013 , Washington DC February 23 -26 th, 2013 Cath Lab Catastrophes : Prevention & Management Strategies Fayaz Shawl, M. D. , F. A. C. C. Director Interventional Cardiology Washington Adventist Hospital - Takoma Park, Maryland Clinical Professor of Medicine George Washington University - Washington, D. C.
 Medtronic Abbot")
Fayaz Shawl, MD Research Support : Boston Scientific Cordis ( J&J ) Medtronic Abbot
")
Cath Lab Catastrophes Crash bypass Urgent bypass P value Results: OR mortality 6/19 (32%) 1/56 (2%) 0. 0001* Hospital stay 8. 06(8. 04) 11. 57(8. 86) 0. 1420 3/56 (5%) 0. 0001 * In-hospital mortality 9/19 (47%) JA Carey, et al, Br Heart J 1994; 72: 428 -435.
 Ø")
Etiology : Cath lab Catastrophes Ø Vessel closure (Dissection, thrombus, Spasm, and no-reflow) Ø Ø Ø Introduction of Air, thrombus Perforations Anaphylaxis Major Bleed High Risk Patient

Management of Cath lab Catastrophes Ø Ø Don’t Panic BP support ; Airway Call for an extra-hand QUICK -- Underlying Etiology

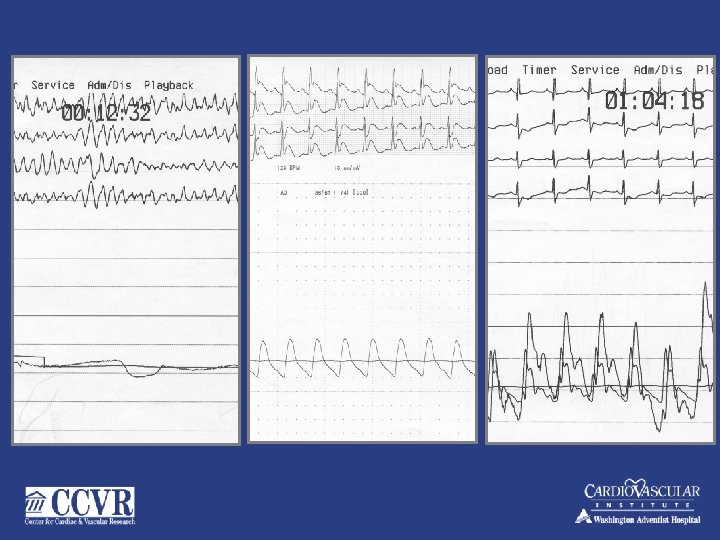
Cath Lab Catastrophes: Clinical Features: ♥ Refractory Hypotension ♥ Loss of consciousness ♥ Respiratory arrest ♥ Wide QRS rhythm / PEA ♥ Ventricular Fibrillation ( Refractory) ♥ Chest compressions
 ♥")
Cath Lab Catastrophes: Angiographic and Hemodynamic Features ♥ Occluded vessel (large viable area) ♥ Left main dissection ♥ No reflow in a major vessel (SVG) ♥ Poor clearance of dye (aortic root) ♥ Major Perforation / thrombosis/Air ♥ Narrow pulse pressure ♥ Pulmonary hypertension ♥ Worsening metabolic acidosis
 Absence of intrinsic rhythm")
Cath Lab Catastrophes: LVAD ( indications ) Absence of intrinsic rhythm

Historical Perspectives. LVAD Impella 70’s 80’s 90’s 00’s
 3. Tandem Heart 4. Impella")
Approved Percutaneous LVADs: 1. IABP 2. CPS ( ECMO) 3. Tandem Heart 4. Impella
 ♥ Intubation")
Cath Lab Catastrophes: ? When Death is Imminent Management (Requiring chest compressions) ♥ Intubation ♥ Continuation of chest compressions ♥ Emergency institution of cardiopulmonary bypass support ( ECMO ) ♥ Replace angiographic access site with CPS cannulae ♥ Flow rate 50 ml/kg/min ♥ Contralateral groin access to re-assess anatomy ♥ Re-Intervention / Emergency Surgery

56 yr. Old F, CTO LCX, RCA

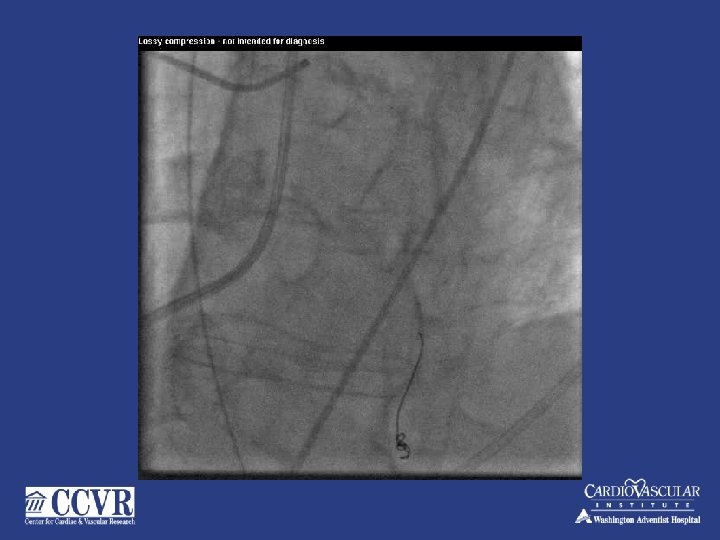
75 yr. . male –CTO RCA, for PCI to LAD



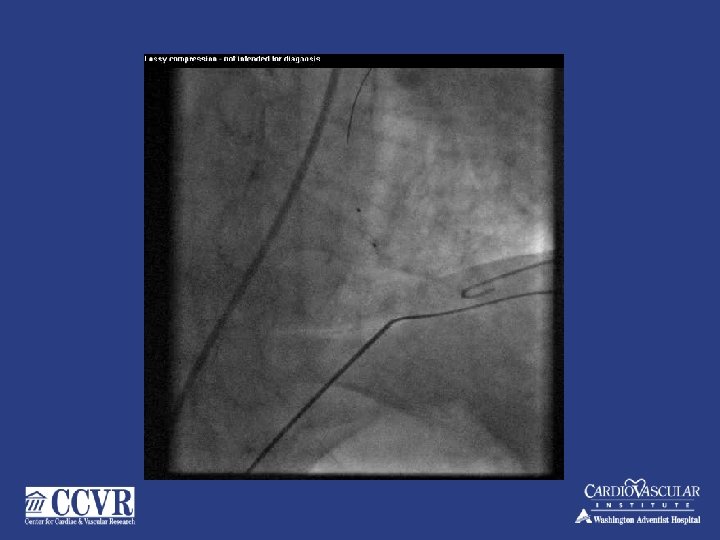
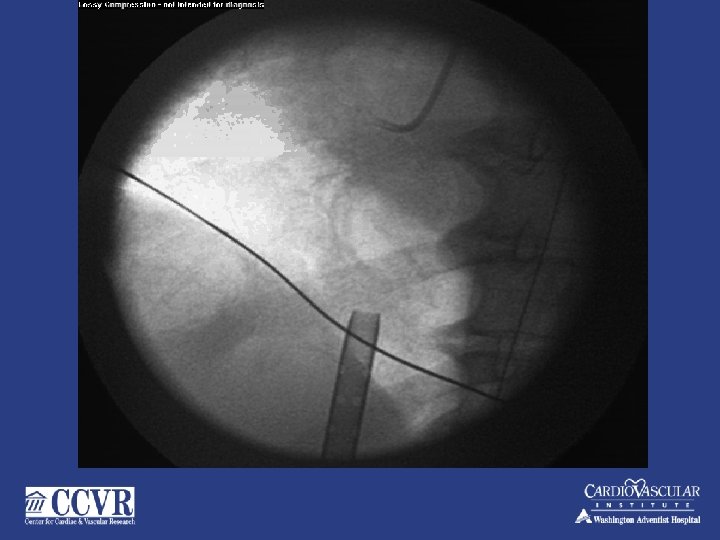
CORONARY AIR EMBOLUS

CORONARY AIR EMBOLUS


 and during")
Air Embolus v v Often from manifold injections (contrast or flush ) and during introduction of devices - TB) Prevention v Avoid pressurized flush v Back bleed before injecting Small amounts are well tolerated Large amounts cause “Air Lock” v Chest Pain v Bradycardia v Hypotension / Hemodynamic Collapse

Air Lock: Management Don’t Panic v 100% O 2 v Morphine, Atropine v Neo-synephrine 0. 1 mg. IV v I/C Epinephrine 1: 10, 000 dil. v Turn patient v Suction / Flushing v IABP v LV assist Devices (for refractory hemodynamic collapse) v

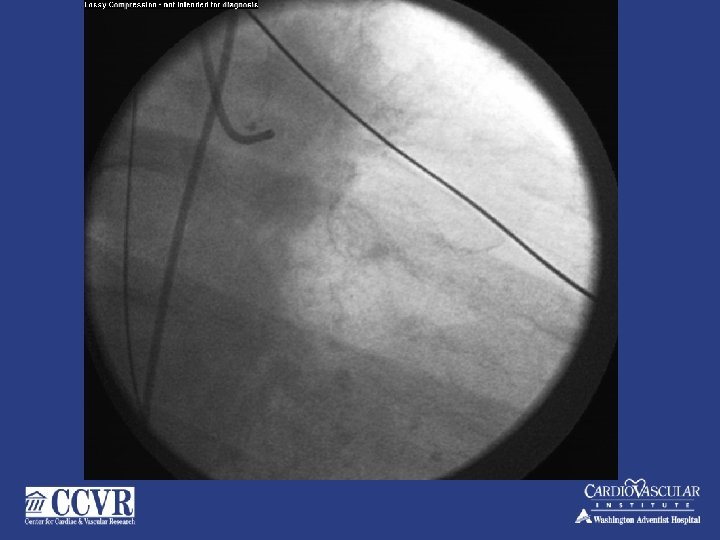
85 yr. female – Class III – PCI - LAD

DES 3. 0 X 23 mm- 16 Atm-

Type III…………

Prolonged Balloon Inflation

Refractory Cardiac Arrest- VF

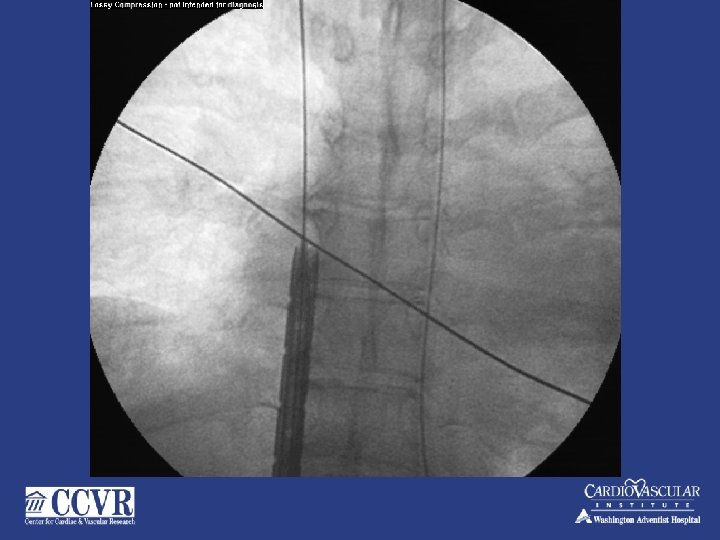
Covered Stent- with CPS

Long Sheath Still in VF- stable Hemodynamics'… On CPS – 4 L/min. Note long sheath

Post – Covered Stent – Defib. To NSR

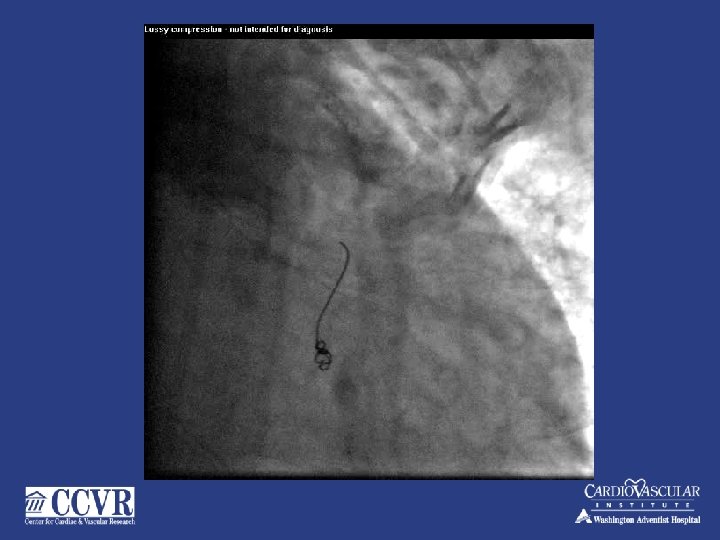
Coronary Perforation Ø Occurs in between 0. 1% - 0. 7% Ø More with ablative devices Ø More with oversizing the devices Ø Hydrophilic guide wire, Temp. Pacemaker Ø Early recognition is key to a successful outcome Ø Highest mortality among all PCI complications
 To Treat Coronary Perforations Overall Perforation Rate 0. 45% (49 / 10,")
JOSTENT (PTFE) To Treat Coronary Perforations Overall Perforation Rate 0. 45% (49 / 10, 945) PTFE (n=12) Non-PTFE (n=37) P-value In-Hospital Outcome QMI (%) 8 23. 5 0. 29 Cardiac Tamponade (%) 8 82 <0. 001 Bypass Surgery (%) 18 88 <0. 001 Death (%) 18 35 0. 28 C. Briguori et al, Circulation 2000

Coronary Perforation Ø Rapid recognition is key Ø Cardiac tamponade and hemodynamic collapse can occur in minutes. Ø Prolonged inflation- ( up to 10 min) of an oversized balloon at low pressure. Reversal of anticoagulation Ø pericardiocentesis Ø Coils, Covered stents (require post-dilation, high pressure) Javaid et al Am J Cardiol 2006; 98: 911 -4

Preventive Measures Make sure – indication for PCI Ø Watch the tip of the guide wire Ø Sizing of the device( small vessel, tortuous , Bend points) Ø During CTO: (confirm the distal end of balloon). Ø Undersize- CB, ROTO, ( Bends) Ø Do not oversize Stent ( small vessels)-do simple balloon or leave them alone- Ø ALWAYS CHECK ANGIO, before removing stent balloon– if you see—just inflate the same balloon

Standby CPS for Elective Interventions Total Number of Interventions at Washington Adventist Hospital from 4/1988 to 2/2000 N = 23, 472 Refractory Cardiopulmonary Arrest in the cath lab N=39 (0. 2%) Perforation N=7 Abrupt closure N=26* LM dissection N=5 *(no reflow in 8 & air E in one) Surgery N=10 Survived N=7 Expired N=3 Pulmonary edema N=1 Re-intervention N=29 Survived N=24 Shawl, et al. , J ACC 2001( Abs. ) Expired N=5
 v")
Standby CPS for Elective Interventions N = 23, 472 Cardiopulmonary Arrest (Imminent death) v Overall survival v Percutaneous interventions v Emergency surgery 39 (0. 2%) 31/39 (79%) 24/29 (83%) 7/10 (70%)

74 yr. old male – NSTMI – PCI to mid LAD




- Slides: 49