Critical Care Medicine Interhospital Training Program Case Presentation













 Sodium 33")























 metabolic disorders arising from defects in")



 § Autosomal recessive")
 急性間歇性卟啉病 (急性間歇性紫質症)")














. An equal volume")

 § If PBGD is deficient in normal red blood cells then the diagnosis")


 § Family screening § Avoid factors known to precipitate attacks l l")

 § High calories carbohydrates intake § Haem derivatives")












 Treatment § Is available outside USA, e. g. South Africa,")








- Slides: 93
Critical Care Medicine Inter-hospital Training Program Case Presentation Royal Disease after 1997 in Hong Kong Intensive Care United Christian Hospital
39 year-old lady…LSY… § § § Non-smoker Non-drinker No known drug allergy No history of adverse drug reaction Premorbid: active and walk unaided
39 year-old lady…History. . . § Fall and land on buttock while ice skating in Japan on 11/2006, since then on-off low back pain
39 year-old lady…c/o. . . § 4 limbs weakness for few months § Dizziness, malaise and increase generalised weakness since 20/11/2007 § Work up in Baptist Hospital newly diagnosed 1. Hypertension with LVH 2. Diabetes Mellitus with retinopathy, nephropathy and dermopathy 3. Hyperlipidaemia
39 year-old lady…was given. . . § § § Crestor 10 mg daily Diamicron MR 15 mg OM Lodoz 25 mg nocte (thiazide + bisoprostol) Calcium supplement 1 g BD Discharged from Baptist Hospital after one week hospitalisation
39 year-old lady. . . AED… § United Christian Hospital on 14/12/2007 § Low back pain § Generalised weakness, especially lower limbs precipitating fall, difficulty in walk for 2 weeks § Dizziness § Hair loss for few years
39 year-old lady. . . AED… § CXR: § H’stix § X-ray L-S spine § Urine stix Clear 5 Collapsed T 12 with normal bone density Alb +++
39 year-old lady…Medical Ward § § Moon face Alopecia DM dermatopathy Generalised muscle wasting (markedly wasted intrinsic hand muscles and thigh muscles) § Clawed hands
39 year-old lady…Medical Ward § § Vital sign stable CVS Respiratory Abdomen Unremarkable
39 year-old lady…CNS § § § GCS 15/15 Coherent Speech No tongue fasciculation Proximal UL power 4/5 Distal UL power 3/5 Proximal LL power 4/5 Distal LL power 3/5 Jerks all depressed No cerebellar sign Impaired pinprick sensation in glove and stock distribution No sensory level elicited DRE: normal anal tone and perianal sensation
Investigation on admission § § § WBC Hb MCV Platelet Hb. A 1 c 11. 2 x 10^9/L 11. 4 g/d. L 80. 2 f. L 186 x 10^9/L 9. 4
Investigation on admission 11/01/03 14/12/07 Urea 6. 1 19. 6 Creatinine 91 182 Sodium 135 126 Potassium 4. 8 3. 7 Bilirubin 12 12 ALP 94 131 Albumin 36 35 AST 25 70 ALT 20 55 CK NA 125
Investigation on admission 11/01/03 14/12/07 Urea 6. 1 19. 6 Creatinine 91 182 Sodium 135 126 Potassium 4. 8 3. 7 Bilirubin 12 12 ALP 94 131 Albumin 36 35 AST 25 70 ALT 20 55 CK NA 125
Investigation on admission § Osmol Blood 266 Urine 356 § Urine (spot) Sodium 33 § Spot Cortisol am 931 pm 737 § TSH 1. 4
Case Summary A lady with diabetes mellitus suffering from 4 limbs weakness with neuropathy, hyponatraemia and renal impairment.
Impression
Impression § 4 -limb weakness with sensory loss ? Diabetes sensori-motor neuropathy ? Guillain-Barre Syndrome ? Heavy metal poisoning § Hyponatraemia ? Drug-related ? SIADH
39 year-old lady… 18/12/2007 § Noted visual hallucination “Saw the color of the wall in ward changed to dark purple and there were some net-like things on the wall. ” § Psychiatry opinion: Likely illusion/ pseudohallucination Valium 5 mg prn nocte for sleep
39 year-old lady… 19/12/2007 § Became confused and disoriented “flashing face, vacant looking, labile mood. Felt people in the ward were from different century…said someone hurted her…” § Psychiatry reviewed: Delirium, DDx Organic psychotic disorder
39 year-old lady… 19/12/2007 § CT brain: NAD § Lumbar Puncture: Opening pressure 26. 5? ? ? CSF Appearance WBC RBC Protein Glucose (CSF/Blood) Clear <1 107 1273 4 /4. 8
39 year-old lady… 20/12/2007 § Worsening muscle weakness with bulbar & extraocular muscles involvement § HKPIC consulted Arsenic, mercury, lead checked not elevated
39 year-old lady… 21/12/2007 § MRI brain: NAD § NCV report: Severe axonal-sensori-motor neuropathy § IV Ig started by neurologist for the possibilty of Guillain Barre Syndrome § R/T feeding initiated as dysphagia due to bulbar muscle weakness § I/O chart: Dark urine, urine stix RBC neg
39 year-old lady… urine www. porphyriafoundation. com
Any Comment?
39 year-old lady… 22/12/2007 § § § Deteriorating muscle weakness Respiratory failure with desaturation Urgent intubation 1 episode of PEA during intubation To ICU for further care…
39 year-old lady…in ICU § Required high inotropic and ventilator support § Multi-organ failure § DIC § ACS § Pneumonia § Put on CRRT support
39 year-old lady… urine result
39 year-old lady… … § Porphobilinogen = Positive § Urine – porphyrins = Positive § Diagnosis: Acute intermittent Porphyria (AIP) § Genetic sequencing confirmed the diagnosis Heterozygous for p. L 137 P 3
Impression § Young lady with newly diagnosed diabetes mellitus with acute intermittemt porphyira. Acute attack was suspected triggering by both relative normal glucose level and oral hypoglycaemics.
Family Genetic Screening § Father § Elder sister’s son
39 year-old lady… § Initiated high carbohydrate nutritional support i. e. 400 g glucose/day (D 20 IVI 500 ml/Q 12 H + enteral feeding) § Avoid precipitating drugs § Panhematin (Hemin) arranged from overseas
39 year-old lady… § First dose of Panhematin was given on 14/1/2008 § Required life-saving CVVH since 15/1/2008, so Panhematin was withheld § Remaining dose of Panhematin resumed after 17/1/2008
39 year-old lady… 26/1/2008 § Despite active management, she developed cardiac arrest and not responsive to resuscitation. § Passed away on 26/1/2008 (ICU LOS: 35 days)
Prophyrias § Derives from the Greek “porphura”, meaning "purple pigment". This is likely to reference to the purple discolouration of some body fluids in patients during an attack. § Original descriptions are attributed to Hippocrates, the disease was first explained biochemically by Felix Hoppe-Seyler in 1874 and acute porphyrias were described by the Dutch physician B. J. Stokvis in 1889.
King George III A portrait of ‘Mad King George’, by Nathaniel Dance. The king suffered from an illness now thought to be porphyria.
Prophyrias § The ‘Royal Disease’ because sufferers are believed to have included Mary Queen of Scots, King James I, and King George III.
Prevalence of Porphyria § Varies widely from country to country § Also depends on the type of porphyria. § Overall prevalence of overt cases in the United Kingdom is about 1 in 25, 000 population for porphyria cutanea tarda and less than 1 in one million for congenital erythropoietic porphyria. § In Taiwan, the overall prevalence of overt cases is about 1 in 300, 000
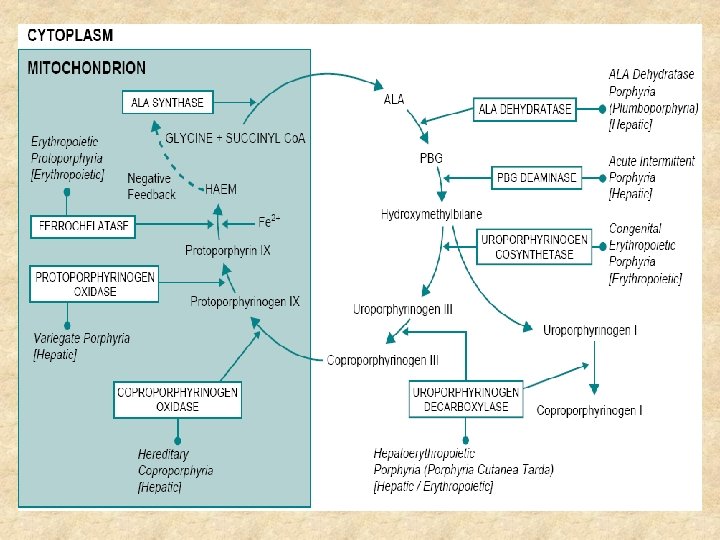
Porphyrias § The porphyrias are (genetic or acquired) metabolic disorders arising from defects in the biosynthetic pathway leading to the production of haem (haem synthetic pathway). § Glycine and succinyl-Co. A combine to form the first porphyrin precursor, aminolaevulinic acid (ALA); two molecules of ALA then combine to form the second porphyrin precursor porphobilinogen (PBG), and four molecules of PBG combine to form uroporphyrinogen. § Uroporphyrinogen is the first true porphyrin
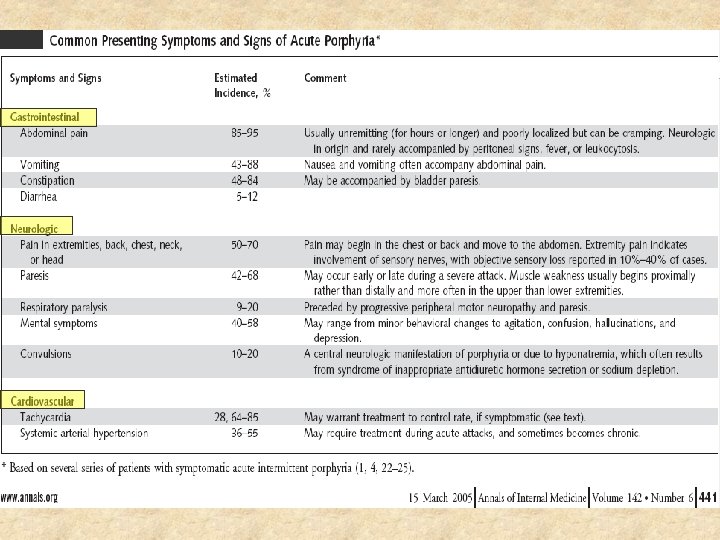
Porphyrias Clinical Manifestation § Acute attack also known as the acute porphyric crisis, is marked by severe abdominal pain and an autonomic neuropathy (typically presenting as hypertension, tachycardia and ileus), which may progress to a motor neuropathy with respiratory failure and death. § Photocutaneous sensitivity presents with increased skin fragility, blistering, erosions and scars in sun-exposed areas.
Clinical Effects and mode of inheritance of Porphyria
Clinical Effects and mode of inheritance of Porphyria
Inheritance of Porphyria § Autosomal dominant -Heterozygous -Homozygous (very severe disease) § Autosomal recessive § Porphyria with complex inheritance the disease only presents clinically when a mutation on one allele is accompanied by a so-called "low-expression" allele on the other chromosome. § Variable expression Approximately 40% of patients who inherit the typical South African (R 59 W) mutation for variegate porphyria will show neither skin disease nor acute attacks. The proportion of asymptomatic patients (latent case) with acute intermittent porphyria is even higher (Only 1015% of gene carriers develop the clinical syndrome. )
Acute Intermittent Porphyria (AIP) 急性間歇性卟啉病 (急性間歇性紫質症)
Acute Intermittent Porphyria § The commonest type of the acute porphyrias § Only 10 -15% of gene carriers develop the clinical syndrome. § A third of patients have no family history. § About 1% of acute attacks of porphyria may be fatal.
Genetic Defect of AIP § Autosomal dominant trait § Both males and females are equally affected in South Africa while more females are affected in Taiwan § More than 100 mutations associated with acute intermittent porphyria had been described throughout the world.
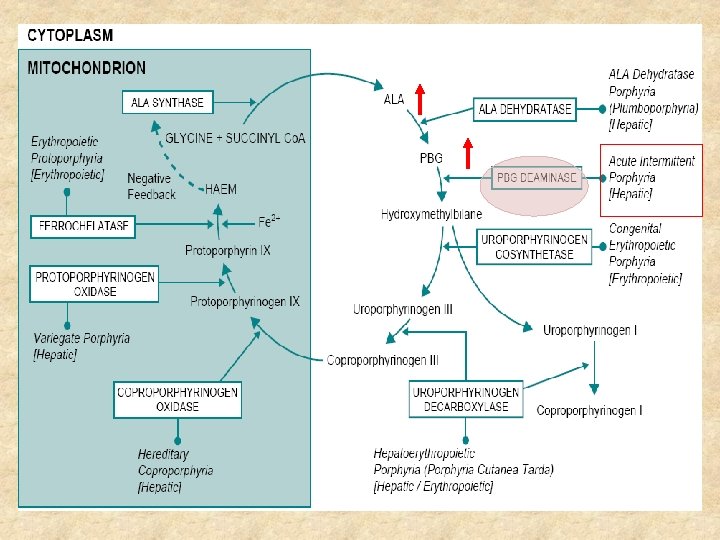
Acute Intermittent Porphyria § Accumulation of ALA and PBG is associated with the acute attack, so patients with acute intermittent porphyria are particularly prone to acute attacks. § The porphyrins, which are photoactive, do not accumulate to a significant extent, and acute intermittent porphyria is therefore never complicated by skin disease.
Frequency of signs and symptoms in Acute Porphyria Copyright © 2000 BMJ Publishing Group Ltd. Thadani, H. et al. BMJ 2000; 320: 1647 -1651
Pathogenesis & Precipitating Factors
Mechanism of neurotoxicity § The pathogenesis of the clinical features is poorly understood § Possible mechanisms: 1. Damage by free radicals 2. Direct neurotoxicity of aminolaevulinic acid 3. Haem deficiency in nervous tissue § § § Monterio H, Bechara EJH, Abdalla DSP. Free radicals involvement in neurological porphyrias and lead poisoning. Mol Cell Biochem 1991; 103: 73 -84 6. Bonkovsky HL. Advances in understanding and treating "the little imitator", acute porphyria. Gastroenterology 1993; 105: 590 -594 7. Lindberg RLP, Parcher C, Grandchamp B. Porphobilinogen deaminase deficiency in mice causes a neuropathy resembling that of human hepatic porphyria. Nat Genet 1996; 12: 195 -199
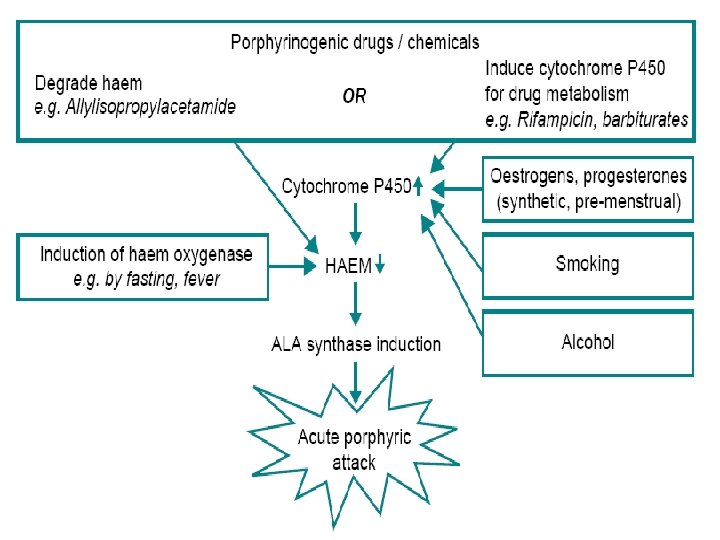
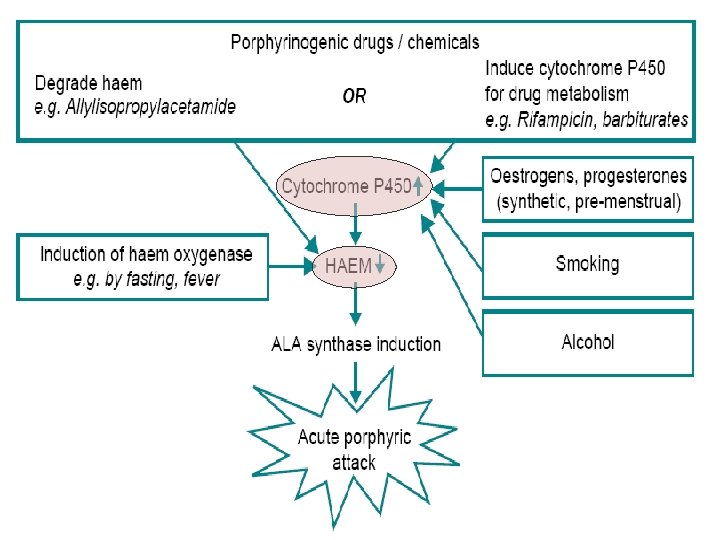
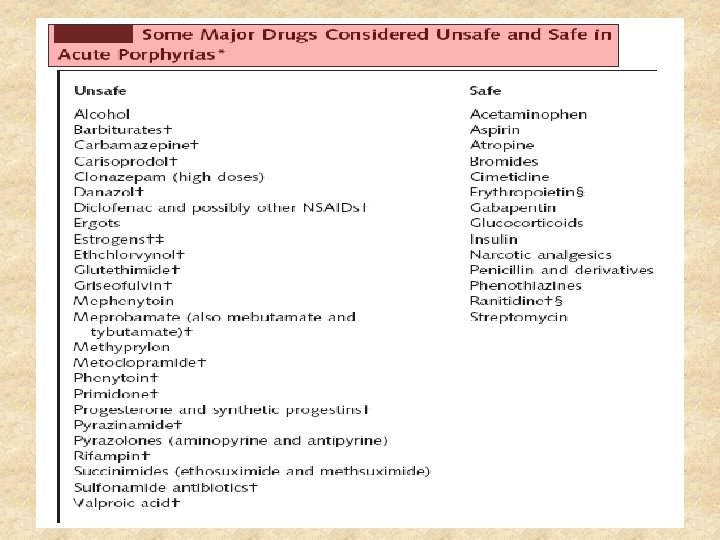
Precipitating Factors of Porphyria acute attacks § Drugs: barbiturates and oestrogens (may be safe in replacement doses), progesterones, sulphonamides, methyldopa, danazol, diazepam, phenytoin, carbamazepine, sulphonylureas, chloramphenicol, tetracyclines, some antihistamines § Fasting § Smoking § Alcohol § Substance misuse: marijuana, ecstasy, amphetamines, and cocaine § Infection § Emotional and physical stress § Cyclic factors: premenstrual attacks are common
Triggers of acute attack § Drugs l Induce ALA synthase activity • Induction of hepatic cytochrome P 450 activity • Destruction of Haem • Inhibition of haem synthesis
www. drugs-porphyria. com
Triggers of acute attack § Hormonal factors l Endogenous steroids • Premenstrual attacks • Female preponderance: young women • Increase level of estrogen/ progesterone § Caloric deprivation l Fasting induces hepatic haem oxygenase Loss of feedback inhibition of ALA synthatase § Alcohol induces cytochrome P 450
Triggers of acute attack § Infections l Fever ? Induce haem oxygenase § Smoking l cytochrome P 450 induction
Investigation
Investigation § Clinical History § Family History § Diagnostic Test -A definitive diagnosis of the type of porphyria. -An estimation of the biochemical activity of the porphyria. (In general there is a relationship between the degree of elevation of urine ALA, PBG and porphyrins and the likelihood that acute symptoms are due to porphyria. ) -Identification of the mutation responsible for the porphyria in the patient (important in subsequent screening of the family).
Investigation § Urine porphyrin and precursor analysis -An initial qualitative screening test for both porphobilinogen (the Watson-Schwartz reaction) and urine porphyrins (Dean's method) should be performed on a urine sample. -If tests are positive, proceed to a chromatographic quantitation of ALA, and PBG and porphyrins. § Stool porphyrin analysis -variegate porphyria -hereditary coproporphyria
The Watson-Schwartz test Urine is placed in a test tube (A). An equal volume of Ehrlich's aldehyde is added. A weakly positive reaction is denoted by a rose-pink colour A strongly positive reaction by a red colour (B). Chloroform is added, the tube is mixed and allowed to settle. Chloroform and water are immiscible and the chloroform, being heavier, sinks to the bottom. If the red colour remains in the top, aqueous phase, this confirms the presence of PBG (C). http: //www. porphyria. uct. ac. za
Investigation § Erythrocyte fluorescence -Positive test suggests erythropoietic protoporphyria or congenital erythropoietic porphyria § Plasma scan (commonly used in South Africa) -more sensitive than stool porphyrin analysis -Variegate porphyria peaked at 625 nm -acute intermittent porphyria and porphyria cutanea tarda peaked at 619 nm § DNA analysis
Investigation(AIP) § If PBGD is deficient in normal red blood cells then the diagnosis of AIP is established. § However, measuring PBGD in red blood cells should not be relied upon by itself to exclude AIP in a sick patient, because the enzyme is not deficient in red blood cells of all AIP patients. § In some AIP families, PBGD is normal in red blood cells and is deficient only in the liver and other tissues. http: //www. porphyriafoundation. com
Laboratory Evaluation of Patients suspected suffering from acute porphyria
Treatment
Treatment (General) § Family screening § Avoid factors known to precipitate attacks l l Avoid precipitating drugs Treat infection promptly Maintain adequate calorie intake Avoid smoking and alcohol § General measures in treatment of acute attack
Treatment § General measures
Treatment (Specific) § High calories carbohydrates intake § Haem derivatives
Treatment Carbohydrates
Treatment – Carbohydrates § Early case studies suggested carbohydrate either PO/ IV loading may benefit in some patients § Carbohydrate ingestion blocks d-aminolevulinic acid (ALA)-synthase. * § However, the mechanisms by which carbohydrates modulate the components of porphyrins and heme synthesis are highly complex and only partially elucidated. § 200 - 500 g per day of carbohydrate intake via enteral feeding +/- IV infusion *Doss M, Verspohl F: The "glucose effect" in acute hepatiac porphyrias and in experimental porphyria. Klin Wschr 9: 727– 735, 1981
Effects of DM on AIP patients
Beneficial Effect of Diabetes on Acute Intermittent Porphyria Diabetes Care 25: 797 -798, 2002 Folke Lithner, MD, PHD Department of Internal Medicine, University Hospital, Umea, Sweden Andersson C, Bylesjo I, Lithner F: Effects of diabetes mellitus on patients with acute intermittent porphyria. J Intern Med 245: 193– 197, 1999
Beneficial Effect of Diabetes on Acute Intermittent Porphyria § Population-based study on AIP patients aged >/= 18 years living in northern Sweden § Total 16 patients (5 women) with AIP and type 2 diabetes identified with a mean age of 67 years § Eight of these patients had AIP symptoms, with three patients suffering severe, recurring attacks § After the onset of their diabetes, no patient suffered attacks or any other AIP symptoms § Mean values of a 52 -year-old woman on 13 occasions of testing for urinary porphobilinogen (PBG) during 6 months before and on 11 occasions during the first 4 months after she developed diabetes were 65. 9 and 10. 2 μmol/l, respectively (reference levels 1. 3– 11. 0 μmol/l) (P = 0. 0001).
Effects of DM on AIP patients
Treatment Haem derivatives
Treatment – Haem derivatives § Hemin / haem arginate § Biochemical improvement was not paralleled by marked clinical improvement § Clinical improvement rapid if given within 1 -2 days if started early in an attack § Delayed treatment neuronal damage maybe advanced and slow to recover § Disadvantage l Induces haem oxygenase breaks down haem potentially obviating benefits
THE ACTION OF HAEM ARGINATE § When haem arginate is administered intravenously, it is taken up by the liver and the resulting increase in haem levels is sensed, ALA synthase is down-regulated and the increased flow through the pathway stops. ALA and PBG levels fall rapidly, and clinical improvement follows.
Treatment – Haem derivatives § Indications: -Severe attack (severe symptoms, hyponatraemia, convulsions, indicators of incipient neuropathy) -Acute attack which does not improve within 24 hours of admission -Frequent, repeated acute attacks while previous attacks do not settle unless haem arginate is given
Panhematin® Treatment § Ovation Pharmaceuticals, Inc § The only commercially available heme therapy in the United States (FDA approved) § lyophilized form of alkaline heme § should be infused into a large peripheral vein. § 3 -4 mg/kg of Panhematin® given once daily for four days early in an attack produces a highly beneficial effect in most patients.
Panhematin® Treatment § Used since the first report in 1971 § Heme therapy was recommended that it be initiated after several days of glucose therapy was unsuccessful § Periodic infusions of Panhematin® can even prevent attacks § Many experts recommend reconstituting Panhematin® with albumin as this makes it more stable. § This helps prevent phlebitis and an anticoagulant effect.
Haem Arginate (Normosang ®) Treatment § Is available outside USA, e. g. South Africa, European countries § The recommended dose for haem arginate is 3 mg/kg (to a maximum of 250 mg) once daily for 4 consecutive days.
Administration of Haem derivatives § It should be administered as an intravenous infusion in 100 m. L of sodium chloride 0. 9% over 30 minutes into a large vein in the forearm or via a central line. § A 15 -20 micron in-line filter should be used to filter out any unseen particles from the dark solution. § It is recommended that haem arginate is diluted in sodium chloride 0. 9% in a glass bottle.
Effect of Haem derivatives Treatment § Urine ALA, PBG and porphyrins will be dramatically reduced within 24 hours § Symptoms begin improving after 24 hours § However -> -haem arginate will not reverse established neuropathy -cannot be used prophylactically -too frequent use may, by inducing the enzyme haem oxygenase, induce its own catabolism with resultant loss of effect.
Side Effects of Haem derivatives Treatment § § Coagulopathy Thrombocytopenia Phlebitis Because the product is made from human blood, it may carry a risk of transmitting infectious agents, e. g. , viruses, and theoretically, the Creutzfeldt. Jakob disease (CJD) agent. § Reversible renal shutdown has occurred with administration of excessive doses
Evoultion of the Acute Attack § Motor neuropathy represents severe damage to the nervous system. § If compete quadriparesis is present, recovery normally proceeds as follows: -requirement for manual ventilation, approximately 6 -8 weeks -time before hands can be used to manipulate objects: 8 -12 weeks -time to walking with support: 5 -6 months -time to near-full recovery: approximately 12 months.
Medic. Alert®
Discussion
Treatment consideration -CVVH affects heme derivatives concentration in blood?
Thank You