Creepy Crawly Killers TickBorne Illnesses Tick Identification Lyme

Creepy, Crawly Killers Tick-Borne Illnesses

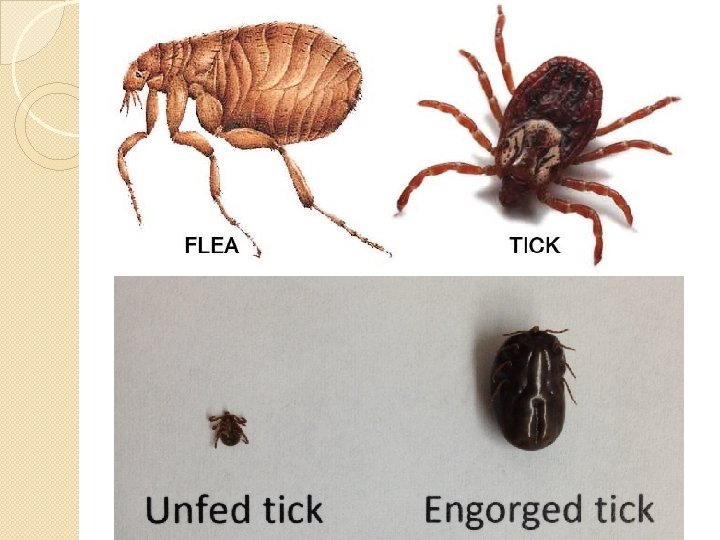
Tick Identification

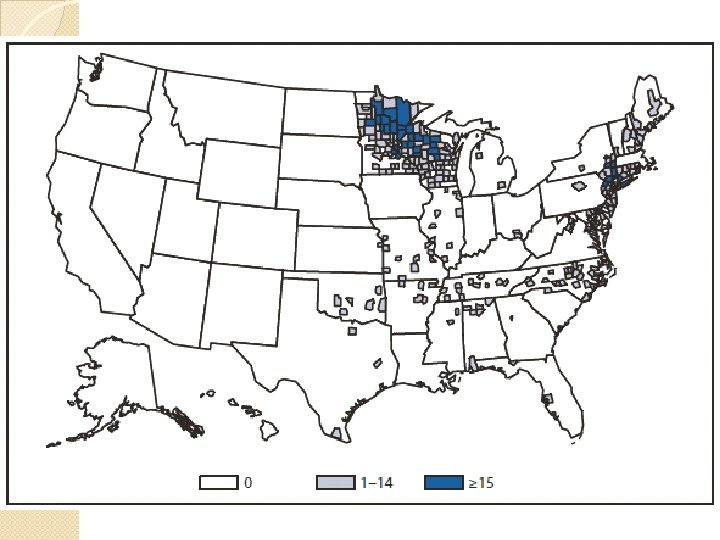
Lyme Disease �Transmitted “deer tick” by Ixodes scapularis

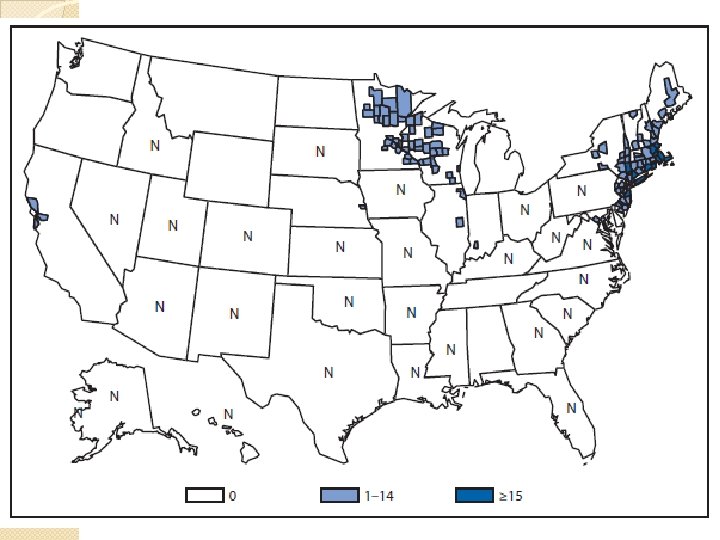
Borrelia burgdorferi �Most common vector-borne zoonotic infection in the United States
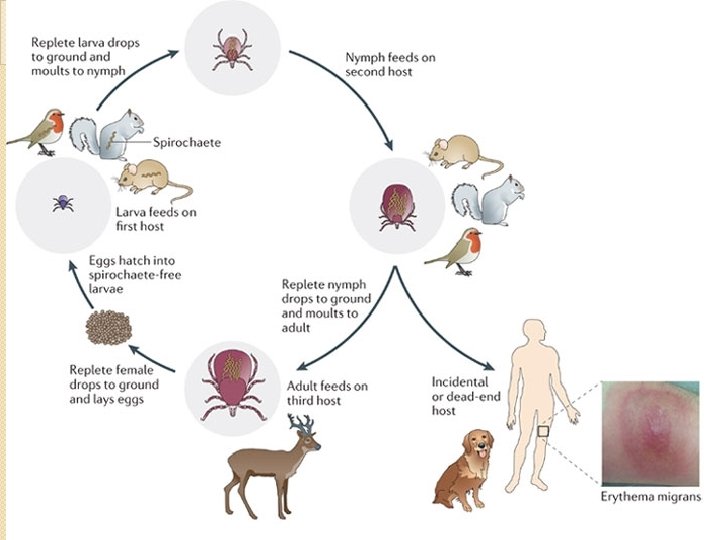

Seasonal Variation �Most cases occur in the warmer months ◦ Outdoor activity is highest ◦ Nymph activity is at its peak

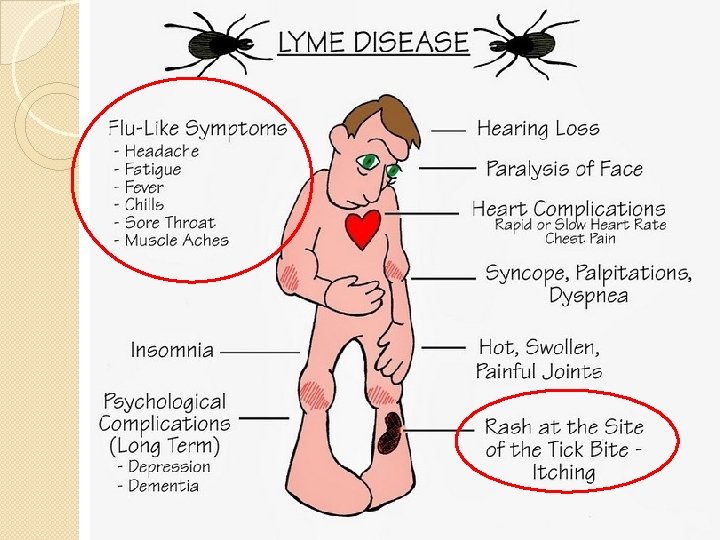
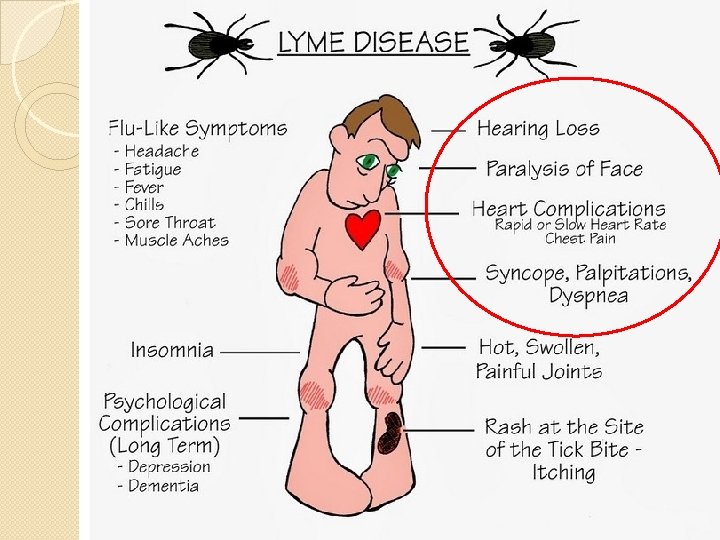
Stages: Primary �Symptoms: 7 -10 days after bite �Erythema migrans: 80% of patients �Belt line, axillary, inguinal, or popliteal � 25% report bite
 Anorexia (26%) Myalgias (44%) and arthralgias")
Stages: Primary �Flu-Like Symptoms ◦ ◦ Fatigue (54%) Anorexia (26%) Myalgias (44%) and arthralgias (44%) Fever (16%) �Regional lymphadenopathy (23%) �Headache (42%), neck stiffness (35%) ◦ Meningeal findings absent, CSF studies normal

Stages: Secondary Rash can evolve

Stages: Secondary �Cranial neuropathy �Meningoencephalitis �Meningeal signs typically absent �CSF studies may be positive

Stages: Secondary �Myopericarditis

Stages: Secondary �Atrioventricular block


Stages: Secondary �Rarely ◦ ◦ ◦ Conjunctivitis Keratitis Uveitis Optic neuritis Blindness
 � 60%")
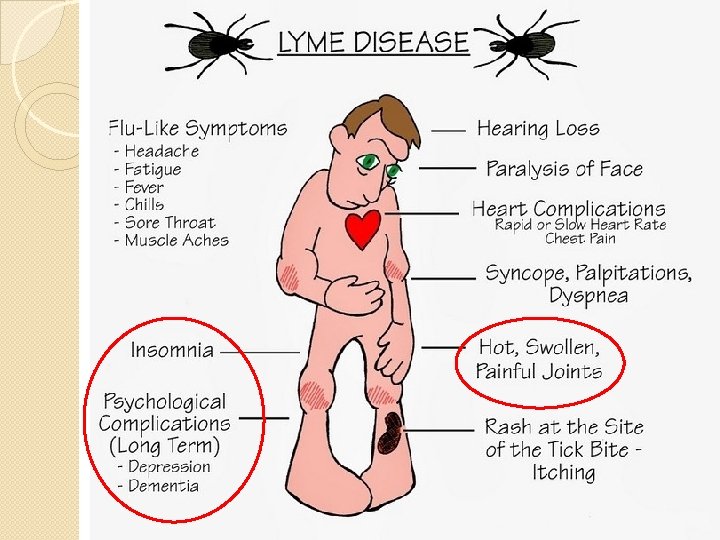
Stages: Tertiary �Months - Years after bite �Joint complaints (usually larger joints) � 60% of untreated patients: monoarticular or oligoarticular arthritis � Exacerbations less frequent over years

Stages: Tertiary �“Lyme encephalopathy” ◦ Mood, memory, cognition, and sleep changes �Polyneuropathy �Both have abnormal CSF studies

Diagnosis �Skin findings in endemic area �ELISA Ig. G and Ig. M against Borrelia (sensitivity of 89% and specificity of 72%) ◦ Many false-positives ◦ Positive or equivocal ELISA tests may be confirmed with western blot

Treatment �Tick removed within 72 hours: low likelihood of infection �Tick attached for at least 36 hours: consider treatment

Treatment: Primary + Secondary Stages �Doxycycline ◦ Adults: 100 mg BID for 14 -21 days ◦ Children > 8 years: 1 -2 mg/kg BID �Amoxicillin ◦ Pregnant or lactating: 500 mg TID for 14 -21 days ◦ Children < 8 years: amoxicillin 50 mg/kg/day, divided TID (max dose of 500 mg/dose)

Treatment Exceptions • Ceftriaxone • Lyme Meningitis • Severe cardiac disease �Second or third degree heart block �PR > 300 msec �Symptomatic patients
. ◦ 2")
Co-Infections �Babesiosis ◦ 2 -40% of lyme patients �Human granulocytic anaplasmosis (HGA). ◦ 2 -12% of lyme patients �Doxycycline does not treat babesiosis �Amoxicillin does not treat HGA or babesiosis �Fever persists past 6 days: suspect co -infection
 �Transmitted by deer tick")
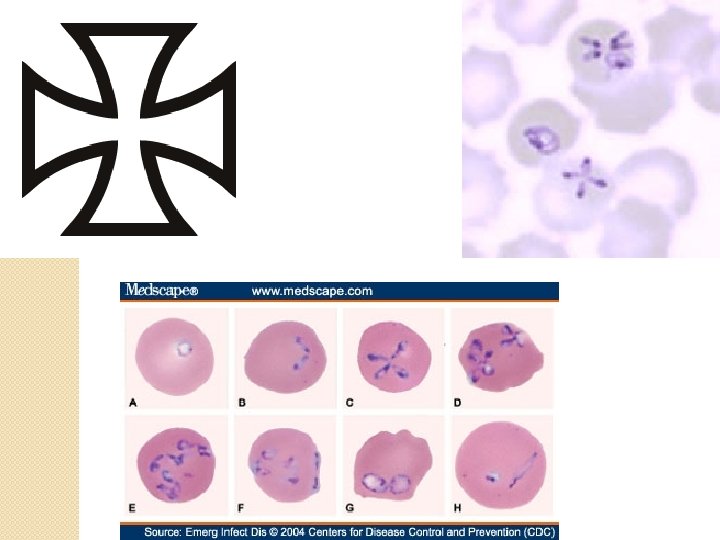
Babesiosis �Babesia species (especially microti) �Transmitted by deer tick

Clinical Presentation �Flu-like illness: fever, chills, headache, fatigue, and anorexia �Splenomegaly �More severe in splenectomized ◦ Severe hemolytic anemia, hemoglobinuria, jaundice ◦ MOD: renal insufficiency, ARDS, and DIC

Diagnosis �Microscopy of thick and thin Giemsa stains �Antibody detection through IFA staining �PCR

Treatment �With spleen: generally recover without treatment �Severe disease, splenectomized ◦ Clindamycin + quinine x 7 -10 days OR ◦ Atovaquone + azithromycin x 7 -10 days
 ◦ Anaplasma phagocytophilum ◦ Black-legged tick ◦ Upper Midwest,")
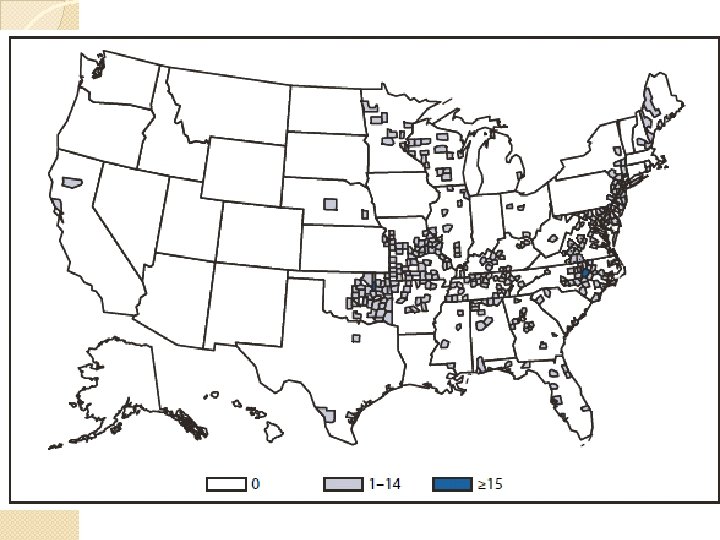
Ehrlichioses �Human granulocytic anaplasmosis (HGA) ◦ Anaplasma phagocytophilum ◦ Black-legged tick ◦ Upper Midwest, New England, parts of the mid-Atlantic states, northern California �Human monocytic ehrlichiosis (HME) ◦ Ehrlichia chaffeensis ◦ Lone Star tick ◦ South central and South east �Ehrlichia ewingii ◦ South central

Clinical Presentation �Abrupt onset of flu symptoms: fever, headache, myalgia, and shaking chills �Can see GI: N/V, diarrhea, abdominal pain �Rashes (HME>HGA) �Meningitis �Carditis �MOD ◦ Renal failure ◦ DIC ◦ ARDS

Diagnosis �Clinical �Leukopenia, thrombocytopenia �Elevated LFTs �Acute and convalescent antibodies �Enzyme immunoassay and Western blot �PCR

Treatment �Doxycycline or tetracycline x 7– 14 days �Rifampin in children if concern for tooth staining

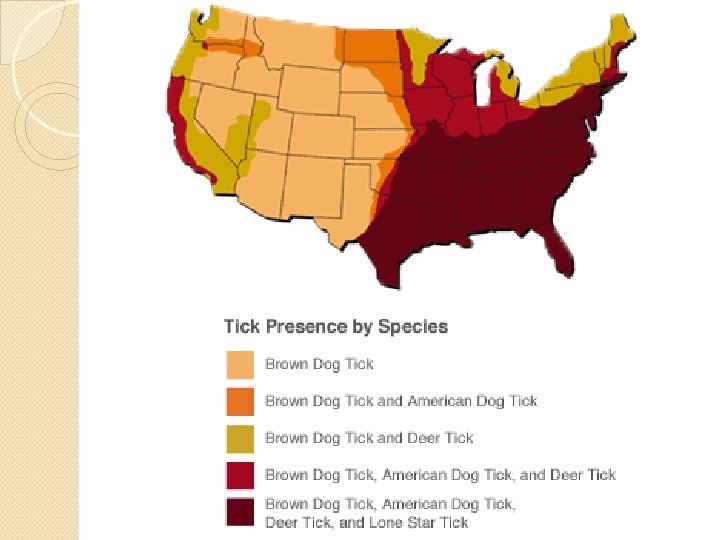
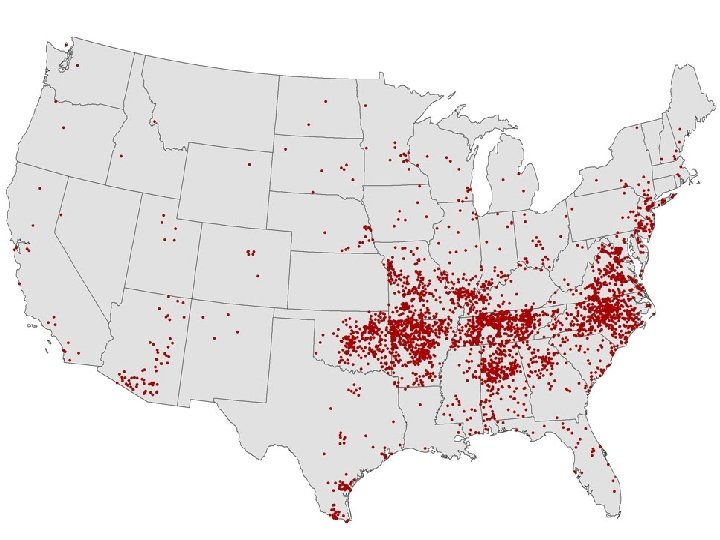
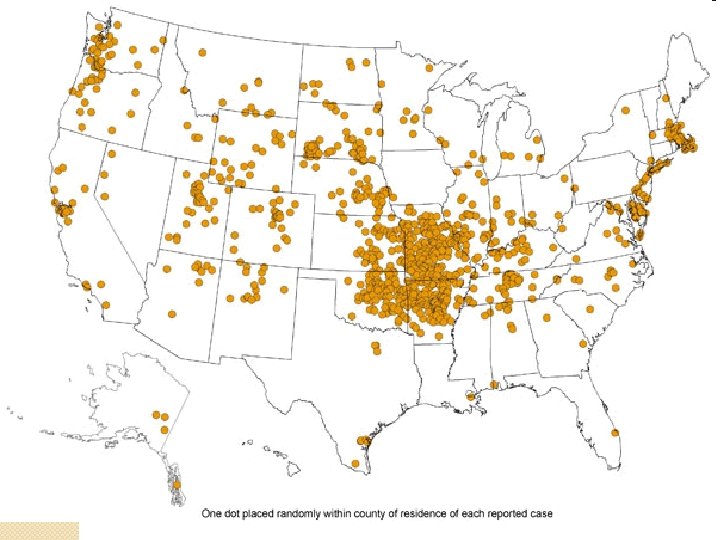
Rocky Mountain Spotted Fever �Rickettsia rickettsii �Southeastern United States �American dog tick, Rocky Mountain wood tick, common brown dog tick, Lone star tick �Frequently transmitted to humans by dogs

Infection Cycle �Infect vascular endothelial cells and vascular smooth muscle �Cell-to-cell transfer via actin-based motility �Damaged endothelium with exposed subendothelium, tissue plasminogen activator, and von Willebrand's factor

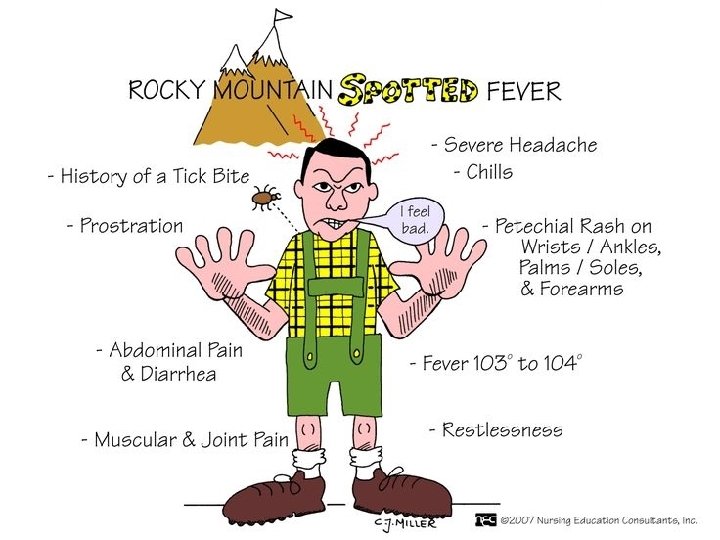

Clinical Presentation �Vasculitis and thrombocytopenia ◦ Early rash ◦ Petechial and hemorrhagic lesions ◦ Microinfarcts �Small-vessel permeability ◦ Hypotension, edema, and increased extravascular fluid • Acute renal failure and hypovolemic shock • Direct lung invasion: interstitial pneumonitis

Diagnosis �Clinical �Immunofluorescent assay and immunoperoxidase staining of R. rickettsii in rash biopsies �Serum antibody titer �PCR �Cell culture
")
Treatment �Doxycycline ◦ Including children! • Chloramphenicol � Pregnant women (except those near term) � For significant contraindication to tetracyclines • High-dose steroids in critically ill
 ◦ Borrelia recurrentis • Endemic (tick-borne) � Borrelia hermsii �")
Relapsing Fever �Epidemic (louse-borne) ◦ Borrelia recurrentis • Endemic (tick-borne) � Borrelia hermsii � Borrelia turicatae � Borrelia parkeri • Mountain and Pacific states � Elevations 2, 000 -7, 000 ft with coniferous forest

Relapsing Fever �Rodent-Tick/Rodent-Louse life cycle �Transmitted in infected saliva

Clinical Presentation �Febrile episode: ~ 3 days �Asymptomatic period: ~7 days �Relapse ◦ Antigenic variation ◦ Cycle repeats itself three to five times ◦ Successive relapses usually less severe


Diagnosis �Spirochetes on peripheral smear �Genus-specific PCR tests from CDC �Differential ◦ malaria, typhus, dengue, yellow fever, Colorado tick fever, and tularemia

Treatment �Tetracycline or erythromycin � 33% have Jarisch-Herxheimer ◦ Approx. 4 hours after treatment ◦ Flu-like illness: fever, chills, headache, myalgia, flushing ◦ Skin lesions ◦ Hypotension

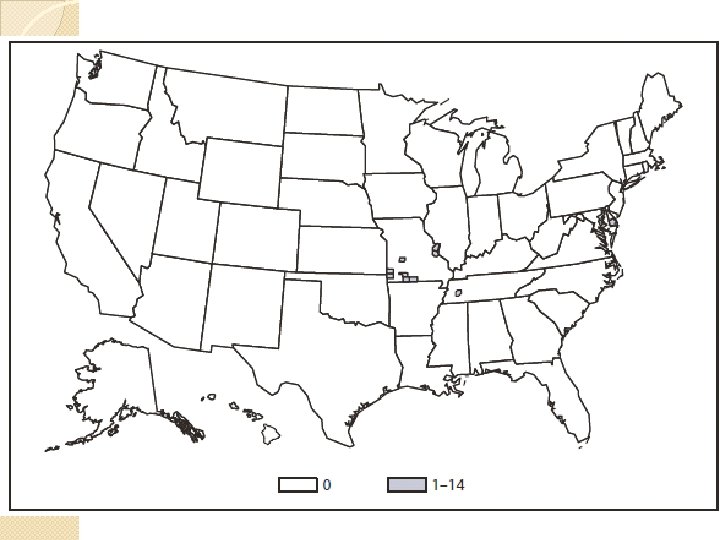
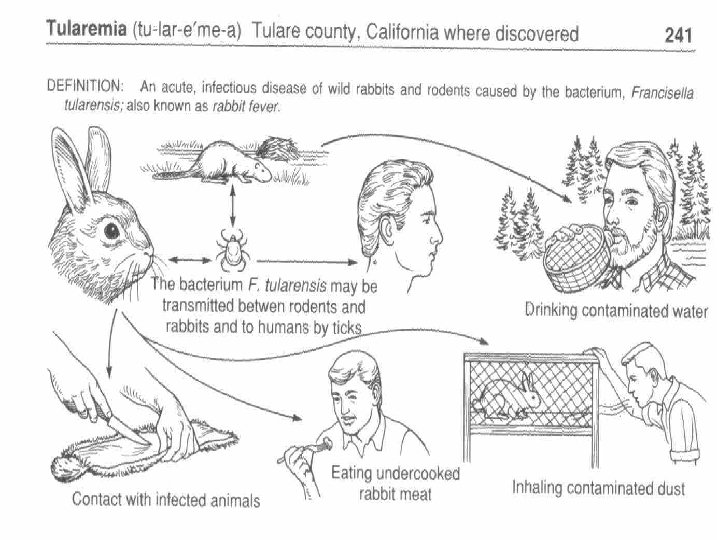
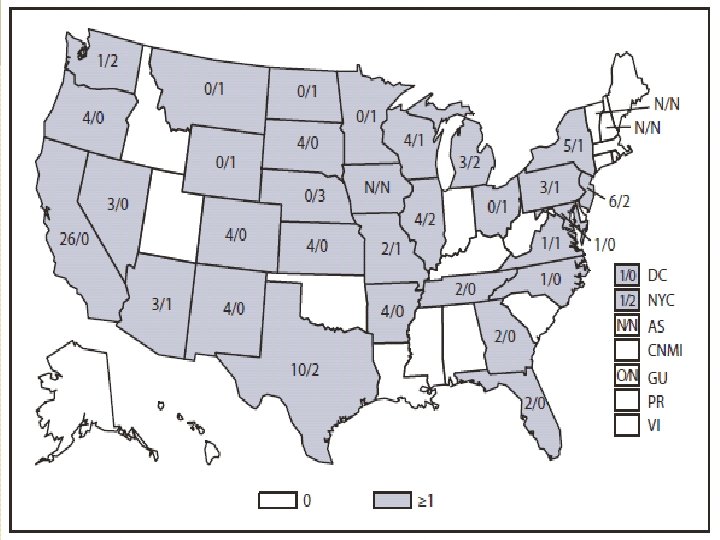
Tularemia �Francisella tularensis �Most common in Southwest �Rodents, rabbits, prarie dogs �Deer tick, the Lone Star tick, and the dog tick �Horse fly, and deer fly �Infected food or water �Inhalation of dust or water aerosol

Seasonal Variation �May to August: ticks �December to January: hunting/skinning of infected animals

Clinical Presentation �Ulceroglandular ◦ Most common form ◦ Inoculation site erythematous papule ulcerates 2 to 3 days later ◦ Regional lymphadenopathy and fever
 without skin ulcer. ◦ Oropharyngeal tularemia �exudative")
Clinical Presentation �Glandular ◦ LAD (usually cervical) without skin ulcer. ◦ Oropharyngeal tularemia �exudative pharyngitis with associated cervical lymphadenitis ◦ Oculoglandular �Unilateral conjunctivitis with regional adenopathy of pre-auricular lymph nodes

Clinical Presentation �Typhoidal: systemic form with no obvious entry site ◦ Fever, chills, constipation/diarrhea, abdominal pain, and weight loss ◦ 30 to 60% mortality �Pulmonary ◦ Direct inhalation of aerosolized organisms or bacteremic spread from another site ◦ Fever, chills, cough, substernal burning, dyspnea

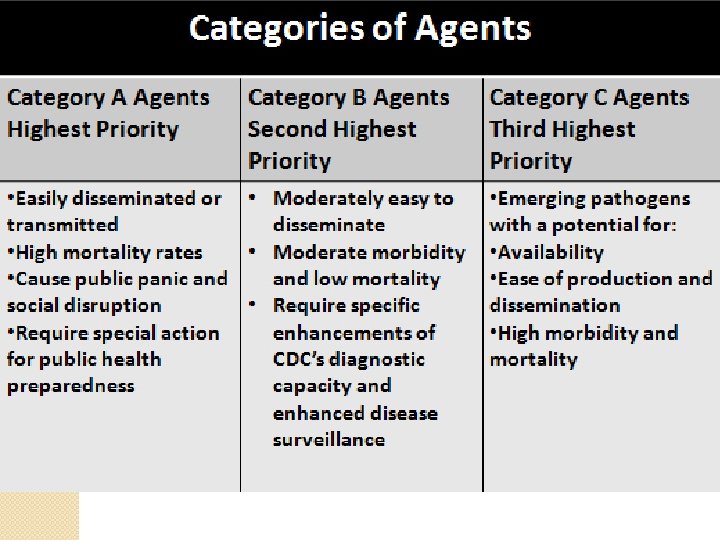
Bioterrorism �Category A �Release of aerosolized particles ◦ ◦ ◦ 3 to 5 days after exposure Acute fever Pneumonia Pleuritis Hilar lymphadenopathy

Diagnosis �PCR �Do not culture bubo ◦ Notify lab personnel if you do

Treatment �Do not need patient isolation �Streptomycin �I&D residual sterile buboes after completion of antibiotics �Prophylaxis with doxycycline

Q Fever �Coxiella burnetii �Cattle, sheep, goats �Rocky Mountain wood tick �Midwest states and California � 80% of cases in males �Extremely resistant �One organism can cause infection �Category B biologic warfare agent
 �Fever (often 40° C or higher), myalgia �Chest pain �Atypical PNA")
Clinical Presentation (Acute) �Fever (often 40° C or higher), myalgia �Chest pain �Atypical PNA �Retrobulbar headache

Chronic �Granulomatous hepatitis �Culture-negative endocarditis ◦ Up to 68% of patients with chronic Q fever ◦ Up to 25% mortality rate ◦ Usually a history of valvular heart disease
 �ELISA assays ◦ Takes 2 -")
Diagnosis �Do not culture (risk to lab workers) �ELISA assays ◦ Takes 2 - 3 weeks

Treatment • Uncomplicated acute � Doxycycline • Acute disease with valvular disease � Doxycycline + Hydroxychloroquine x 1 year • Chronic � Doxycycline + Hydroxychloroquine x 1. 5 to 3 years • Pregnant � Long-term TMP/SMX • Prophylaxis � Doxycyline x 5 -7 days

Colorado Tick Fever �Coltivirus �Rocky Mountain area �Rocky Mountain wood tick
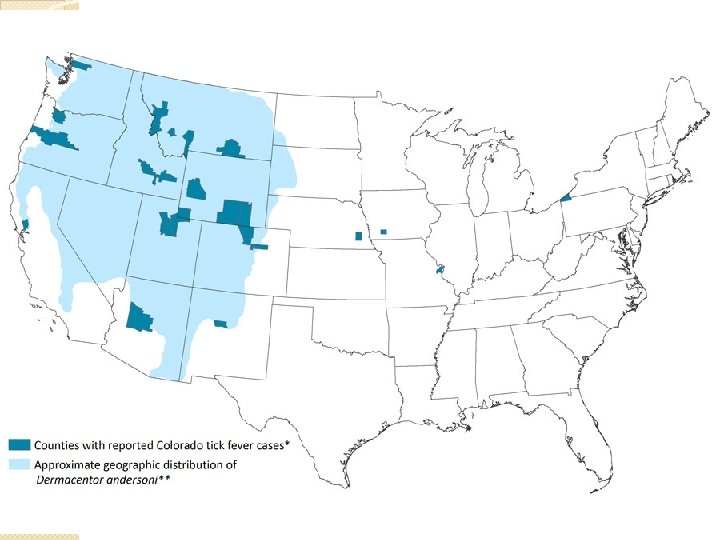

Clinical Presentation �Flu-like: fever, chills, headache, myalgia, lethargy, anorexia, and nausea �Retrobulbar pain �Biphasic course : “saddleback” fever curve ◦ Sick for 2 - 3 days ◦ Well for 1 - 2 days ◦ Sick 2 - 4 days

Diagnosis �Immunofluoroescence �PCR

Treatment �Almost always self-limited �Supportive treatment

Tick Paralysis �Adult female tick �Releases a neurotoxin that causes cerebellar dysfunction, ascending paralysis �Southeastern and northwestern regions of the United States � 47 tick species: most common Rocky Mountain wood tick and American dog tick

Mechanism �Ixobotoxin stops sodium flux across axonal membranes loss of acetyl choline release at neuromuscular junction

Clinical Presentation �Restlessness and irritability �Ascending flaccid paralysis +/- acute ataxia ◦ bulbar involvement, respiratory paralysis, �https: //www. youtube. com/watch? v=24 DZEa. UN 7 cc

Treatment �Tick removal �Improvement in hours

References � � � � � http: //www. cdc. gov/ticks/diseases/ Cline D, Ma OJ, et al. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 6 th edition. Mc. Graw-Hill, 2004 Dudley, J P (2010), “Tularemia: A Case Study In Medical Surveillance And Bioterrorism Preparedness”, JMed. CBR 8, 17 September 2010, http: //www. jmedcbr. org/issue_0801/Dudley_09_10. html. Halperin JJ. Prolonged Lyme disease treatment: enough is enough. Neurology 2008; 70: 986 http: //www. michigan. gov/emergingdiseases/0, 4579, 7 -186 -25890 -75870 --, 00. html. Accessed 9/27/15. Nadelman RB, Nowakowski J, Forseter G, et al. The clinical spectrum of early Lyme borreliosis in patients with culture-confirmed erythema migrans. Am J Med 1996; 100: 502 Rosen's emergency medicine: concepts and clinical practice 7 th edition. Philadelphia, PA: Mosby/Elsevier; 2010. Steere AC, Schoe RT, Taylor E. The clinical evolution of Lyme arthritis. Ann Intern Med 1987; 107: 725 Wolfson A, Hendey GW, et al. Harwood-Nuss’ Clinical Practice of Emergency Medicine, 5 th edition. Philadelphia: Lippincott Williams & Wilkins and Wolters Kluwer Business, 2010. Wormser GP. Clinical Practice Early Lyme Disease. N Engl J Med 1996; 354: 2794.
- Slides: 80